Teach me cornea for neet pg 2026 based on PREVIOUS YEAR TOPICS
Reading File
Finding Sources
Searching the Web
NEET PG 2025 2024 2023 ophthalmology cornea previous year questions topics
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have everything needed to compile a comprehensive, PYQ-focused NEET PG 2026 cornea guide. Let me write it out.
🔬 CORNEA for NEET PG 2026 - Based on Previous Year Question Trends
PYQ Trend Analysis (2023-2025): Cornea typically contributes 2 questions per exam. High-yield topics in recent years: Fuchs endothelial dystrophy, Keratoconus (INTACS image), HSV keratitis (dendritic ulcer), corneal layers, Acanthamoeba keratitis. Image-based questions are now standard.
TOPIC 1: CORNEAL LAYERS - MUST KNOW (Repeated in PYQs)
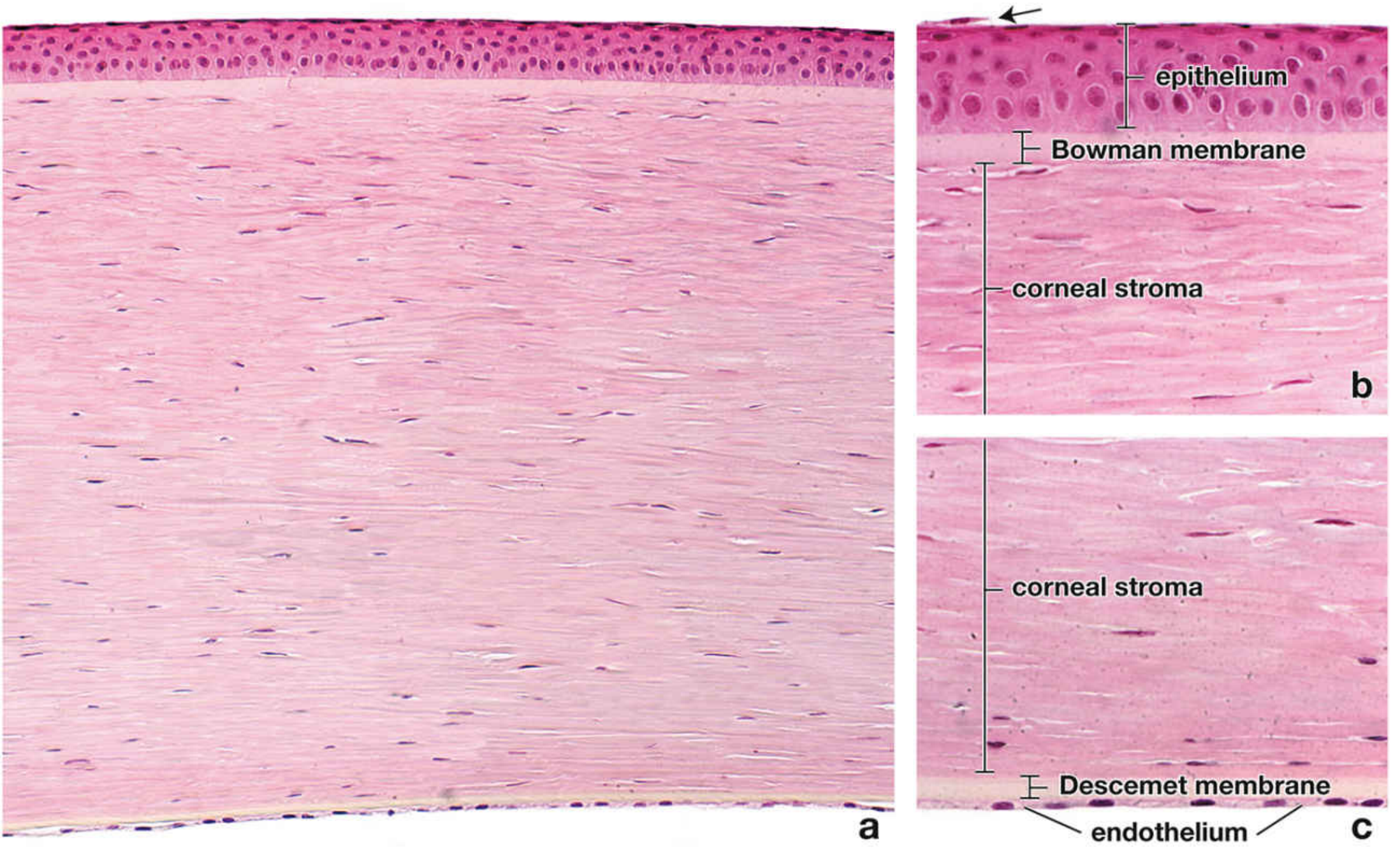
The cornea has 5 layers (3 cellular + 2 acellular):
| Layer | Key Features | High-Yield Facts |
|---|---|---|
| 1. Epithelium | Non-keratinized stratified squamous, ~5 cell layers, ~50 µm thick | Regenerates in ~7 days; continuous with conjunctival epithelium |
| 2. Bowman membrane | Acellular, anterior basement membrane | Does NOT regenerate if destroyed - scar forms |
| 3. Stroma | Thickest layer (~90% of corneal thickness); collagen lamellae + keratocytes | Avascular; collagen type I; 0.5 mm center, 1 mm periphery |
| 4. Descemet membrane | Acellular, posterior basement membrane of endothelium | PAS-positive; most resistant layer; thickens with age |
| 5. Endothelium | Single layer of hexagonal cells; Na-K ATPase pump | Most metabolically active; DOES NOT regenerate - cell count decreases with age |
Memory trick: "Every Bloody Student Dreams Easily" - Epithelium, Bowman, Stroma, Descemet, Endothelium
Key one-liners for MCQs:
-
Most resistant layer = Descemet membrane
-
Thickest layer = Stroma
-
Most metabolically active layer = Endothelium (Na-K ATPase pump keeps stroma dehydrated)
-
