hey i am a first year mbbs student in kusms nepal and i have a pbl session tomorrow i need to learn about some topics so please give answers to my questions carefully and make sure you give every answer with respect to any medical books
also mention the source of each answer and make sure each answers are from any medical books
Tell me about unhappy traid of knee and its significance
Unhappy Triad of the Knee (O'Donoghue's Triad)
Definition
- Anterior Cruciate Ligament (ACL)
- Medial Collateral Ligament (MCL) (tibial collateral ligament)
- Medial Meniscus
"O'Donoghue's 'unhappy' triad describes tears of the ACL, medial collateral ligament (MCL) and medial meniscus secondary to valgus stress."
- Grainger & Allison's Diagnostic Radiology
Mechanism of Injury
- Abduction (valgus force) at the knee
- Flexion of the knee
- Internal rotation of the femur on the fixed tibia
"When abduction, flexion, and internal rotation of the femur on the tibia occur, the medial supporting structures (the MCL and the medial capsular ligament) are the initial structures injured. If the force is of sufficient magnitude, the ACL also can be torn. The medial meniscus may be trapped between the condyles of the femur and the tibia, and it may be torn at its periphery as the medial structures tear, thus producing 'the unhappy triad' of O'Donoghue."
- Campbell's Operative Orthopaedics, 15th Ed. (2026)
"This is most often seen in contact sports with a lateral blow to a planted leg, causing a significant valgus..."
- Schwartz's Principles of Surgery, 11th Ed.
An Important Modern Update
"The traditional 'unhappy triad' of ACL, MCL, and medial meniscal injury is actually less common than the combination of ACL, MCL, and lateral meniscal injury."
- Rosen's Emergency Medicine, 9th Ed.
Clinical Features
| Feature | Detail |
|---|---|
| Audible "pop" | Heard at time of injury (from ACL tear) |
| Rapid hemarthrosis | Swelling within 1-3 hours |
| Medial joint line pain | From MCL + meniscus injury |
| Instability / "giving way" | From ACL insufficiency |
| Unable to bear weight | Acute phase |
- Lachman test - most sensitive and specific test for ACL tear
- Anterior drawer test - also used for ACL
- Valgus stress test - for MCL integrity
- McMurray's test / Thessaly test - for meniscal tear
Investigations
- X-ray (AP, lateral, sunrise, notch views) - to rule out fractures; look for Segond fracture (lateral tibial plateau avulsion - associated with ACL tears)
- MRI - gold standard to confirm ligament and meniscal injuries
"MRI is the preferred imaging modality to identify ligamentous injuries."
- Rosen's Emergency Medicine
Clinical Significance
- Common sports injury - especially in football, skiing, rugby
- Requires surgical management in active individuals - ACL reconstruction is needed to restore knee stability; the MCL often heals conservatively, but meniscal tears may need repair/meniscectomy
- Long-term risk of osteoarthritis - even after treatment, internal joint damage leads to early degenerative changes
- Instability cascade - an untreated ACL tear leads to repeated episodes of giving way, causing further cartilage and meniscal damage over time
"In those with high activity levels, surgical reconstruction of the ligament is required... in the long term the internal damage to the knee leads to the development of early osteoarthritis."
- Gray's Anatomy for Students
Summary Table
| Structure Injured | Role in Knee | Result of Injury |
|---|---|---|
| ACL | Prevents anterior tibial translation & rotation | Anterior instability, giving way |
| MCL (Tibial collateral lig.) | Resists valgus force | Medial instability |
| Medial/Lateral Meniscus | Shock absorption, joint congruence | Pain, locking, long-term OA |
- Campbell's Operative Orthopaedics, 15th Ed. (2026) - Mechanism of Injury
- Gray's Anatomy for Students - Collateral Ligament Injuries
- Schwartz's Principles of Surgery, 11th Ed. - Collateral Ligaments
- Rosen's Emergency Medicine - Cruciate and Collateral Ligament Injuries
- Grainger & Allison's Diagnostic Radiology - Anterior Cruciate Ligament
- General Anatomy and Musculoskeletal System (Thieme Atlas) - Mechanisms of Injury
tell its significance and why is more common in sports
Significance of the Unhappy Triad & Why It Is Common in Sports
1. Clinical Significance
A. It Involves Three Critical Stabilizing Structures Simultaneously
| Structure | Function Lost |
|---|---|
| ACL | Resists anterior tibial translation and rotational stability |
| MCL | Resists valgus (inward) forces on the knee |
| Medial/Lateral Meniscus | Shock absorption, joint congruence, load distribution |
"The ACL's primary function is to restrict anterior translation of the tibia on the femur."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
B. It Causes Immediate Functional Disability
- Patients hear/feel a "pop" at the time of injury
- Haemarthrosis (bleeding into joint) develops within 1-12 hours
- Inability to bear weight on the injured limb
- Feeling of "giving way" - the knee buckles with any cutting or pivoting movement
- Medial joint line pain from meniscal and MCL damage
"Patients with an acute ACL injury will often report hearing or feeling a pop in their knee followed by a notable effusion and/or haemarthrosis. Once the effusion resolves, they may report a paucity of knee pain, often leading the patient to believe that the injury has healed itself. However, patients usually present to a physician after attempting subsequent cutting and pivoting activities, which can lead to recurrent instability."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
C. High Risk of Long-Term Osteoarthritis
"Chondral and meniscal injuries that occur at the time of initial ACL rupture have been demonstrated to be the main predictors of arthritic change."
