intestional absorption anatomy, physiology,pathology and medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"intestinal absorption" AND "nutrient transport"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete answer.
Intestinal Absorption: Anatomy, Physiology, Pathology & Medicine
1. ANATOMY
Gross Structure
The small intestine - the primary absorptive organ - is divided into duodenum, jejunum, and ileum. Its internal surface area is amplified by three structural adaptations that increase absorptive surface roughly 600-fold:
- Plicae circulares (valvulae conniventes) - circular folds of mucosa and submucosa, most prominent in the jejunum
- Villi - finger-like projections of the mucosa (~0.5-1.5 mm), covered by columnar absorptive cells (enterocytes) and goblet cells
- Microvilli (brush border) - dense projections on the apical surface of enterocytes; each cell has ~1,000 microvilli, forming the "brush border"
The Enterocyte (Absorptive Cell)
Enterocytes are polarized epithelial cells with two distinct membrane domains:
- Apical (brush border) membrane (BBM) - faces the lumen; site of digestive enzymes (lactase, sucrase, peptidases) and nutrient transporters
- Basolateral membrane (BLM) - faces blood/lymph; site of exit transporters that deliver absorbed nutrients to the portal circulation or lacteals
Crypt-Villus Axis
- Crypt cells (of Lieberkuhn) - secrete fluid and electrolytes; home to stem cells
- Villus cells - absorb fluid and nutrients
- Tight junctions between cells can be "leaky" (jejunum/ileum) allowing paracellular movement, or "tight" (colon) restricting paracellular flow
Segment-Specific Features
| Segment | Key Absorptive Roles |
|---|---|
| Duodenum | Iron, calcium, water-soluble vitamins; site of highest gluten exposure |
| Jejunum | Carbohydrates, proteins, fats, most water-soluble vitamins; dominant Na+ absorption |
| Ileum | Bile acid reabsorption (terminal ileum - essential for fat-soluble vitamin recycling), vitamin B12-intrinsic factor complex, remaining electrolytes |
