Type 1 hypersensitivity reactin mechanism
Reading File
Finding Sources
Searching the Web
Type 1 hypersensitivity reaction mechanism IgE mast cells
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to give a thorough, well-structured answer. Let me compile everything.
Type I Hypersensitivity Reaction - Mechanism
Type I hypersensitivity (immediate hypersensitivity) is an IgE-mediated allergic reaction that occurs within minutes of re-exposure to an antigen (allergen). It involves two key phases: sensitization and the effector (elicitation) phase.
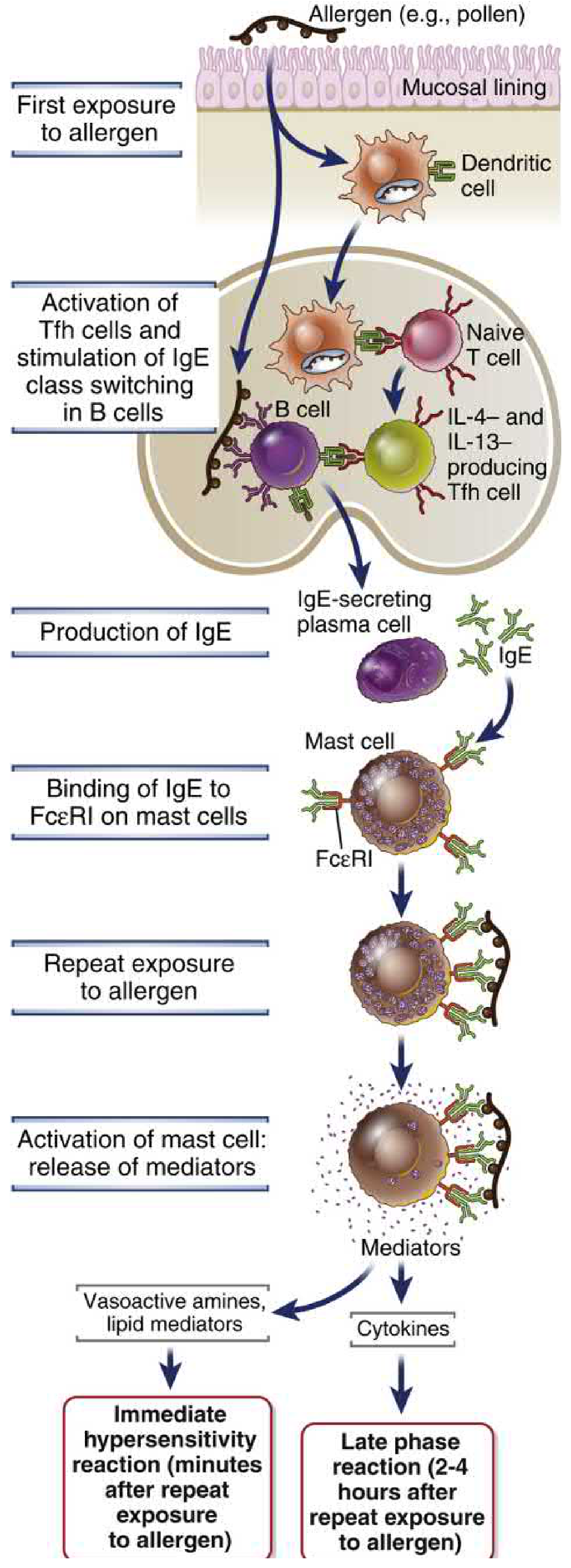
Phase 1: Sensitization (First Exposure)
This phase primes the immune system - no symptoms occur yet.
-
Allergen entry: Allergens (pollen, house dust mite proteins, food proteins, drugs) enter via mucosal surfaces and are captured by dendritic cells (DCs).
-
T cell polarization: DCs present allergen peptides to naive T cells, which differentiate into Th2 cells (and T follicular helper [Tfh] cells). Th2/Tfh cells produce IL-4 and IL-13.
-
IgE class switching: IL-4 and IL-13 act on allergen-specific B cells, promoting class-switch recombination from IgM/IgG to IgE production. Plasma cells then secrete large amounts of IgE.
