Erythema infectiosum
Reading File
Finding Sources
Finding Sources
Searching PubMed
erythema infectiosum parvovirus B19
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative textbooks and clinical images. Here is a complete overview:
Erythema Infectiosum (Fifth Disease)
Overview
Erythema infectiosum is an acute exanthematous illness caused by human parvovirus B19 (B19V) — a small (~22 nm), nonenveloped, icosahedral, single-stranded DNA virus belonging to the genus Erythroparvovirus (family Parvoviridae). It is the fifth of the classical numbered childhood exanthems, hence "fifth disease."
Epidemiology
- Worldwide distribution; outbreaks peak in late winter and spring, often in school settings.
- Highest attack rates in children aged 5–15, though all ages are susceptible.
- Seroprevalence rises with age: 15–60% in children 5–19 years → >90% in the elderly.
- Incubation period: 4–14 days; viremia occurs 6–14 days after inoculation; rash appears ~day 17–18.
- Transmission: primarily respiratory droplet during the viremic phase. By the time the rash appears, the child is no longer infectious — can return to school.
- Secondary household attack rate ~50% among susceptible contacts.
- Also transmissible via blood products and vertically (mother → fetus).
- Prior infection confers lifelong immunity.
Pathogenesis
B19V has a narrow tropism for erythroid progenitor cells in the bone marrow, mediated by:
- Blood group P antigen (globoside) as receptor — individuals lacking P antigen are naturally resistant.
- Infection causes lysis of erythroid progenitors, halting red cell production transiently.
In immunocompetent individuals, the viremia resolves as the immune response mounts (~2–3 weeks). The rash and arthralgia of erythema infectiosum are immune-mediated (immune complex deposition), not direct viral cytopathic effects. This is why children are no longer contagious when symptomatic.
Clinical Manifestations
In Children — Classic Three-Stage Exanthem
Stage 1 — "Slapped Cheeks"
Abrupt onset of confluent, fiery-red erythema over the malar eminences with relative circumoral pallor and sparing of the eyelids and chin. The face appears as if slapped.


The facial rash fades over 4–5 days.
Stage 2 — Lacy/Reticulated Rash on Trunk and Extremities
~1–2 days after the facial rash, a maculopapular eruption appears on the trunk, neck, deltoids, and extensor surfaces of the extremities. Central clearing produces a characteristic lacy or reticulated pattern.

- Palms and soles rarely affected.
- Usually non-pruritic (though pruritus can be prominent in some outbreaks).
- Lasts ~1 week; can be morbilliform, circinate, or annular.
Stage 3 — Recurrent/Waxing-Waning Phase
The rash may recur over 3+ weeks, triggered by sunlight, hot baths, exercise, temperature change, or emotional stress.
Associated symptoms: fever, malaise, headache, sore throat, cough, coryza, nausea, vomiting, diarrhea, myalgia.
An enanthem (erythema of tongue, pharynx, red macules on buccal mucosa and palate) can also occur.
In Adults
- Facial slapped-cheek rash is often absent.
- Primary manifestation: acute symmetric polyarthropathy — sudden onset, affecting small joints of the hands, knees, wrists, ankles. More common in women (~50% of adult infections).
- Arthropathy is usually self-limited but can recur/persist for months and may mimic rheumatoid arthritis or Lyme disease.
- Men often present with only a flu-like illness.
- Constitutional symptoms (fever, malaise, depression) tend to be more severe than in children.
- Pruritus with acute-onset arthritis → consider B19V.