| Colon | Water, Na+ (aldosterone-regulated), K+ secretion; short-chain fatty acid absorption |
2. PHYSIOLOGY
Fluid and Electrolyte Absorption
The intestine processes ~8-9 L of fluid daily (2 L dietary + 7 L secretions). Nearly all is absorbed, with only ~200 mL lost in stool. Absorption is always isosmotic - solute and water are absorbed proportionally, analogous to the renal proximal tubule.
The mechanism of absorption differs by segment:
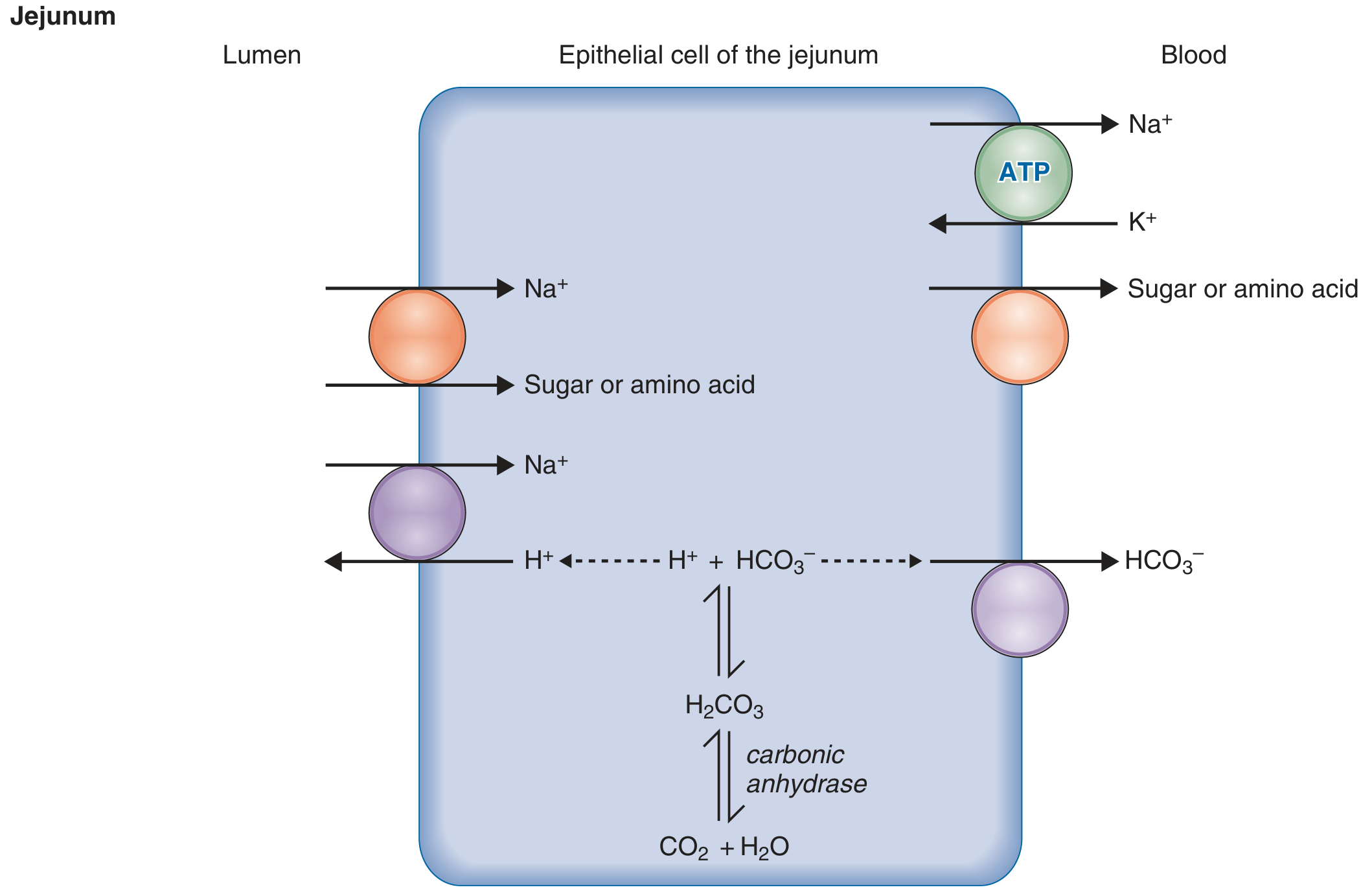
Jejunum - Na+ enters epithelial cells via:
- Na+-glucose cotransporters (SGLT1)
- Na+-amino acid cotransporters
- Na+-H+ exchange (driven by carbonic anhydrase)
- Na+-K+ ATPase on the basolateral membrane extrudes Na+ into blood, maintaining the inward gradient
- Net result: absorption of NaHCO₃ + sugars + amino acids
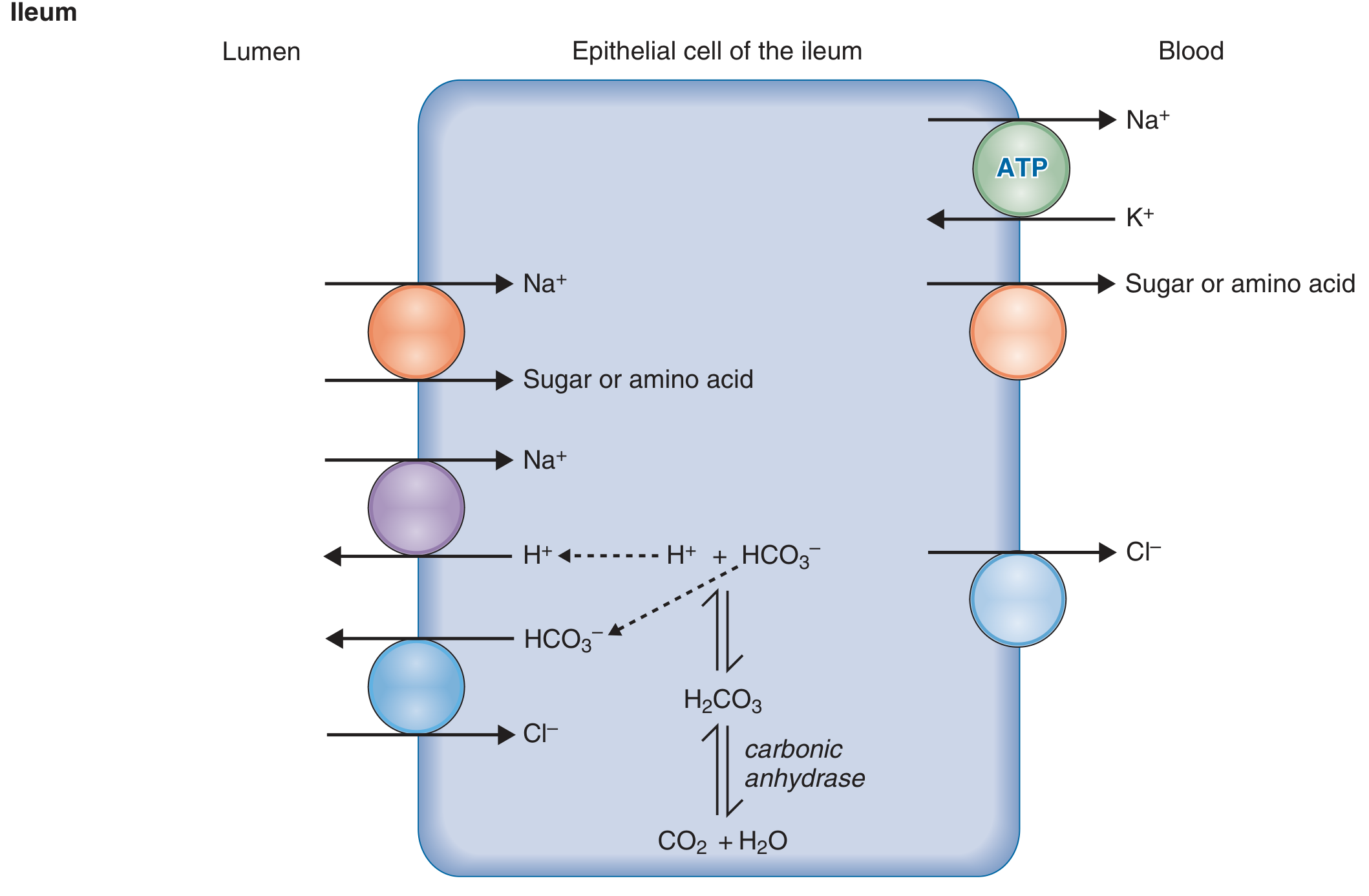
Ileum - All jejunal mechanisms plus:
- Cl⁻-HCO₃⁻ exchange in the apical membrane
- Cl⁻ transporter (instead of HCO₃⁻) in the basolateral membrane
- Net result: NaCl absorption (H+ secreted to lumen; HCO₃⁻ also secreted to lumen via the apical exchanger)
Colon - Principal cells analogous to renal collecting duct:
- Apical Na+ channels (ENaC) and K+ channels
- Na+ absorption is aldosterone-induced
- Aldosterone increases ENaC expression → increased Na+ entry → increased basolateral Na+-K+ ATPase activity → K+ secretion
- In diarrhea, high flow rate increases colonic K+ secretion → fecal K+ loss → hypokalemia
Nutrient-Specific Absorption Mechanisms
Carbohydrates
- Starch digested by salivary and pancreatic amylase to oligosaccharides, then by brush-border disaccharidases (lactase, sucrase-isomaltase, maltase) to monosaccharides
- Glucose & galactose: absorbed by SGLT1 (Na+-dependent cotransporter, apical) → exit via GLUT2 (basolateral)
- Fructose: absorbed via GLUT5 (facilitated diffusion, apical) → exits via GLUT2 (basolateral)
Proteins
- Gastric pepsin + pancreatic proteases (trypsin, chymotrypsin, elastase, carboxypeptidases) → oligopeptides and amino acids
