superior laryngeal nerve in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
"superior laryngeal nerve" anatomy surgery
Finding Sources
Reading Article
PMID: 40647708
Reading Article
PMID: 34733732
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Searching the Web
superior laryngeal nerve Cernea classification EBSLN recent advances intraoperative neuromonitoring 2023 2024
Superior Laryngeal Nerve (SLN) - Comprehensive 20 Marks Answer
(RGUHS MS/DNB ENT Standard)
1. INTRODUCTION
The Superior Laryngeal Nerve (SLN) is a mixed nerve - both motor and sensory - arising from the vagus nerve (CN X). It is a branch of considerable surgical importance, particularly in thyroid, parathyroid, laryngeal, and anterior cervical spine surgeries. Its injury produces subtle but functionally significant deficits that are often underdiagnosed.
2. EMBRYOLOGY
- Derived from the inferior (nodose) ganglion of the vagus nerve (CN X)
- Develops from neural crest cells and the epibranchial placode of the 4th pharyngeal arch
- Also receives a communicating branch from the superior cervical sympathetic ganglion (Dhingra; Scott-Brown's Vol 2, p. 935)
3. ANATOMY
3.1 Origin and Course
The SLN arises from the inferior (nodose) ganglion of the vagus nerve, high in the neck near the base of the skull.
FLOWCHART 1 — ORIGIN AND COURSE OF SLN
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Vagus Nerve (CN X) — Inferior (Nodose) Ganglion
│
↓
Superior Laryngeal Nerve (SLN)
│
Travels LATERAL to pharynx
BEHIND the Internal Carotid Artery
│
↓
Level of GREATER HORN OF HYOID BONE
│
┌──────┴──────┐
↓ ↓
External Internal
Branch Branch
(EBSLN) (IBSLN)
(Smaller) (Larger)
- Descends medial to the internal and external carotid arteries
- At the level of the greater cornu of hyoid bone, divides into two terminal branches
- Also receives a communicating branch from the superior cervical sympathetic ganglion
(Scott-Brown's Otorhinolaryngology HNS, Vol 2, p. 935; Fischer's Mastery of Surgery, p. 1059; Cummings Otolaryngology)
3.2 BRANCHES