- Miller's Review of Orthopaedics, 9th Ed.
"In the long term the internal damage to the knee leads to the development of early osteoarthritis."
- Gray's Anatomy for Students
- Chronic ACL deficiency leads to repeated episodes of subluxation, which cause progressive cartilage damage and complex meniscal tears
- Loss of the meniscus removes the primary shock absorber of the knee, dramatically accelerating joint degeneration
D. Surgical Complexity
- ACL reconstruction (using patellar tendon or hamstring graft)
- Possible meniscal repair or partial meniscectomy
- MCL usually managed non-operatively (heals on its own)
"MCL injuries typically treated nonoperatively."
- Miller's Review of Orthopaedics, 9th Ed.
E. Risk of Failure to Return to Sport
"The most common reasons for failure to return to play/sport after ACL reconstruction are pain and fear of reinjury."
- Miller's Review of Orthopaedics, 9th Ed.
2. Why Is It More Common in Sports?
A. The Injury Requires a Very Specific Force Combination
"Acute knee injuries are extremely common in most sports that require jumping, twisting, and contact. Sports with physical impact or tackling, such as rugby or American football, can result in contact knee injuries that often lead to varus or valgus stresses to the knee, resulting in collateral ligament injuries in addition to concomitant cruciate ligament, meniscus or articular cartilage injuries."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
B. Two Distinct Sporting Mechanisms
- A direct lateral blow to the knee while the foot is planted
- Forces the knee into valgus → tears MCL first, then ACL, then traps the meniscus
- Sudden deceleration, change of direction, or landing from a jump
- The knee collapses into valgus with the tibia externally rotating
"The most common mechanism of these injuries is a deceleration when the knee falls into valgus and the tibia externally rotates, leading to a subluxation of the knee."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
"Mechanism of injury is typically a valgus load with internal tibial rotation and anterior tibial translation while the knee is in almost full extension."
- Miller's Review of Orthopaedics, 9th Ed.
C. High-Risk Sports Identified
"Skiing, soccer, basketball, and football are the highest-risk sports."
- Miller's Review of Orthopaedics, 9th Ed.
"ACL rupture is a typical sequela of sports injuries and occurs about 10 times as often as a rupture of the posterior cruciate ligament. 20% of all knee injuries involve an ACL rupture."
- General Anatomy and Musculoskeletal System (Thieme Atlas of Anatomy)
D. Female Athletes Are at Higher Risk
"Female athletes have a two to eight times higher risk of ACL tear than male athletes. Thought to occur because women have different landing biomechanics. Women have a greater total valgus knee loading in landing and land more erectly. Women have increased quadriceps-to-hamstring strength, causing greater anterior shear. Smaller notches, smaller ligaments, greater generalized ligament laxity... are additional proposed factors."
- Miller's Review of Orthopaedics, 9th Ed.
E. Age Distribution
"70% of ACL ruptures occur between the ages of 15 and 45, whereby women are affected significantly more often than men."
- Thieme Atlas of Anatomy
Summary
| Why Sports? | Reason |
|---|---|
| Planted foot + twisting/tackling | Creates the exact valgus + rotation force needed |
| High-speed deceleration | Common in soccer, basketball, skiing |
| Repeated jumping and landing | Stresses ACL and menisci repeatedly |
| Direct contact/collision | Lateral blow to knee - classic mechanism |
| Young, active age group (15-45) | Peak sports participation years |
- Bailey and Love's Short Practice of Surgery, 28th Ed. - ACL Rupture with Meniscus Tear
- Miller's Review of Orthopaedics, 9th Ed. - ACL Injury
- General Anatomy and Musculoskeletal System, Thieme Atlas of Anatomy - ACL Rupture, Mechanisms and Epidemiology
- Gray's Anatomy for Students - Collateral Ligament Injuries
- Campbell's Operative Orthopaedics, 15th Ed. - Mechanism of Injury
what do you mean by valgus here?