-
Mast cell sensitization: IgE binds with extremely high affinity to FcεRI (Fc epsilon receptor type I) on tissue mast cells and circulating basophils. The mast cells are now "armed" - this is sensitization.
At this point the person is sensitized but asymptomatic.
Phase 2: Effector Phase (Re-exposure / Elicitation)
Re-exposure to the same allergen triggers the reaction.
-
Allergen cross-linking: The allergen binds to and cross-links two or more adjacent IgE molecules on the mast cell surface. This aggregates the FcεRI receptors.
-
Mast cell activation: Cross-linking of FcεRI activates intracellular signaling (Lyn kinase → Syk kinase → downstream phospholipase C pathway), leading to:
- Rise in intracellular Ca²+
- Degranulation - preformed granule contents released within seconds to minutes
Mediators Released
| Category | Mediator | Effect |
|---|---|---|
| Preformed (granules) | Histamine | Vasodilation, increased vascular permeability, smooth muscle contraction |
| Heparin | Anticoagulant | |
| Tryptase, chymase | Tissue remodeling, inflammation marker | |
| Serotonin | Vasoconstriction/dilation depending on site | |
| Newly synthesized lipid mediators | Prostaglandin D2 (PGD2) | Vasodilation, bronchoconstriction |
| Leukotrienes C4, D4, E4 | Prolonged bronchoconstriction, mucus secretion, increased vascular permeability | |
| PAF (platelet-activating factor) | Vasodilation, leukocyte chemotaxis | |
| Cytokines (produced on activation) | IL-4, IL-13 | Sustain Th2 responses, mucus secretion |
| IL-5 | Eosinophil recruitment and activation | |
| TNF, IL-3, MIP-1α | Late-phase inflammation |
- Cellular and Molecular Immunology, Table 20.2
Immediate vs. Late-Phase Reactions
-
Immediate reaction (within minutes): Driven by vasoactive amines (histamine) and lipid mediators - causes rapid vasodilation, bronchoconstriction, and mucus secretion.
-
Late-phase reaction (2-4 hours after re-exposure): Driven by cytokines (especially IL-4, IL-5, TNF) released by mast cells. These recruit eosinophils, neutrophils, and more Th2 cells, causing a prolonged inflammatory response.
Clinical Manifestations
Depending on the tissue involved:
- Systemic - Anaphylaxis (most severe - airway restriction + cardiovascular collapse)
- Respiratory - Allergic asthma, allergic rhinitis (hay fever)
- Skin - Urticaria (hives), angioedema, atopic dermatitis
- GI - Food allergy symptoms (abdominal pain, diarrhea)
- Eyes - Allergic conjunctivitis
Key diagnostic markers:
- Serum tryptase - elevated in anaphylaxis (peaks at ~1 hour; also chronically elevated in systemic mastocytosis)
- Plasma histamine - peaks rapidly (~10 minutes), returns to normal within 1 hour
- Urinary histamine - may remain elevated for 24 hours
- Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 1524-1525
- Cellular and Molecular Immunology (Abbas), 10th Ed., pp. 1302-1308
- Quick Compendium of Clinical Pathology, 5th Ed., p. 4360
Why NOT Type I: Important Distinctions
- Anaphylactoid reactions - clinically similar to anaphylaxis but NOT IgE-mediated (direct mast cell degranulation by drugs like morphine, radiocontrast media) - not true Type I hypersensitivity
- Hereditary angioedema - complement-mediated (C1 inhibitor deficiency) - not Type I
- Type II - antibody-mediated cytotoxicity (IgG/IgM on cell surfaces)
- Type III - immune complex-mediated (IgG + antigen complexes + complement)
- Type IV - delayed-type (T cell and macrophage mediated, 48-72 hrs)
Haptens
Finding Sources
Searching the Web
hapten immunology mechanism carrier protein immune response
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough, well-illustrated answer on haptens.