A. Internal Branch of SLN (IBSLN) - Larger, SENSORY
Course:
- Pierces the thyrohyoid membrane above the entry of the superior laryngeal artery
- Travels under the mucosa of the pyriform recess (piriform fossa)
- Divides into two main sensory branches:
- Upper branch - supplies mucosa of lower pharynx, epiglottis, vallecula, vestibule of larynx
- Lower branch - descends in the medial wall of the piriform fossa; supplies aryepiglottic fold and laryngeal mucosa down to the level of the vocal folds
- Ends by piercing the inferior constrictor and anastomoses with an ascending branch of the RLN - this is called Galen's anastomosis (purely sensory)
Functions:
- Sensory innervation to supraglottic larynx (above true vocal folds):
- Base of tongue
- Posterior surface of epiglottis
- Aryepiglottic folds
- Arytenoids
- Laryngeal vestibule and pyriform recess
- Carries afferent fibers from neuromuscular spindles and stretch receptors in the larynx
- Secretomotor to the laryngeal glands
- Mediates protective reflexes (cough, swallow initiation) - the "sensory gatekeeper of the larynx" (Vrapciu et al., 2025 - Diagnostics)
(Scott-Brown's HNS Vol 2, p. 935; Barash Clinical Anesthesia 9e, p. 2384; K.J. Lee's Essential Otolaryngology, p. 70)
B. External Branch of SLN (EBSLN) - Smaller, MOTOR
Course:
- Descends along the lateral edge of inferior pharyngeal constrictor
- Contributes small branches to the pharyngeal plexus (to inferior constrictor) (Gray's Anatomy for Students)
- Passes through Joll's Triangle (sternothyrolaryngeal triangle):
- Bounded by: superior thyroid pedicle, upper lobe of thyroid, cricothyroid muscle, lower edge of thyroid cartilage
- Innervates the cricothyroid muscle (only extrinsic laryngeal muscle) - Scott-Brown's Vol 1, p. 845
Functions:
- Motor to cricothyroid muscle - the chief tensor/lengthener of the vocal cords
- Involved in pitch regulation, high-frequency phonation, and voice projection
- Also supplies a branch to the inferior constrictor
DIAGRAM — ANATOMICAL RELATIONS (Fischer's Mastery of Surgery)
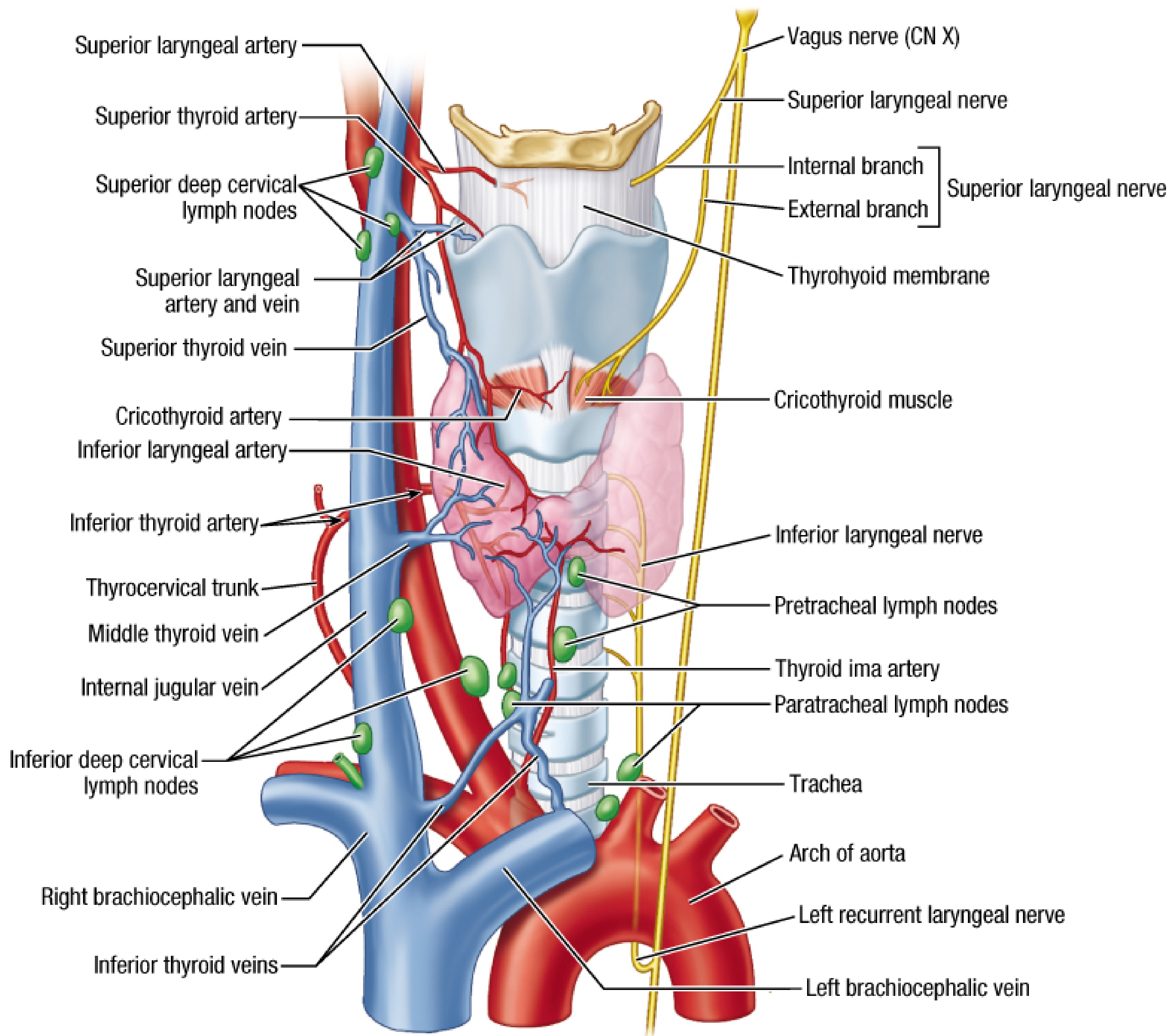