What is Valgus? (and Varus)
The Simple Rule
| Term | Direction of distal bone | Common name at knee |
|---|---|---|
| Valgus | Points away from the midline (outward) | Knock-knee (Genu valgum) |
| Varus | Points toward the midline (inward) | Bow-leg (Genu varum) |
Textbook Definition
"A varus deformity in the knee joint exists if the axis deviation is concave to the vertical body axis, or if the distal bone (the tibia) points to the median line (e.g., genu varum = bow-leggedness). In a valgus deformity of the knee joint, the axis deviation is convex to the vertical body axis, or the tibia points away from the median line (e.g., genu valgum = knock knee)."
- General Anatomy and Musculoskeletal System, Thieme Atlas of Anatomy
"Genu valgum = abnormal abduction of the knee joint. Genu varum = abnormal adduction of the knee joint. In case of genu valgum or knock knee, the degree of deformity can be estimated by the intermalleolar separation present when the inner sides of the knees are kept in apposition."
- S. Das - A Manual on Clinical Surgery, 13th Ed.
Visualizing It at the Knee
Normal: Valgus (knock-knee): Varus (bow-leg):
| / \
| / \
| (straight) / (tibia goes out) \ (tibia goes in)
- In valgus, the knees touch each other but the ankles are apart - "knock-knees"
- In varus, the ankles touch but there is a gap between the knees - "bow-legs"
How Valgus Causes the Unhappy Triad
- Stretches and tears the MCL on the medial (inner) side - because it is being pulled apart
- The force continues and tears the ACL inside the joint
- The medial meniscus gets pinched and torn between the bones
"Injury to the tibial collateral ligament is damaged when excessive force is applied inward to the lateral side of the joint (valgus force)."
- Gray's Anatomy for Students
Quick Summary
| Valgus | Varus | |
|---|---|---|
| Tibia direction | Away from midline | Toward midline |
| Common name | Knock-knee | Bow-leg |
| Latin root | Bent outward | Bent inward |
| Stress on knee | Opens the medial side (tears MCL) | Opens the lateral side (tears LCL) |
| Causes unhappy triad? | Yes | No (causes lateral injuries instead) |
- General Anatomy and Musculoskeletal System, Thieme Atlas of Anatomy - Axis Deviation of Upper and Lower Limbs
- S. Das - A Manual on Clinical Surgery, 13th Ed. - The Knee Joint
- Gray's Anatomy for Students - Collateral Ligament Injuries
replace the word vulgus and then give me the answer
What is a "Knock-Knee Force"? (Understanding Valgus Simply)
The Simple Concept
A force that pushes the knee inward (medially), while the lower leg (tibia) is pushed outward - creating a "knock-knee" position.
- Your foot is planted on the ground (cannot move)
- Someone hits you from the outside of your knee
- Your knee gets forced inward
- But your foot stays fixed
- This creates a bending stress that pulls apart the inner side of the knee
The Two Terms - Simply Put
| Medical Term | Plain English | How the knee looks |
|---|---|---|
| Valgus (knock-knee force) | Lower leg pushed outward, knee buckles inward | Knees touch, ankles apart |
| Varus (bow-leg force) | Lower leg pushed inward, knee pushed outward | Gap between knees, ankles touch |
"In a knock-knee deformity (genu valgum), the tibia points away from the midline of the body. In a bow-leg deformity (genu varum), the tibia points toward the midline."
- Thieme Atlas of Anatomy - General Anatomy and Musculoskeletal System
How This "Knock-Knee Force" Causes the Unhappy Triad
TACKLE
→→→
Thigh |
| ← knee forced inward
Shin \___ foot fixed on ground
- Tears the MCL - the ligament on the inner side gets violently stretched and snaps
- Tears the ACL - as the knee continues to buckle, the ACL inside the joint ruptures
- Traps and tears the meniscus - the medial meniscus gets pinched between the femur and tibia
"Injury to the tibial collateral ligament (MCL) is caused when excessive force is applied to the lateral side of the joint, creating a knock-knee (inward buckling) stress."
- Gray's Anatomy for Students
"When the knee is forced into a knock-knee position (abduction + flexion + internal rotation of the femur on the fixed tibia), the MCL and medial capsular ligament are the first structures injured. If the force is great enough, the ACL also tears. The medial meniscus gets trapped between the condyles and tears at its periphery - producing the unhappy triad of O'Donoghue."