- Brush-border peptidases complete digestion
- Di- and tripeptides absorbed via PepT1 (H+-dependent cotransporter, apical) - actually more efficient than free amino acid transport
- Free amino acids absorbed via specific Na+-dependent amino acid transporters
- Hartnup syndrome = defect in neutral amino acid transporter → tryptophan malabsorption → niacin deficiency
Lipids
- Pancreatic lipase + colipase hydrolyze triglycerides to 2-monoglycerides + fatty acids
- Products emulsify with bile salts and phospholipids to form mixed micelles - the vehicle for lipid transport to the brush border
- At the BBM, fatty acids and monoglycerides diffuse passively into the enterocyte
- Inside the cell, they are re-esterified in the smooth ER to triglycerides, packaged into chylomicrons with apolipoproteins
- Chylomicrons exit via exocytosis at the basolateral membrane → enter lacteals (lymphatics) → thoracic duct → systemic circulation
- Optimal luminal pH for micelle formation: 6-8 (requires pancreatic HCO₃⁻ to neutralize gastric acid)
- Medium-chain fatty acids bypass this system and absorb directly into portal blood
Iron
- Dietary iron is either heme (from meat) or non-heme (Fe³+)
- Fe³+ is reduced to Fe²+ by duodenal cytochrome B (Dcytb) on the brush border
- Fe²+ enters via DMT1 (divalent metal transporter 1) on the apical membrane
- Exported via ferroportin on the basolateral membrane
- Regulated by hepcidin (liver-produced hormone): hepcidin ↑ → ferroportin degradation → iron trapping in enterocytes
- Absorbed primarily in the duodenum and proximal jejunum
Vitamin B12 (Cobalamin)
- Binds intrinsic factor (IF) secreted by gastric parietal cells
- B12-IF complex binds cubilin receptors in the terminal ileum → endocytosis
- B12 deficiency results from: pernicious anemia (lack of IF), terminal ileum resection/disease, or bacterial overgrowth (bacteria consume B12)
Water-Soluble Vitamins
- Most absorbed via specific Na+-dependent transporters or carrier-mediated mechanisms at the brush border
- Key transporters (per Sleisenger & Fordtran's):