Layer that does NOT regenerate = Bowman membrane (scarring occurs)
-
Maintains corneal clarity by active dehydration = Endothelium
-
Histology A Text and Atlas, p. 2379
TOPIC 2: FUCHS ENDOTHELIAL CORNEAL DYSTROPHY ⭐⭐⭐ (NEET PG 2025 - Direct Q)
PYQ 2025: "Patient with guttate lesions in one eye and bullous keratopathy in the other" = Fuchs endothelial dystrophy
Key Facts:
- Bilateral accelerated endothelial cell loss
- More common in women; onset in middle age or later
- Associated with slightly increased risk of glaucoma
- Inheritance: Mostly sporadic; AD inheritance possible; mutation in COL8A2 (early-onset variant) or TCF4 gene (most cases)
Pathology (in order of progression):
- Cornea guttata - irregular wart-like excrescences on Descemet membrane secreted by abnormal endothelial cells (earliest sign)
- Specular reflection = tiny dark spots → "beaten metal" appearance
- Central stromal edema → blurred vision worse in morning (corneal dehydration overnight fails)
- Epithelial edema → microcysts and bullae (bullous keratopathy)
- Rupture of bullae = severe acute pain (exposure of nerve fibers)
- Subepithelial scarring + peripheral vascularization (end-stage)
Treatment:
- Conservative: Topical NaCl 5% drops/ointment (hyperosmotic dehydration), hair dryer for corneal dehydration, reduce IOP
- Surgical: DSAEK (Descemet stripping automated endothelial keratoplasty) or DMEK - gold standard
- Bullae relief = bandage contact lenses + cycloplegia + antibiotic ointment
Exam trap: Cataract surgery worsens Fuchs dystrophy - endothelial cell loss from phaco. Always screen preoperatively.
- Kanski's Clinical Ophthalmology 10th, p. 260
TOPIC 3: KERATOCONUS ⭐⭐⭐ (NEET PG 2025 Image Q - INTACS)
PYQ 2025: Image showing a ring in the cornea = INTACS (Intracorneal Ring Segments) = treatment for Keratoconus
Definition:
Progressive central/paracentral corneal stromal thinning + apical protrusion + irregular astigmatism. Prevalence: 0.1-0.2%.