- Campbell's Operative Orthopaedics, 15th Ed. (2026)
Visual Diagram
One-Line Summary
- Thieme Atlas of Anatomy - General Anatomy and Musculoskeletal System - Axis Deviation of Limbs
- Gray's Anatomy for Students - Collateral Ligament Injuries
- Campbell's Operative Orthopaedics, 15th Ed. - Mechanism of Injury
- S. Das - A Manual on Clinical Surgery, 13th Ed. - The Knee Joint
give name and function of all ligaments of knee in short
Ligaments of the Knee Joint - Names and Functions
Diagram (Posterior View)
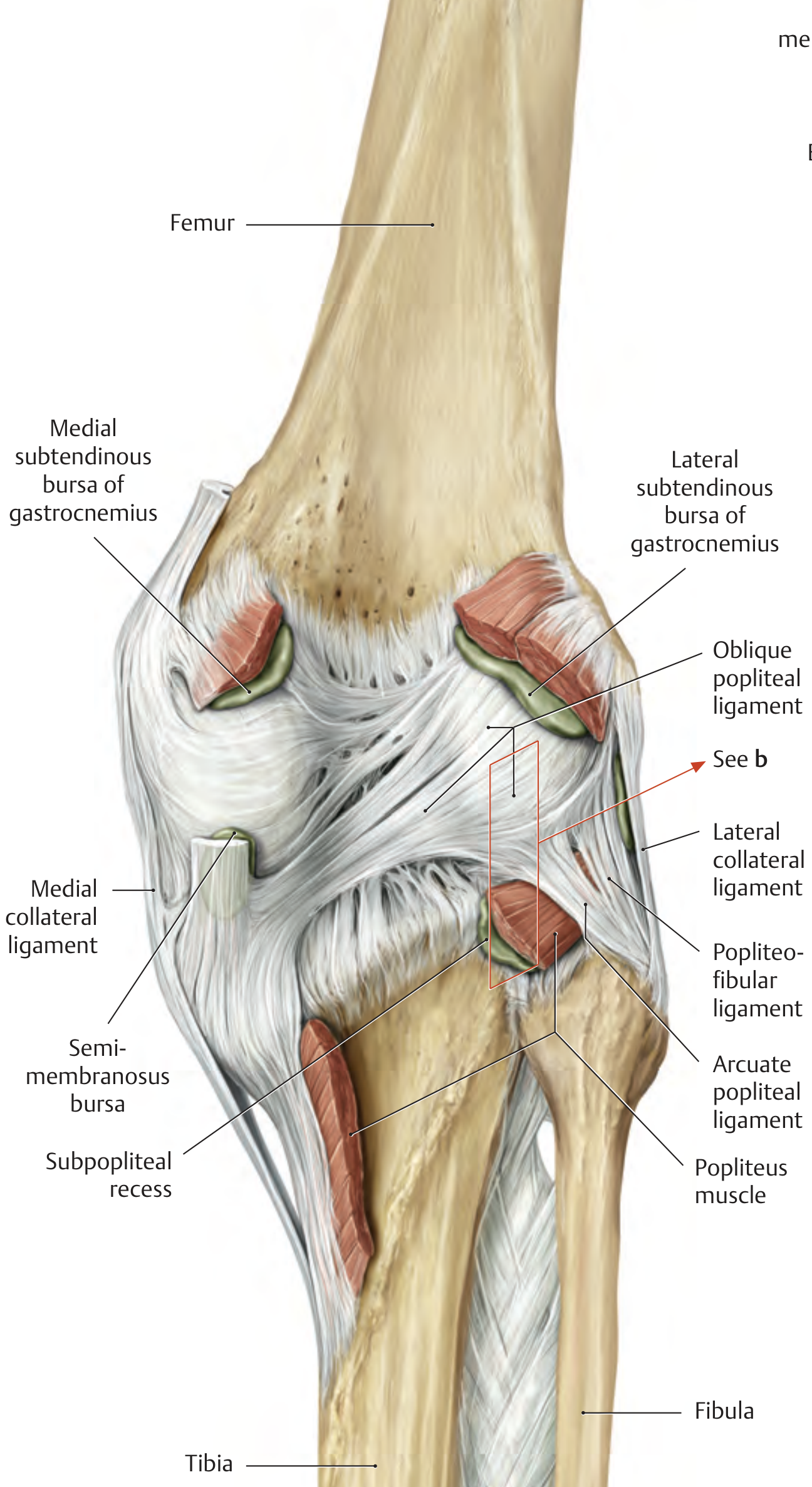
A. Cruciate Ligaments (Inside the Joint)
| Ligament | Function |
|---|---|
| Anterior Cruciate Ligament (ACL) | Resists anterior translation of tibia on femur; also prevents hyperextension and internal rotation |
| Posterior Cruciate Ligament (PCL) | Resists posterior translation of tibia on femur; also prevents hyperflexion |
"ACL: Resists anterior translation, hyperextension. PCL: Resists posterior translation, hyperflexion."