- Vitamin C: SVCT-1 (Na+-dependent) at the apical membrane
- Thiamine: THTR-1, THTR-2 (Na+-dependent)
- Riboflavin: RFT-1, RFT-2
- Folate: PCFT (proton-coupled folate transporter) + RFC (reduced folate carrier)
- Biotin, pantothenic acid: SMVT (Na+-dependent multivitamin transporter)
- DHAA (oxidized vitamin C): absorbed via GLUT1, GLUT3, GLUT4 (glucose transporters) - competitively inhibited by glucose
Calcium
- Absorbed by two routes:
- Transcellular: vitamin D (1,25-dihydroxyvitamin D3) activates calbindin synthesis → facilitates Ca²+ movement through enterocyte → exported by Ca²+-ATPase (PMCA1b) at basolateral membrane
- Paracellular: passive, concentration-dependent, occurs throughout small intestine
- Primary site: duodenum and proximal jejunum
Intestinal Secretion (Counterpart to Absorption)
- Crypt cells secrete Cl⁻ via apical CFTR channels
- Basolateral NKCC1 cotransporter loads Cl⁻ into the cell
- Cl⁻ secretion drives Na+ (paracellular) and water into the lumen
- Normally balanced by villus absorption
- Secretion activated by cAMP (ACh, VIP, cholera toxin) or cGMP (heat-stable E. coli enterotoxin)
- Cholera: Vibrio cholerae toxin permanently activates adenylyl cyclase → massive cAMP → maximal Cl⁻ secretion → overwhelms absorptive capacity → life-threatening secretory diarrhea
3. PATHOLOGY
Classification of Malabsorption
Malabsorption can be classified by the mechanism affected:
| Mechanism | Example Diseases |
|---|---|
| Impaired intraluminal digestion | Pancreatic exocrine insufficiency, bile acid deficiency |
| Impaired mixing | Post-gastrectomy (Billroth II), gastrojejunostomy |
| Mucosal malabsorption | Celiac disease, tropical sprue, Crohn's disease, autoimmune enteropathy |
| Lymphatic obstruction | Primary intestinal lymphangiectasia, lymphoma |
| Infection | Giardia, Whipple's disease, bacterial overgrowth |
Steatorrhea (fatty stools) is the cardinal sign of significant malabsorption because fat is the nutrient most difficult to absorb - it requires the most processing steps.