Serious/Special Manifestations
| Condition | Population at risk | Mechanism |
|---|---|---|
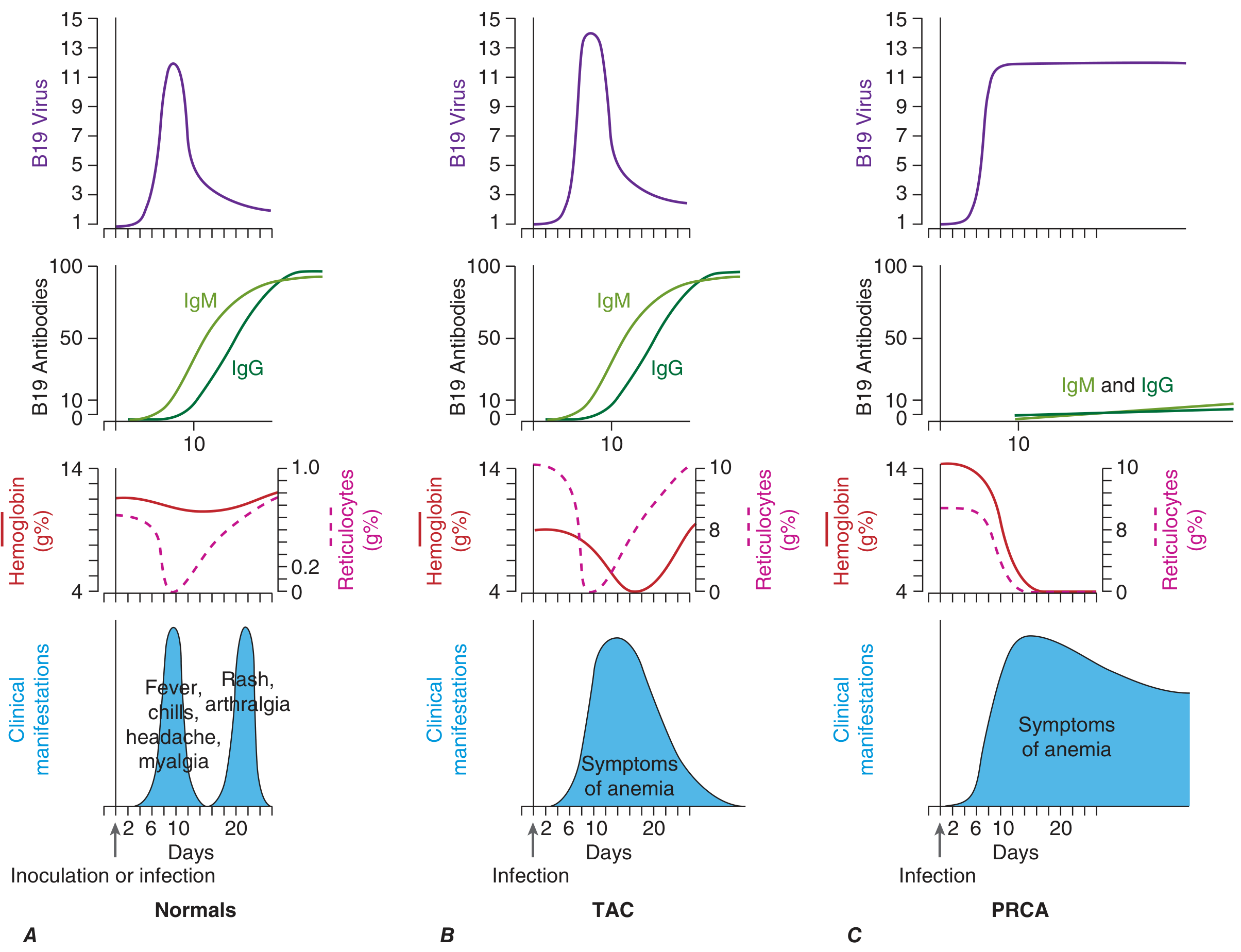
| Transient aplastic crisis (TAC) | Hemolytic anemias (sickle cell, spherocytosis, thalassemia), chronic hemolysis | B19V lyses erythroid progenitors → severe anemia + reticulocytopenia; bone marrow shows giant pronormoblasts, absent erythroid precursors |
| Pure red cell aplasia (PRCA) / chronic anemia | Immunocompromised (AIDS, leukemia, transplant, congenital immunodeficiency) | Failure to mount neutralizing antibody → persistent viral replication → chronic anemia |
| Hydrops fetalis / fetal loss | Seronegative pregnant women | Transplacental infection → fetal erythroid failure → severe anemia → high-output heart failure, gross edema; causes ~10–20% of nonimmune hydrops |
| Papular purpuric gloves-and-socks syndrome | Adolescents/adults | Pruritic erythema, edema, petechiae of hands and feet + fever + oral erosions |
- Fetal risk: ~30% transplacental transmission rate; excess fetal loss ~9% if maternal infection before week 20 (very low after week 20).