- Miller's Review of Orthopaedics, 9th Ed. (Table 2.27)
- Anteromedial (AM) bundle - tight in flexion, resists anterior translation
- Posterolateral (PL) bundle - tight in extension, resists rotatory loads
B. Collateral Ligaments (Sides of the Joint)
| Ligament | Side | Function |
|---|---|---|
| Medial Collateral Ligament (MCL) - Superficial | Medial (inner) | Resists knock-knee (inward buckling) force; also resists tibial external rotation |
| MCL - Deep | Medial (inner) | Resists knock-knee force; also stabilizes the medial meniscus |
| Lateral Collateral Ligament (LCL) - also called Fibular Collateral Ligament | Lateral (outer) | Resists bow-leg (outward buckling) force; also resists tibial external rotation |
"MCL: Resists valgus force, stabilizes medial meniscus. LCL: Resists varus force."
- Miller's Review of Orthopaedics, 9th Ed. (Table 2.27)
C. Posterior Ligaments (Back of the Joint)
| Ligament | Function |
|---|---|
| Oblique Popliteal Ligament | Strengthens the posterior capsule; resists hyperextension; also resists inward buckling force |
| Arcuate Popliteal Ligament | Provides posterior support to the joint; part of the posterolateral corner |
| Popliteofibular Ligament | Resists tibial external rotation (especially during flexion); resists posterior tibial displacement |
"The popliteofibular ligament, the LCL, and the iliotibial tract are referred to as the 'posterior ligament complex.' This acts as a passive stabilizer especially in external rotation and posterior tibial translation."
- Thieme Atlas of Anatomy
D. Anterior Ligaments (Front of the Joint)
| Ligament | Function |
|---|---|
| Patellar Ligament (continuation of quadriceps tendon) | Connects patella to tibial tuberosity; transmits force of quadriceps to extend the knee |
| Medial Patellofemoral Ligament (MPFL) | Resists lateral displacement of the patella |
| Retinacular Ligaments (medial & lateral) | Form the anterior capsule; help stabilize the patella |
E. Intra-articular Ligaments (Inside, Related to Menisci)
| Ligament | Function |
|---|---|
| Ligament of Humphrey (anterior meniscofemoral) | Stabilizes the lateral meniscus; runs anterior to PCL |
| Ligament of Wrisberg (posterior meniscofemoral) | Stabilizes the lateral meniscus; runs posterior to PCL |
| Transverse (Intermeniscal) Ligament | Connects anterior horns of both menisci; stabilizes both menisci |
"Humphrey: anterior to PCL - stabilizes lateral meniscus. Wrisberg: posterior to PCL - stabilizes lateral meniscus. Transverse meniscal ligament: connects anteromedial to anterolateral meniscus."
- Miller's Review of Orthopaedics, 9th Ed. (Table 2.27)
Quick Summary Table (For Revision)
| Group | Ligament | One-line Function |
|---|---|---|
| Cruciate | ACL | Stops tibia sliding forward |
| Cruciate | PCL | Stops tibia sliding backward |
| Collateral | MCL | Stops knee buckling inward |