Haptens
Definition
A hapten is a small chemical molecule (typically <1 kDa) that is antigenic (can bind to a specific antibody) but not immunogenic by itself (cannot elicit an immune response alone). To become immunogenic, a hapten must be covalently coupled to a large carrier protein - this complex is called the hapten-carrier conjugate or immunogen.
The term comes from the Greek haptein ("to fasten"). The concept was first worked out using small molecules like m-aminobenzene sulfonate and dinitrophenol (DNP).
"Immunization with free hapten produces no antibodies to the hapten. However, immunization with hapten groups linked to a protein carrier generates antibodies that react with high affinity to hapten alone or linked to a molecule other than the carrier."
- Roitt's Essential Immunology
The Classic Demonstration
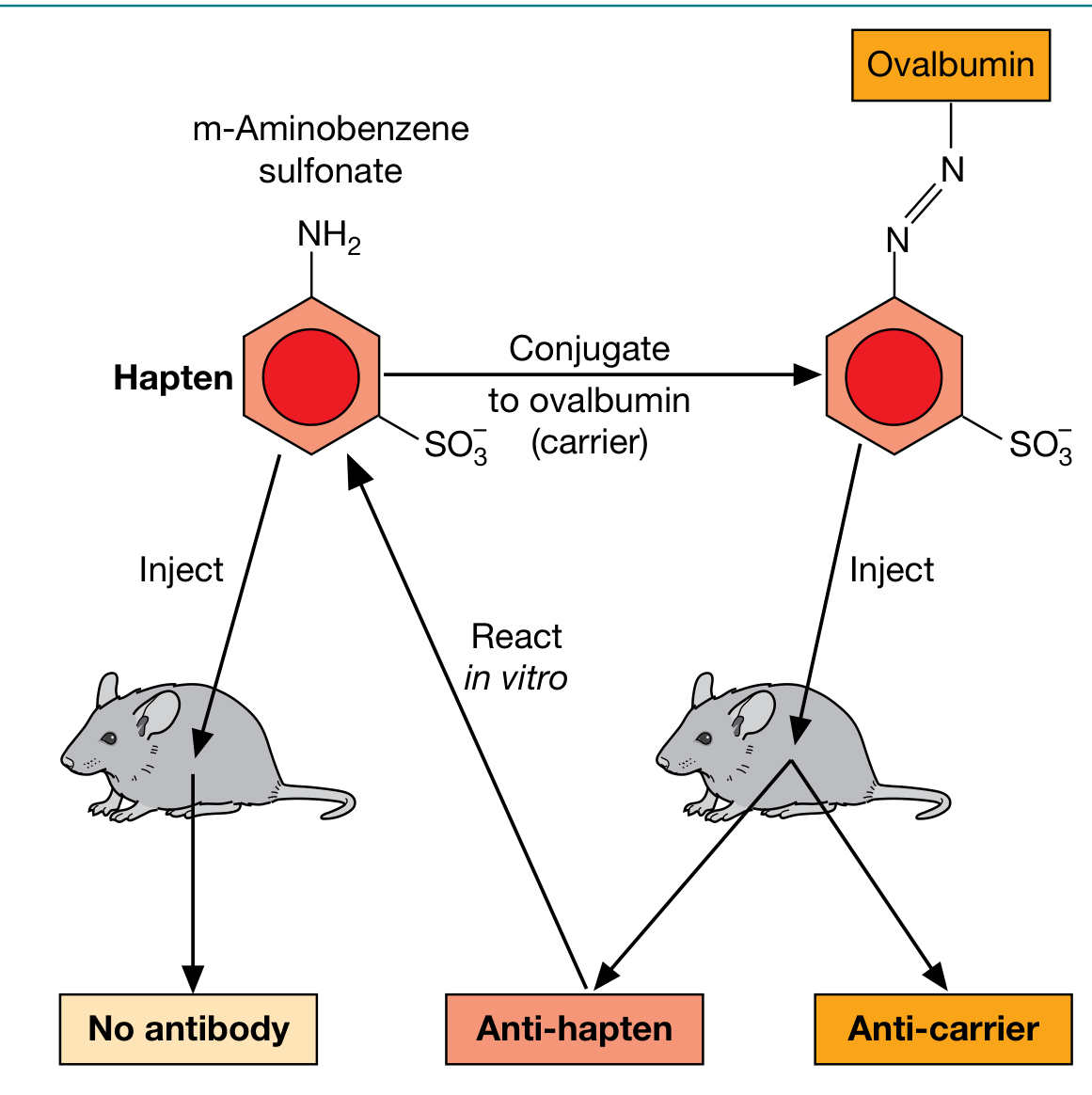
As shown above:
- Injecting a free hapten (e.g., m-aminobenzene sulfonate) alone → no antibody produced
- Injecting hapten conjugated to a carrier protein (e.g., ovalbumin) → produces anti-hapten AND anti-carrier antibodies
- The antibodies produced can then react with the free hapten in vitro
Why Haptens Alone Cannot Induce an Immune Response
The reason lies in the T cell-B cell collaboration required for a full humoral immune response:
A T cell-dependent B cell response requires two distinct epitopes on the same molecule:
| Role | Recognized by | Epitope type |
|---|---|---|
| Hapten | B cell (via BCR/membrane Ig) | Native conformational epitope |
| Carrier protein | CD4+ T helper cell (via class II MHC) | Linear peptide epitope |