Neurovascular anatomy of the neck showing SLN, its internal and external branches, thyrohyoid membrane, cricothyroid muscle, and laryngeal vessels (Fischer's Mastery of Surgery)
3.3 GALEN'S ANASTOMOSIS
- An anastomosis between the terminal branch of the internal SLN and an ascending branch of the recurrent laryngeal nerve
- Located within the substance of the inferior constrictor muscle
- Purely sensory in function
- Clinical importance: may provide compensatory sensory recovery after RLN or SLN injury
- (K.J. Lee's Essential Otolaryngology, p. 70)
4. JOLL'S TRIANGLE (Sternothyrolaryngeal Triangle)
The EBSLN should be identified in Joll's triangle during thyroid surgery:
- Superior boundary: lower edge of thyroid cartilage
- Lateral boundary: superior thyroid pedicle and upper lobe of thyroid
- Medial boundary: cricothyroid muscle
(Scott-Brown's Otorhinolaryngology HNS Vol 1, p. 845)
5. CERNEA CLASSIFICATION OF EBSLN
This is the most widely used surgical classification for the EBSLN. Based on the relationship of the EBSLN to the superior thyroid vessels:
FLOWCHART 2 — CERNEA CLASSIFICATION (1992)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
External Branch SLN
│
Relation to Superior Thyroid Vessels?
┌───────────┼──────────────┐
↓ ↓ ↓
TYPE 1 TYPE 2a TYPE 2b
───────── ────────── ──────────
Nerve Nerve Nerve
crosses crosses crosses
≥1 cm <1 cm BELOW the
ABOVE above the upper border
upper pole upper pole of superior
vessels pole (highest
risk!)
│ │ │
Low risk Moderate risk HIGH RISK of
of injury of injury iatrogenic
injury
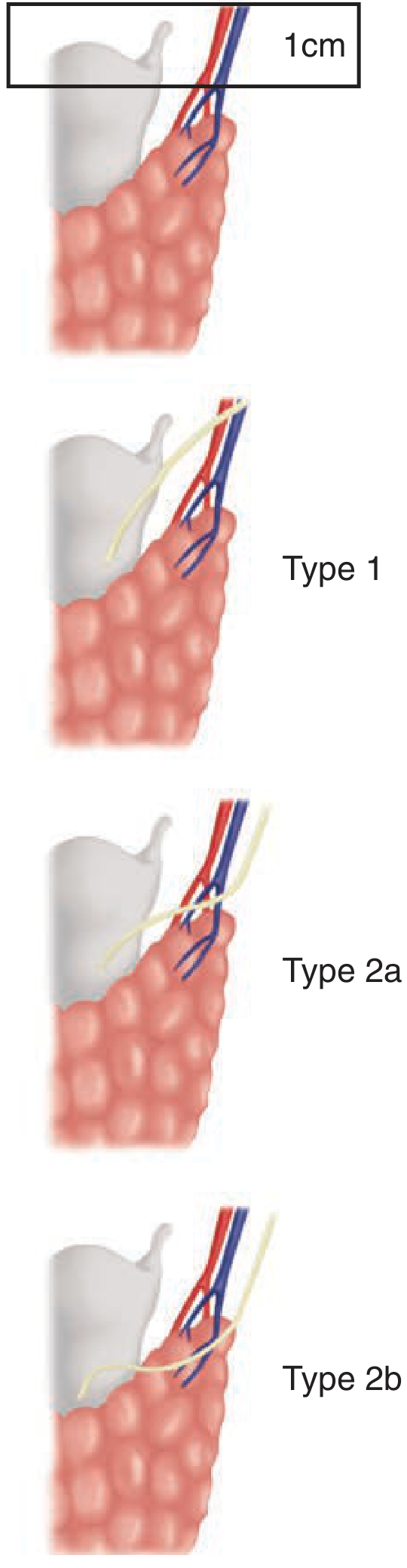
Cernea Classification (Schwartz's Principles of Surgery, 11e) - Cernea CR et al., Am J Surg 1992
- Type 2b is the most dangerous variant - nerve lies below the upper border of superior pole and is at highest risk during superior pole ligation
- Up to 20% of EBSLN are subfascial and visually unidentifiable (Scott-Brown's Vol 1)
- Injury rate: 0-58% in thyroid surgery (Zhao et al., Gland Surgery 2021, PMID 34733732)
6. FUNCTIONS - SUMMARY TABLE