Key Association Facts (MCQ-favorite):
- Onset: teens to twenties, more in males
- Associations: Down syndrome, Ehlers-Danlos, Marfan, Osteogenesis imperfecta
- Ocular associations: Vernal keratoconjunctivitis, Leber congenital amaurosis, Retinitis pigmentosa, Aniridia
- Risk factors: Allergy, asthma, eczema, eye rubbing (persistent)
- ~50% of normal fellow eyes develop KC within 16 years
Signs (Know all):
| Sign | Description |
|---|---|
| Oil droplet reflex | Distant direct ophthalmoscopy at 0.5m |
| Scissor reflex | Retinoscopy |
| Munson sign | V-shaped indentation of lower lid on downgaze |
| Vogt's striae | Fine vertical stress lines in deep stroma |
| Fleischer ring | Iron (hemosiderin) deposition at base of cone (slit lamp with cobalt blue filter) |
| Rizzuti sign | Sharply focused beam near nasal limbus when light directed from temporal side |
Grading (Keratometry):
- Mild: <48 D
- Moderate: 48-54 D
- Severe: >54 D
Acute Hydrops:
Rupture of Descemet membrane → sudden corneal edema → acute vision loss. Munson sign may appear. Heals with scarring in 6-10 weeks.
Treatment Ladder:
- Spectacles (mild)
- Contact lenses (moderate)
- Corneal collagen cross-linking (CXL) - halts progression (riboflavin + UV-A; epithelium removed)
- INTACS (Intracorneal ring segment implantation) - image-based Q in NEET PG 2025
- DALK (Deep anterior lamellar keratoplasty) or PKP (Penetrating keratoplasty) - severe
Important: LASIK is absolutely contraindicated in keratoconus. History of hydrops = contraindication to DALK.
- Kanski's Clinical Ophthalmology 10th, p. 265-270
TOPIC 4: HERPES SIMPLEX KERATITIS ⭐⭐⭐
Repeatedly asked across NEET PG, AIIMS, INI CET
Key Facts:
- Most common infectious cause of corneal blindness in developed countries
- Up to 60% of corneal ulcers in developing countries may be HSV
- HSV-1: above waist (face, lips, eyes); HSV-2: genital (rarely ocular)
- Virus latent in trigeminal ganglion; reactivation triggers = fever, UV radiation, hormonal change, trauma, immunosuppression
Types of HSV Keratitis:
1. Epithelial Keratitis (Active virus replication):
- Starts as stellate/coarse punctate epithelial opacification
- Progresses to dendritic ulcer - linear branching with terminal buds (pathognomonic)
- Ulcer bed stains with fluorescein; margins stain with rose Bengal (virus-laden cells)
- Reduced corneal sensation (key feature)
- Geographic/amoeboid ulcer = if topical steroids used inadvertently (enlargement)
- Treatment: Topical acyclovir 3% ointment 5x/day OR topical ganciclovir; NOT steroids
2. Disciform (Stromal Immune) Keratitis:
- Central disc-shaped stromal edema
- Keratic precipitates (KPs) in area of edema
- Corneal vascularization in late/severe cases
- Treatment: Topical steroids + antiviral cover (to suppress immune reaction, not active virus)
3. Necrotizing Stromal Keratitis:
- Direct viral invasion of stroma
- Severe inflammatory response, tissue necrosis
- Treat with antivirals + judicious steroids
4. Neurotrophic Keratopathy:
- Due to loss of corneal sensation
- Persistent epithelial defects, oval or round (NOT branching - important differentiation)
Exam trap: Topical steroids + dendritic ulcer = geographic ulcer. NEVER use steroids in active epithelial HSV keratitis.