A hapten alone is too small to be processed into peptides and presented on MHC class II - so it cannot activate T helper cells. Without T cell help, B cells cannot undergo full activation, class switching, affinity maturation, or plasma cell differentiation.
Three Key Rules of the Hapten-Carrier Effect (Abbas, Cellular & Molecular Immunology)
- Both hapten-specific B cells AND carrier-specific T helper cells are required - the response is T cell-dependent
- Hapten and carrier must be physically linked - administering them separately cannot induce an anti-hapten response. The hapten is responsible for the efficient internalization of the carrier protein into the B cell
- The interaction is MHC class II-restricted - helper T cells cooperate only with B cells that express the same class II MHC molecules involved in the initial T cell activation by dendritic cells
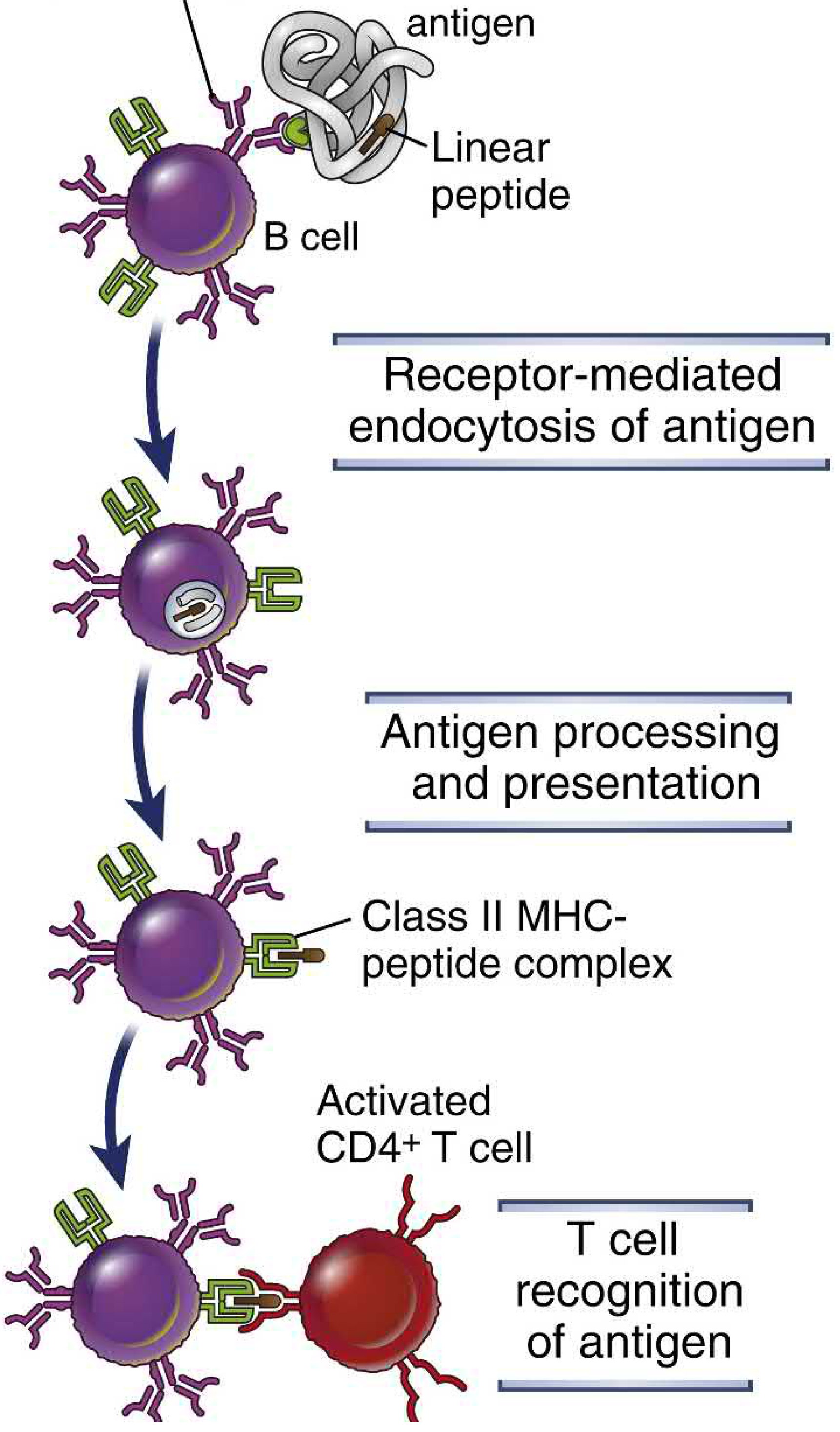
Mechanism Step-by-Step
- Hapten-carrier conjugate enters the body
- Hapten-specific B cell binds the conjugate via its BCR (recognizing the hapten epitope)
- The B cell endocytoses the entire hapten-carrier conjugate
- The carrier protein is proteolytically processed inside the B cell into linear peptides
- These peptides are loaded onto class II MHC molecules and displayed on the B cell surface
- A carrier-specific CD4+ T cell (Th cell) recognizes the class II MHC-peptide complex
- T cell delivers help via CD40L-CD40 interaction + cytokines (IL-4, IL-21)