Celiac Disease (Gluten-Sensitive Enteropathy)
Epidemiology: 0.6-1% worldwide; rising incidence for unclear reasons.
Pathogenesis (from Robbins & Kumar):
- Triggered by gluten (wheat, rye, barley) in genetically predisposed individuals (HLA-DQ2 in ~90%, HLA-DQ8 in most of the rest)
- Gluten peptides are deamidated by tissue transglutaminase 2 (TG2) → negatively charged peptides bind HLA-DQ2/8 on antigen-presenting cells → activation of gluten-specific CD4+ T cells → IFN-γ, IL-21, IL-2 production
- Gluten-TG2 complexes → anti-TG2 IgA plasma cells (up to 20% of all intestinal plasma cells in active disease)
- CD4+ T cells + IL-15 → expansion of intraepithelial CD8+ cytotoxic T cells expressing NKG2D/NKG2C → attack epithelial cells via interaction with HLA-E and MICA
Morphology (Marsh classification):
- Intraepithelial lymphocytosis (CD8+ T cells in the villous epithelium - most sensitive finding)
- Crypt hyperplasia (increased mitotic activity)
- Villous atrophy - loss of absorptive surface → malabsorption
- Loss of brush-border surface area + impaired enterocyte differentiation → reduced terminal digestion and transepithelial transport
- Increased plasma cells, mast cells, and eosinophils in the lamina propria
- Most pronounced in the second duodenum and proximal jejunum (highest gluten exposure)
Serology: Anti-TG2 IgA (most sensitive), anti-endomysial IgA; check total IgA (IgA deficiency gives false negatives - use IgG anti-TG2 instead)
Clinical features:
- Classic: diarrhea, steatorrhea, weight loss, abdominal distention, failure to thrive (children)
- Non-classic: iron deficiency anemia, osteoporosis, infertility, neurologic symptoms (ataxia, neuropathy), dermatitis herpetiformis
- Silent: positive serology + villous atrophy without symptoms
Complications: Enteropathy-associated T-cell lymphoma (EATL), small intestinal adenocarcinoma, refractory sprue (loss of response to gluten-free diet)
Treatment: Gluten-free diet - the only established treatment; restores histology in 6-24 months, reduces risk of lymphoma, anemia, osteoporosis, infertility
Bacterial Overgrowth Syndrome
Pathophysiology (from Goldman-Cecil Medicine):
- Normally, motility and gastric acid limit bacteria in the upper small bowel
- Any condition causing local stasis allows a "colonic" flora (coliforms, Bacteroides, Clostridium) to colonize the small intestine
- Anaerobic bacteria deconjugate bile salts → unconjugated bile salts absorbed passively (high pKa) → bile salt concentration falls below critical micellar concentration → fat and fat-soluble vitamin malabsorption
- Bacteria also: consume vitamin B12, release proteases that degrade brush-border disaccharidases → carbohydrate malabsorption
- Bacteria synthesize folate → serum folate normal or high (distinguishes from tropical sprue, where both B12 and folate are low)
Predisposing conditions: Elderly, post-surgical blind loops, strictures, multiple jejunal diverticula, abnormal motility (scleroderma, diabetes)
Diagnosis: >10³ CFU/mL on small intestinal aspirate culture (gold standard); glucose hydrogen/methane breath tests (noninvasive)
Treatment:
- Rifaximin 400 mg orally three times daily
- Alternatives: tetracycline, doxycycline, ciprofloxacin, amoxicillin-clavulanic acid, metronidazole
- Prokinetics for dysmotility: prucalopride, metoclopramide, erythromycin
- Octreotide (50 µg SC daily) for scleroderma-related overgrowth
Crohn's Disease and Malabsorption