- Kanski's Clinical Ophthalmology 10th, p. 220-225
TOPIC 5: ACANTHAMOEBA KERATITIS ⭐⭐
Classic PYQ association: Contact lens + severe pain disproportionate to signs
Key Facts:
- Protozoan, ubiquitous in environment (tap water, soil)
- Classic history: Soft contact lens wear + poor lens hygiene (using tap water, infrequent disinfection)
- Most painful keratitis - pain out of proportion to clinical signs
- Perineural invasion on slit lamp = pathognomonic (ring infiltrate around corneal nerves)
- Ring infiltrate in mid-stroma = classic finding
Treatment:
- PHMB (Polyhexamethylene biguanide) + propamidine isethionate (Brolene)
- Long duration (months) needed
- Corneal transplant for severe scarring
TOPIC 6: INTERSTITIAL KERATITIS
| Feature | Syphilitic IK | Cogan Syndrome |
|---|---|---|
| Cause | Congenital syphilis (Treponema) | Autoimmune (ANCA-associated) |
| Age | 5-20 years (congenital syphilis) | Young adults |
| Cornea | Deep stromal vascularization; "salmon patch" | Peripheral stromal infiltrates |
| Ghost vessels | Yes - after treatment | - |
| Systemic | Deafness, Hutchinson teeth (Hutchinson's triad) | Sensorineural deafness, vestibular dysfunction |
| Treatment | Penicillin + topical steroids | Systemic steroids |
TOPIC 7: CORNEAL DYSTROPHIES - Quick Overview
Classification by layer (IC3D):
Epithelial Layer:
- Map-dot-fingerprint (Cogan microcystic) - most common epithelial dystrophy; recurrent erosions
Bowman Layer:
- Reis-Bucklers - bilateral, progressive; replaces Bowman layer with fibrous tissue; early onset, painful erosions
Stromal Dystrophies:
| Dystrophy | Appearance | Deposits | Staining |
|---|---|---|---|
| Granular (BIGH3 gene) | Discrete breadcrumb-like opacities; clear zones between opacities | Hyaline | Masson trichome (red) |
| Lattice | Refractile lattice lines; amyloid deposits | Amyloid | Congo red (birefringent) |
| Macular | Most severe; opacities involve entire stroma including periphery | Glycosaminoglycans (keratan sulfate) | Alcian blue |
| Schnyder | Central discoid opacity; corneal arcus; hypercholesterolemia | Cholesterol crystals | Oil Red O |
Memory trick for stromal dystrophies (clarity of clear intervals): Granular > Lattice > Macular (Granular has clearest intervals between opacities, Macular has no clear areas)
Endothelial Layer:
-
Fuchs endothelial dystrophy (see above - NEET PG 2025)
-
Kanski's Clinical Ophthalmology 10th, p. 254-260
TOPIC 8: CORNEAL DEGENERATIONS
| Condition | Key Feature | Cause/Association |
|---|---|---|
| Arcus senilis | White ring at limbus (clear gap between arcus & limbus) | Lipid deposit; normal in elderly; in young = hypercholesterolemia |
| Band keratopathy | Horizontal calcium band at Bowman layer (interpalpebral zone) | Hypercalcemia, chronic uveitis, JIA, Still's disease |
| Spheroidal degeneration | Amber/golden deposits; exposed areas | UV radiation, dry climate (climatic droplet keratopathy) |
| Salzmann nodular | Bluish-white elevated nodules | Post-inflammatory (trachoma, phlyctenulosis) |
| Terrien marginal degeneration | Superior peripheral thinning, with lipid leading edge; vascularized; NO ulceration | Unknown |
| Coat's white ring | Small white ring; iron deposits | Previous metallic foreign body |
Wilson's Disease Corneal Finding:
Kayser-Fleischer ring = copper deposition in Descemet membrane at periphery; starts superiorly > inferiorly; seen in hepatolenticular degeneration
TOPIC 9: CORNEAL ULCERS - Comparison Table ⭐
| Feature | Bacterial | Fungal | HSV | Acanthamoeba |
|---|---|---|---|---|
| Onset | Acute | Subacute/chronic | Acute | Subacute |
| Pain | Moderate-severe | Mild-moderate | Mild-moderate | Severe (disproportionate) |
| Appearance | Dense stromal infiltrate, hypopyon | Feathery margins, satellite lesions, hypopyon | Dendritic/geographic | Ring infiltrate, perineural |
| Association | Trauma, CL | Trauma (vegetative matter), immunosuppression | Recurrent, fever | Contact lens, water exposure |
| Rx | Fluoroquinolones (ciprofloxacin/moxifloxacin) | Natamycin (1st line), Voriconazole | Topical acyclovir/ganciclovir | PHMB + Brolene |
TOPIC 10: CORNEAL TRANSPLANT (Keratoplasty)
| Type | Layers Transplanted | Indication |
|---|---|---|
| PKP (Penetrating) | Full thickness | Advanced keratoconus, corneal scar |
| DALK (Deep anterior lamellar) | All layers except Descemet + endothelium | Keratoconus, stromal scars (endothelium healthy) |
| DSAEK | Descemet + endothelium + thin stroma | Fuchs dystrophy, bullous keratopathy |
| DMEK | Descemet + endothelium only | Fuchs dystrophy (best visual outcome) |
| KLAL | Limbal + corneal tissue | Limbal stem cell deficiency |
Key: DALK is contraindicated if Descemet membrane is diseased or post-hydrops (discontinuous Descemet).