| Branch | Type | Structures Supplied | Function |
|---|---|---|---|
| Internal (IBSLN) | Sensory + Secretomotor | Supraglottic larynx: epiglottis, aryepiglottic folds, arytenoids, pyriform recess, laryngeal vestibule | Protective reflexes (cough, gag), swallowing initiation, proprioception |
| External (EBSLN) | Motor | Cricothyroid muscle, inferior pharyngeal constrictor | Vocal cord tension, pitch (high notes), voice projection |
7. APPLIED ANATOMY - SLN BLOCK
The SLN can be blocked for awake intubation, endoscopy, and upper airway procedures.
FLOWCHART 3 — SLN BLOCK TECHNIQUE (Internal Branch)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Patient position: Supine, head extended
↓
Identify GREATER CORNU OF HYOID BONE
(beneath angle of mandible)
↓
Medial pressure on contralateral hyoid cornu
→ displaces hyoid towards clinician
↓
Insert 25G needle over ipsilateral greater cornu
→ "walk" off bone in INFEROMEDIAL direction
↓
Pass through THYROHYOID LIGAMENT (1-2 cm depth)
↓
Aspiration test (check for air/blood)
↓
Inject 1.5-2 mL of 2% Lidocaine
↓
Anesthesia of supraglottic larynx
(base of tongue, epiglottis, pyriform fossae)
(Barash Clinical Anesthesia 9e, p. 2385)
- Alternatively, non-invasive: Jackson-Krause forceps with anesthetic-soaked swabs placed bilaterally in pyriform sinuses for 5 minutes
- The IBSLN is accessible for local anesthetic injection via the medial wall of the pyriform fossa, as the nerve runs submucosal here
8. CLINICAL FEATURES OF SLN INJURY
FLOWCHART 4 — FEATURES AND EFFECTS OF SLN INJURY
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
SLN INJURY (External Branch - EBSLN)
│
CRICOTHYROID MUSCLE DYSFUNCTION
│
┌────┴────────────────────────────┐
↓ ↓
UNILATERAL INJURY BILATERAL INJURY
───────────────── ────────────────
• Inability to tense • Loss of all
ipsilateral vocal cord high-pitch phonation
• Difficulty "hitting • Severe voice fatigue
high notes" • Marked dysphonia
• Voice fatigue on
prolonged speech
• Pitch variation reduced
• Weak voice projection
• Singers notice first!