- B cell activates, proliferates, undergoes isotype switching, and differentiates into plasma cells secreting anti-hapten antibodies
Clinical Relevance
Drug allergies are the most important clinical application of hapten biology:
| Drug | Mechanism |
|---|---|
| Penicillin | The reactive β-lactam ring covalently binds to carrier proteins, forming a hapten. This is why ~10% of penicillin-allergic patients also react to cephalosporins (cross-reactive haptens) |
| Cephalosporins | Similar β-lactam haptenization |
| Tetracyclines, Tolbutamide | Hapten/drug adsorption mechanism |
Drug-induced immune hemolytic anemia uses the hapten mechanism:
- Drugs like penicillin bind to RBC membranes (haptenize them)
- Anti-drug IgG antibodies then coat the RBCs → complement activation → hemolysis (Type II hypersensitivity)
Application: Conjugate Vaccines
The hapten-carrier concept is the basis for conjugate vaccines against encapsulated bacteria:
- Polysaccharide capsule antigens (equivalent to haptens - recognized by B cells but T cell-independent and weak in infants) are covalently linked to carrier proteins (e.g., tetanus toxoid, CRM197)
- This converts the weak T-independent polysaccharide response into a strong T-dependent response with isotype switching, affinity maturation, and immunologic memory
- Examples: Hib (H. influenzae type b), PCV (pneumococcal), MCV (meningococcal) vaccines
- Cellular and Molecular Immunology (Abbas), 10th Ed., pp. 769-771
- Roitt's Essential Immunology, p. 163
- The Washington Manual of Medical Therapeutics, p. 1215
This is a shared conversation. Sign in to Orris to start your own chat.