| Collateral | LCL | Stops knee buckling outward |
| Posterior | Oblique popliteal | Strengthens back of joint, stops overstraightening |
| Posterior | Arcuate popliteal | Posterior support, posterolateral corner |
| Posterior | Popliteofibular | Stops excessive outward rotation of tibia |
| Anterior | Patellar ligament | Extends knee (quadriceps force transmission) |
| Anterior | MPFL | Stops kneecap slipping outward |
| Intra-articular | Humphrey & Wrisberg | Stabilize lateral meniscus |
| Intra-articular | Transverse meniscal | Stabilize both menisci |
- Miller's Review of Orthopaedics, 9th Ed. - Table 2.27: Ligaments of the Knee; Table 4.1: Stabilizing Functions
- Thieme Atlas of Anatomy - General Anatomy and Musculoskeletal System - Overview of Knee Ligaments
- Campbell's Operative Orthopaedics, 15th Ed. - Knee Ligaments
Mechanism of Muscle cramp . Also about Ors composition and use of glucose in ORS osmomolarity and how it helps in muscle cramps
1. Mechanism of Muscle Cramp
Normal Muscle Contraction (Quick Recap)
- A motor nerve fires an action potential
- This releases acetylcholine at the neuromuscular junction
- Sodium (Na⁺) rushes in → depolarizes the muscle cell
- Calcium (Ca²⁺) is released from the sarcoplasmic reticulum
- Actin-myosin cross-bridges form → muscle contracts
- ATP is used to pump Ca²⁺ back in and restore the resting state → muscle relaxes
How a Cramp Occurs
A. Electrolyte Imbalance (Most Common in Sports/Diarrhea)
| Electrolyte Lost | Effect |
|---|---|
| Sodium (Na⁺) low (hyponatremia) | Resting membrane potential becomes unstable; spontaneous nerve firing |
| Potassium (K⁺) low (hypokalemia) | Cannot repolarize the muscle cell after contraction - stays depolarized |
| Magnesium (Mg²⁺) low | Mg²⁺ normally blocks calcium channels; without it, excess Ca²⁺ floods the cell → sustained contraction |
| Calcium (Ca²⁺) low (hypocalcemia) | Increases nerve excitability → spontaneous motor neuron firing |
B. Dehydration
C. Fatigue / Reduced Blood Flow
- Lactic acid and other metabolic waste products accumulate
- ATP depletion - the Na⁺/K⁺-ATPase pump cannot restore ion gradients
- Without the pump working, Na⁺ accumulates inside the cell → sustained depolarization → cramp
"Transient muscle cramps and tetany are common [with severe dehydration and electrolyte loss]."
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
2. ORS - Composition
| Constituent | Concentration (mmol/L) |
|---|---|
| Sodium (Na⁺) | 75 |
| Potassium (K⁺) | 20 |
| Chloride (Cl⁻) | 65 |
| Citrate (base/bicarbonate) | 10 |
| Glucose | 75 |
| Total Osmolarity | 245 mOsm/kg |
- NaCl: 2.6 g
- Sodium citrate: 2.9 g
- KCl: 1.5 g
- Glucose (anhydrous): 13.5 g
"WHO now recommends 'low-osmolarity' ORS (245 mOsm/kg) for treatment of individuals with dehydrating diarrhea of any cause."