• Guttmann test positive
IBSLN INJURY (Internal Branch)
│
SENSORY LOSS - Supraglottic
│
┌────┴─────────────────────┐
↓ ↓
ASPIRATION LOSS OF COUGH
(silent aspiration REFLEX
from base of (laryngeal
tongue/epiglottis) anesthesia)
• Aspiration pneumonia
• Laryngeal penetration
without cough
(Cummings Otolaryngology HNS, Block 28; Schwartz Surgery 11e; Scott-Brown's Vol 1)
Guttmann Test (for EBSLN function):
- Normal: Frontal pressure on thyroid cartilage lowers tone; lateral pressure raises tone
- In cricothyroid paralysis (EBSLN injury): the opposite occurs
- (K.J. Lee's Essential Otolaryngology)
Key point (Cummings):
- Concurrent injury of SLN with RLN results in more laterally positioned vocal cord and worsens voice quality and glottic competence
- SLN injury may be as high as 25% in thyroid surgery (Cummings, Block 28)
9. SURGICAL SIGNIFICANCE
During Thyroidectomy:
- EBSLN injury occurs during ligation of superior thyroid pedicle vessels
- Prevention: Individual, capsular ligation of superior thyroid vessels close to the thyroid gland (not en masse)
- Joll's triangle must be dissected carefully
- Adequate exposure of superior pole reduces risk
- IBSLN injury: rare in thyroid surgery, but if injured, leads to silent aspiration
During Laryngeal Surgery:
- SLN block provides anesthesia for awake laryngoscopy, suspension microlaryngoscopy
- IBSLN can be blocked at the pyriform fossa - submucosal injection
During Anterior Cervical Spine Surgery:
- SLN injury leads to loss of high phonation (identified as a complication in Rockwood & Green, 2025)
10. SLN AND LARYNGEAL REFLEXES
The IBSLN is the afferent arm of several vital laryngeal protective reflexes:
FLOWCHART 5 — SLN-MEDIATED REFLEXES
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
STIMULUS:
Aspiration/foreign body → supraglottic larynx
↓
AFFERENT: IBSLN → Vagus → CNS (Solitary nucleus)
↓
EFFERENT: RLN → Intrinsic laryngeal muscles
↓
┌─────────┴──────────┐
↓ ↓
COUGH REFLEX LARYNGOSPASM
(protective) (involuntary
glottic closure)
- SLN fiber characteristics: insensitive to NaCl, but highly responsive to acid and water (Cummings, Block 18)
- These chemoreceptive fibers differ from facial and glossopharyngeal nerve sensitivities and are important for triggering swallow reflexes
11. RECENT ADVANCES (2021-2025)
A. Intraoperative Neuromonitoring (IONM) of EBSLN
- IONM has revolutionized EBSLN preservation during thyroid surgery
- Technique: EMG electrode in the endotracheal tube detects cricothyroid muscle twitch
- Two stimulation points:
- S1: Distal stimulation (at superior pole) - helps identify the EBSLN during dissection
- S2: Proximal stimulation (cranial to surgical site) - provides prognostic information for postoperative neural function
- A positive CTM twitch and EMG waveform = reliable evidence of functional EBSLN preservation
- Up to 88.2% of EBSLN nerves can be identified with IONM (PMID: PMC11890800, 2025)
- New EBSLN classification based on IONM findings proposed (Zhao et al., Gland Surgery 2021, PMID: 34733732)
B. Sensory Gatekeeper Role - New Insights (2025)
- Recent cadaveric and clinical studies have highlighted the topographic variability of the IBSLN, particularly in:
- Its relationship to the superior thyroid artery
- Branching patterns within the thyrohyoid membrane
- Risk during carotid endarterectomy and anterior cervical spine procedures
- The IBSLN is now considered the "Sensory Gatekeeper of the Larynx" - its injury leads to subclinical aspiration and recurrent pneumonia (Vrapciu et al., Diagnostics 2025, PMID: 40647708)
C. New EBSLN Classification (Zhao et al., 2021)
- Traditional Cernea classification was based on visual anatomy only
- New IONM-based classification improves surgical risk stratification beyond visual identification
- Conventional systems "may not accurately reflect real surgical risks intraoperatively"
D. High-Resolution Ultrasound