- B19V does not appear to be teratogenic, but rare CNS, eye, and congenital anemia cases are reported.
- Rarely: hepatitis, vasculitis, myocarditis, glomerulosclerosis, meningoencephalitis, Henoch-Schönlein purpura.
Virology
- Genus: Erythroparvovirus; 3 genotypes (1, 2, 3) — similar pathogenicity; genotype 1 currently predominant.
- 18–26 nm, nonenveloped, single-stranded DNA.
- Smallest single-stranded DNA virus known to infect humans.
- Animal parvoviruses are not transmissible to humans.
Diagnosis
| Setting | Test of choice | Notes |
|---|---|---|
| Immunocompetent, typical presentation | B19V IgM | Detectable days after rash onset; persists up to 6 months; sensitivity 62–70% |
| Confirming past infection | B19V IgG | Present by day 7; persists years |
| Immunocompromised, pregnant women, fetal infection | B19V DNA PCR | Most sensitive; can detect in serum, amniotic fluid, placenta, bone marrow; caveat: DNA fragments persist >1 year post-infection without indicating viable virus |
| Histopathology (skin) | Non-specific | Sparse superficial perivascular lymphocytic infiltrate |
Lab: Mild anemia, leukopenia, neutropenia, thrombocytopenia can occur but rarely symptomatic in healthy individuals. ESR usually normal. RF occasionally positive with B19-associated arthritis.
Differential Diagnosis
- Drug reaction
- Enteroviral exanthem
- Erysipelas (Stage 1 facial rash)
- Hand-foot-mouth disease
- Atypical measles / rubella
- Papular purpuric gloves-and-socks syndrome
- Systemic lupus erythematosus / collagen vascular disease
- Lyme disease (arthropathy in adults)
- Rheumatoid arthritis (arthropathy in adults)
Management
- In healthy children: entirely supportive — the illness is self-limited; NSAIDs/antipyretics for fever/arthralgia.
- Pregnant seronegative women exposed to B19V: test for acute infection (IgM + PCR); monitor with serial fetal ultrasounds throughout pregnancy if positive.
- Transient aplastic crisis: red blood cell transfusion as needed; typically resolves in ~1 week.
- PRCA in immunocompromised: IV immunoglobulin (IVIG) — effective and often curative; may require repeated courses.
- Fetal hydrops: intrauterine red cell transfusions may be required; many resolve spontaneously.
- No antiviral therapy is currently available specifically for B19V.
- Isolation: children with erythema infectiosum are not infectious once rash appears and do not need to be excluded from school. Immunocompromised patients and those with aplastic crisis, however, may have prolonged viremia and pose a transmission risk.
Prognosis
- Healthy individuals: self-limited; full recovery expected.
- Arthropathy resolves in 1–2 weeks in most but can recur or persist for months.
- Aplastic crisis: potentially fatal if untreated; most recover in ~1 week with support.
- Chronic anemia (PRCA): responds to IVIG in most.
- Fetal hydrops: can lead to fetal death without intervention.
Sources: Fitzpatrick's Dermatology, p. 3024–3026 | Harrison's Principles of Internal Medicine 22E, pp. 1565–1568 | Tintinalli's Emergency Medicine, p. 971 | Andrews' Diseases of the Skin | Swanson's Family Medicine Review
Relations between hcg and thyroid hormone
Reading File
Finding Sources
Finding Sources
Searching PubMed
hCG thyroid stimulation pregnancy
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.