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- ½ teaspoon salt + 6 teaspoons sugar in 1 litre of safe water + potassium source (banana/coconut water)
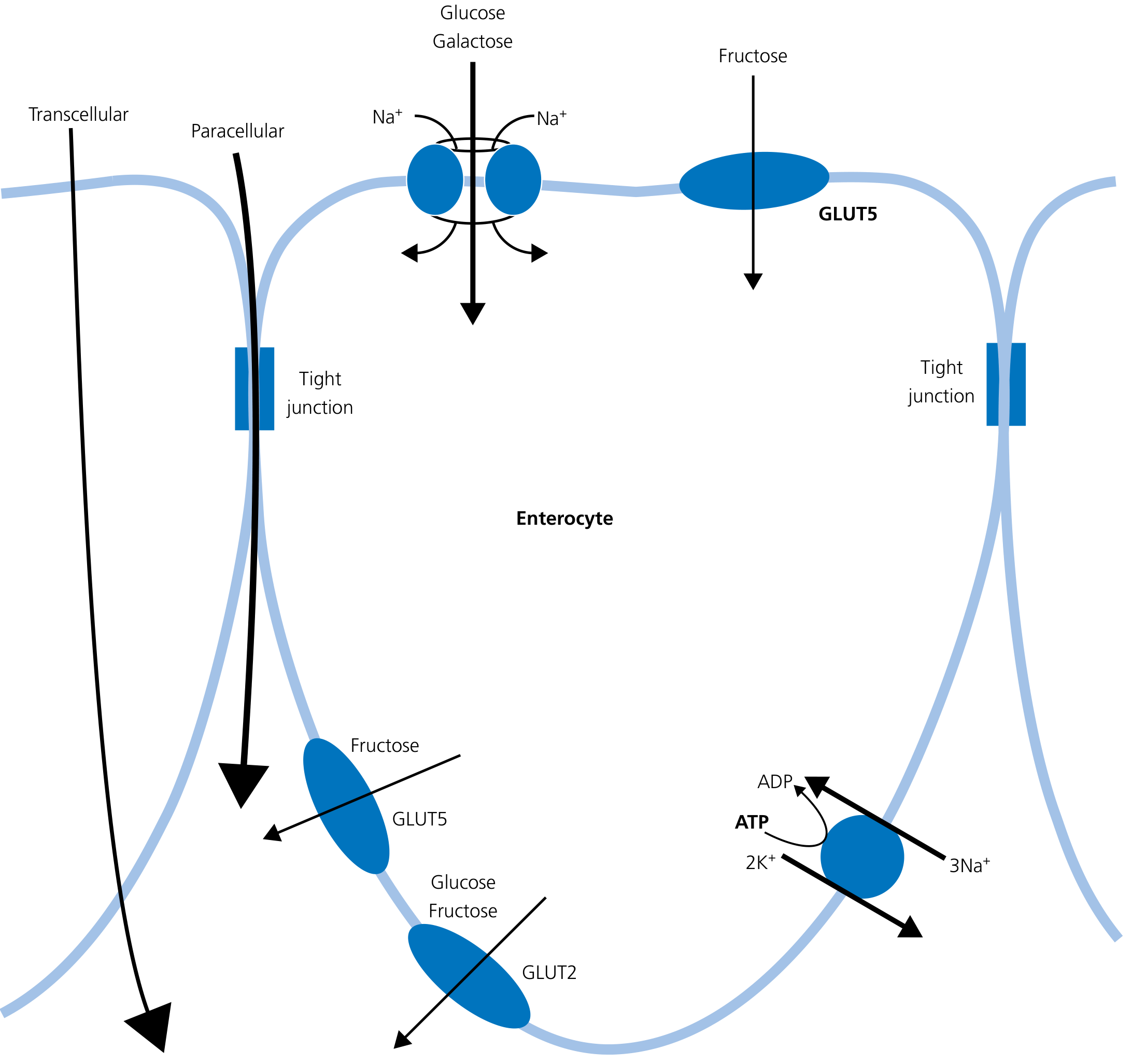
3. Role of Glucose in ORS - The SGLT1 Mechanism
The SGLT1 Cotransporter
"Glucose and galactose are transported across the apical membrane by the Na⁺-dependent cotransporter SGLT1. Each monosaccharide molecule is transported with ~264 molecules of water, resulting in the net absorption of 5-6 litres of water per day - thus the rationale for adding glucose to oral rehydration solutions."
- Yamada's Textbook of Gastroenterology, 7th Ed.
How it works (Step by Step):
Intestinal Lumen
|
Glucose + Na⁺
|
[SGLT1 cotransporter on enterocyte]
| ← glucose and Na⁺ enter together
| ← ~264 molecules of water follow by osmosis
|
Enterocyte
|
[GLUT2 on basolateral side]
| → glucose exits into blood
[Na⁺/K⁺-ATPase pumps Na⁺ out]
| → Na⁺ exits into blood
| → water follows Na⁺ into bloodstream
"Fluids containing glucose and electrolytes provide optimal rehydration due to the cotransport of water across the intestinal lumen."
- Rosen's Emergency Medicine
4. Why ORS Osmolarity Matters (245 mOsm/kg)
| Solution | Osmolarity | Problem |
|---|---|---|
| Plain water | ~0 mOsm/kg | Too low - no sodium to drive cotransport; can cause further electrolyte dilution |
| High-glucose drinks (juice, soda) | >350 mOsm/kg | Too high (hypertonic) - draws water INTO the gut instead of absorbing it - worsens diarrhea |
| WHO ORS | 245 mOsm/kg | Just right - slightly hypotonic, maximises cotransport absorption |
"High-glucose solutions have high osmolarity and pure water has low osmolarity; thus neither are optimal for water resorption. Reduced osmolarity ORS (245 mOsm/kg) is associated with reduced need for IV infusions, lower stool volume, and less vomiting."
- Rosen's Emergency Medicine
5. How ORS Helps Muscle Cramps
| ORS Component | What it Restores | How it Stops Cramps |
|---|---|---|
| Sodium (75 mmol/L) | Extracellular Na⁺ | Restores resting membrane potential; stops spontaneous nerve firing |
| Potassium (20 mmol/L) | Intracellular K⁺ | Restores repolarization after contraction; muscle can relax |
| Citrate (base) | Corrects acidosis | Lactic acid/metabolic acidosis worsens cramps; citrate neutralizes it |
| Glucose | Drives water+Na absorption | Rapidly restores blood volume and electrolyte balance via SGLT1 |
| Water (via osmosis) | Intravascular volume | Restores interstitial fluid around muscles; removes metabolic waste |
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - Cholera/ORS, muscle cramps in dehydration
- Yamada's Textbook of Gastroenterology, 7th Ed. - SGLT1, glucose-sodium cotransport, water absorption
- Rosen's Emergency Medicine - ORS osmolarity and optimal rehydration
- WHO ORS composition table (cited in Harrison's)
what is osmomolarity
What is Osmolarity?