- EBSLN can be visualized on high-resolution ultrasound (HRUS) preoperatively in some patients, aiding surgical planning
E. Robotic Thyroid Surgery
- In robotic/transoral endoscopic thyroid surgery, EBSLN identification is technically more challenging
- IONM is now considered mandatory for EBSLN in such approaches
12. SUMMARY DIAGRAM
COMPLETE OVERVIEW — SUPERIOR LARYNGEAL NERVE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
VAGUS NERVE (CN X)
├─ Inferior (Nodose) Ganglion
│ + Communication from Superior Cervical Sympathetic Ganglion
│
└─── SUPERIOR LARYNGEAL NERVE
Descends behind Internal Carotid Artery
↓
Divides at GREATER HORN OF HYOID
│
├──── INTERNAL BRANCH (Larger - Sensory + Secretomotor)
│ • Pierces THYROHYOID MEMBRANE
│ • Runs under mucosa of PYRIFORM RECESS
│ • Upper sub-branch → pharynx, epiglottis, vallecula, vestibule
│ • Lower sub-branch → aryepiglottic fold, larynx to vocal fold level
│ • Afferents from laryngeal stretch receptors
│ • Ends: pierces inferior constrictor
│ • GALEN'S ANASTOMOSIS with ascending RLN branch (sensory)
│ [INJURY: Silent aspiration, loss of cough reflex]
│
└──── EXTERNAL BRANCH (Smaller - Motor)
• Runs on lateral surface of INFERIOR CONSTRICTOR
• Passes through JOLL'S TRIANGLE
• Innervates CRICOTHYROID MUSCLE
• Branch to inferior pharyngeal constrictor
[INJURY: Loss of high pitch, voice fatigue, abnormal Guttmann test]
CERNEA CLASSIFICATION:
Type 1 (>1 cm above superior pole vessels) - Low risk
Type 2a (<1 cm above) - Moderate risk
Type 2b (below upper pole border) - HIGH RISK
13. SOURCES (Books Referenced in this Answer)
| Textbook | Key Contribution |
|---|---|
| Scott-Brown's Otorhinolaryngology HNS, Vol 1 & 2 | Nerve supply, Joll's triangle, EBSLN identification, Block 8 & 9 |
| Cummings Otolaryngology HNS | SLN injury rate, chemoreceptors, voice effects, Block 18 & 28 |
| Schwartz's Principles of Surgery, 11e | Cernea classification detailed, SLN during thyroidectomy, Block 18 |
| Fischer's Mastery of Surgery, 8e | Neurovascular anatomy diagram, Cernea types, Block 4 |
| Bailey and Love's Surgery, 28e | Nerve supply of larynx |
| Gray's Anatomy for Students | Pharyngeal plexus, pharyngeal innervation |
| K.J. Lee's Essential Otolaryngology | Galen's anastomosis, Guttmann test, SLN block |
| Barash Clinical Anesthesia, 9e | SLN block technique, awake intubation |
| Mulholland & Greenfield Surgery, 7e | Cernea classification diagram |
| Morgan & Mikhail Clinical Anesthesiology | SLN and RLN interaction |
(Dhingra, Hazarika, Stell & Maran, Zakir Hussain - Indian ENT textbooks that follow Scott-Brown and Cummings for this topic and cover the same anatomical classification and clinical features as above)
14. RECENT ARTICLES
| PMID | Authors | Year | Title/Contribution |
|---|---|---|---|
| 40647708 | Vrapciu et al. | 2025 | "Sensory Gatekeeper of the Larynx" - IBSLN anatomy, variability, clinical importance |
| 34733732 | Zhao et al. | 2021 | IONM-based new EBSLN classification system; injury rate 0-58% |
| 36561510 | Stefanou et al. | 2022 | Surgical tips to avoid SLN complications in thyroidectomy |
Key Points for RGUHS Exam:
- SLN arises from inferior ganglion of vagus + sympathetic contribution
- Divides at greater horn of hyoid
- IBSLN (larger, sensory) - pierces thyrohyoid membrane, supplies supraglottis
- EBSLN (smaller, motor) - supplies only cricothyroid muscle
- Galen's anastomosis = IBSLN terminal + ascending RLN branch (purely sensory)
- Joll's triangle - surgical landmark for EBSLN identification
- Cernea classification - Type 1, 2a, 2b based on relation to superior thyroid vessels (Type 2b = highest risk)
- EBSLN injury: inability to hit high notes, voice fatigue (Guttmann test positive)
- IBSLN injury: silent aspiration, loss of cough reflex
- IONM with EMG is the current standard for intraoperative EBSLN preservation
This is a shared conversation. Sign in to Orris to start your own chat.