QUICK REVISION - HIGH-YIELD ONE-LINERS FOR NEET PG 2026
| Fact | Answer |
|---|---|
| Most common corneal dystrophy | Map-dot-fingerprint (epithelial) |
| Most common infectious cause of corneal blindness (developed countries) | HSV |
| Cornea guttata = | Fuchs endothelial dystrophy (excrescences on Descemet by abnormal endothelium) |
| "Beaten metal" appearance on specular microscopy | Fuchs endothelial dystrophy |
| Oil droplet reflex on retinoscopy | Keratoconus |
| Munson sign + Vogt's striae + Fleischer ring | Keratoconus |
| Dendritic ulcer stains with | Fluorescein (bed) + Rose Bengal (margins) |
| INTACS is used for | Keratoconus |
| CXL (Corneal collagen cross-linking) halts | Keratoconus progression |
| LASIK contraindicated in | Keratoconus |
| Most painful keratitis | Acanthamoeba |
| Perineural invasion on slit lamp | Acanthamoeba keratitis |
| KF ring location starts | Superiorly (Descemet membrane) in Wilson's disease |
| Corneal deposit in Wilson's disease | Kayser-Fleischer ring (copper in Descemet) |
| Calcium deposition at Bowman layer | Band keratopathy |
| Most resistant layer of cornea | Descemet membrane |
| Stroma constitutes what % of corneal thickness | 90% |
| Layer that does NOT regenerate if destroyed | Bowman membrane |
| Symptomatic Fuchs is worse when | Morning (overnight dew point causes edema) |
| Treatment of choice for Fuchs | DMEK (best), DSAEK |
| Interstitial keratitis + deafness + Hutchinson teeth | Congenital syphilis (Hutchinson's triad) |
| Granular dystrophy stains | Red with Masson trichrome (hyaline) |
| Lattice dystrophy stains | Congo red (amyloid, birefringent) |
| Macular dystrophy stains | Alcian blue (GAGs/keratan sulfate) |
PYQ-BASED PRACTICE QUESTIONS
Q1 (NEET PG 2025): A patient presents with guttate lesions in one eye and bullous keratopathy in the other eye. Most probable diagnosis?
A: Fuchs endothelial dystrophy
Q2 (NEET PG 2025 - Image): A ring visible inside the cornea used to treat which condition?
A: Keratoconus (INTACS = Intracorneal ring segments)
Q3: A 25-year-old contact lens wearer presents with extremely painful red eye disproportionate to signs, with ring infiltrate on slit lamp. Diagnosis?
A: Acanthamoeba keratitis
Q4: A patient with dendritic corneal ulcer was inadvertently given topical steroids. The ulcer transformed to a geographic shape. This is because?
A: Topical steroids promote viral replication, enlarging HSV epithelial ulcer to geographic/amoeboid pattern
Q5: Which corneal dystrophy deposit stains with Congo red?
A: Lattice dystrophy (amyloid deposits)
Q6: The most metabolically active layer of cornea is?
A: Endothelium (Na-K ATPase pump activity)
Q7: Which layer of cornea does NOT regenerate?
A: Bowman membrane (replaced by fibrous scar)
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach 10th Edition; Histology: A Text and Atlas (Pawlina & Ross); Junqueira's Basic Histology 17e; NEET PG 2025 PYQs (DocTutorials/OnCourse AI).
This is a shared conversation. Sign in to Orris to start your own chat.