- Diarrhea/malabsorption mechanisms include: (1) bacterial overgrowth from obstruction or fistulization, (2) bile acid malabsorption from terminal ileal disease/resection, (3) intestinal inflammation → decreased water and electrolyte absorption, and (4) protein-losing enteropathy
- Bile salt diarrhea (cholerheic diarrhea): unconjugated bile salts reach the colon → secretory diarrhea; treated with cholestyramine
Pancreatic Exocrine Insufficiency
- Lack of lipase, protease, and amylase → impaired intraluminal digestion
- Common causes: chronic pancreatitis, cystic fibrosis, pancreatic cancer
- Treatment: pancreatic enzyme replacement therapy (PERT)
Lactase Deficiency
- Most common cause of selective carbohydrate malabsorption worldwide (primary lactase non-persistence in adults)
- Unabsorbed lactose → osmotic diarrhea + fermentation by colonic bacteria → gas, bloating, cramping
- Diagnosis: hydrogen breath test after lactose load
4. CLINICAL MEDICINE
Approach to Malabsorption
Steatorrhea (>7 g fat/day on 100 g/day fat diet) is the most sensitive screening test. A systematic approach:
- History: prior surgery, alcohol use, travel, family history, medications (orlistat causes malabsorption by design)
- Fecal fat test: positive → malabsorption confirmed
- Imaging: CT/MR enterography for mucosal disease, lymphoma, strictures; abdominal X-ray for pancreatic calcification
- Endoscopy + biopsy: upper endoscopy with duodenal biopsies for celiac disease; colonoscopy to terminal ileum for IBD
- Serology: anti-TG2 IgA (celiac), total IgA level
- Breath tests: H2 and methane breath tests for lactose/fructose malabsorption or bacterial overgrowth
- Small intestinal aspirate culture: gold standard for bacterial overgrowth (>10³ CFU/mL)
Key Drug-Related Malabsorption
| Drug | Mechanism |
|---|---|
| Orlistat | Lipase inhibitor → fat malabsorption (intended pharmacologic effect for obesity) |
| Metformin | Reduces vitamin B12 absorption (competes with IF-B12 complex at ileal receptors) |
| Cholestyramine | Bile acid sequestrant → can impair fat-soluble vitamin absorption |
| Proton pump inhibitors | Reduce gastric acid → impair non-heme iron absorption (requires acid for Fe³+ reduction) |
| Antibiotics | Can alter intestinal flora → temporary disruption of absorption |
Oral Rehydration Therapy (ORT) - Clinical Application of Physiology
ORT exploits SGLT1: glucose-Na+ cotransport is intact even in secretory diarrhea (e.g., cholera). Oral rehydration solution (glucose + Na+ + K+ + HCO₃⁻) uses luminal glucose to drive Na+ absorption → water follows osmotically. This is why ORT works even when the gut is secreting massively - the SGLT1 pathway is independent of the CFTR/cAMP secretory pathway.
Parenteral and Enteral Nutrition
- When intestinal absorption is severely compromised (short bowel syndrome, severe Crohn's, radiation enteritis), enteral or parenteral nutrition is required
- Short bowel syndrome: managed with intestinal rehabilitation, teduglutide (GLP-2 analogue that promotes intestinal adaptation), and parenteral nutrition for irreversible cases
Sources:
- Costanzo Physiology 7th Edition - Intestinal Absorption, Electrolyte Transport
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Intestinal Absorption, Bacterial Overgrowth, Water-Soluble Vitamins
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Celiac Disease (Pathogenesis, Morphology)
- Goldman-Cecil Medicine - Malabsorptive Syndromes, Bacterial Overgrowth
- Harrison's Principles of Internal Medicine 22E (2025) - Crohn's Disease
This is a shared conversation. Sign in to Orris to start your own chat.