Simple Definition
"Osmolarity = the measure of solute concentration per unit volume of solvent."
- Tintinalli's Emergency Medicine
- The more particles dissolved → higher osmolarity → solution pulls water strongly toward itself
- The fewer particles dissolved → lower osmolarity → weaker pull on water
Osmolarity vs Osmolality - What's the Difference?
| Term | Definition | Unit | Used in... |
|---|---|---|---|
| Osmolarity | Solute per unit volume of solution | mOsm/L | Calculated values, ORS |
| Osmolality | Solute per unit mass of solvent | mOsm/kg | Lab reports, clinical medicine |
"Osmolality is the preferred measure because it remains constant with changes in temperature. Osmolarity varies with changing temperature because water changes its volume according to temperature."
- Tintinalli's Emergency Medicine
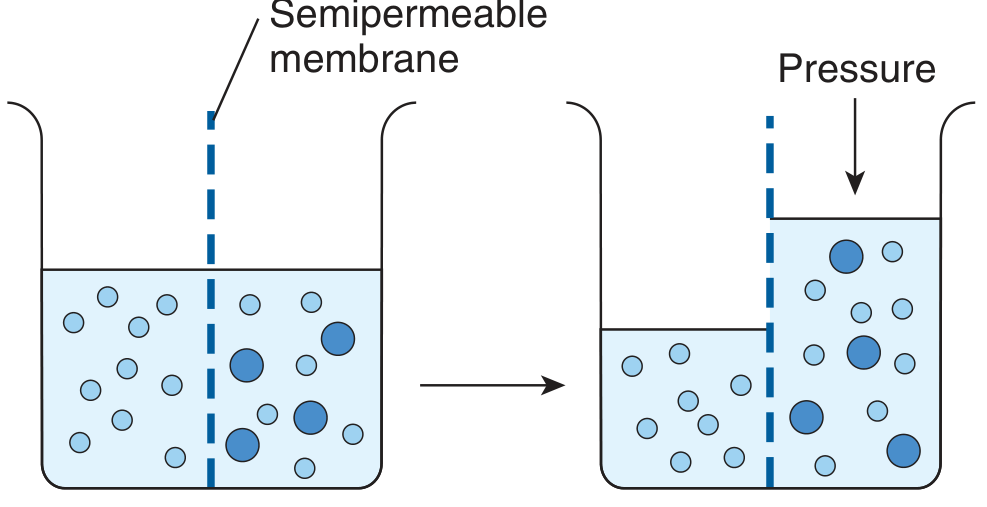
The Concept of Osmosis (The Basis of Osmolarity)
"Osmosis is the net movement of water across a semipermeable membrane as a result of a difference in nondiffusible solute concentrations across the membrane."
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
"The tendency for movement of solvent molecules to a region of greater solute concentration can be prevented by applying pressure to the more concentrated solution. The pressure necessary to prevent solvent migration is the osmotic pressure of the solution."
- Ganong's Review of Medical Physiology, 26th Ed.
What is One Osmole?
"One osmole (Osm) equals the gram-molecular weight of a substance divided by the number of freely moving particles that each molecule liberates in solution. For biological solutions, the milliosmole (mOsm; 1/1000 of 1 Osm) is more commonly used."
- Ganong's Review of Medical Physiology
Key examples:
| Substance | Behaviour in water | Osmoles produced per mole |
|---|---|---|
| Glucose | Does NOT ionize | 1 mol = 1 Osm |
| NaCl | Ionizes into Na⁺ + Cl⁻ | 1 mol = ~2 Osm (actually ~1.86 due to ionic interactions) |
| Na₂SO₄ | Ionizes into 2Na⁺ + SO₄²⁻ | 1 mol = ~3 Osm |
"If a solute is a nonionizing compound such as glucose, the osmotic pressure is a function of the number of glucose molecules present. If the solute ionizes, each ion is an osmotically active particle. NaCl dissociates into Na⁺ and Cl⁻, so that each mole in solution supplies 2 Osm."
- Ganong's Review of Medical Physiology
Normal Body Osmolarity
Effective osmolality = 2 × [Na⁺] + glucose/18 (Normal range: 275-290 mOsm/L)
- Tintinalli's Emergency Medicine
- Sodium contributes the most to blood osmolarity (multiplied by 2 because Na⁺ comes with an anion)
- Glucose also contributes (important in diabetes)
Hypo-, Iso-, and Hypertonic - Related Concepts
| Type | Osmolarity | Effect on a cell placed in it |
|---|---|---|
| Isotonic (e.g., normal saline 0.9%) | ~290 mOsm/L | No change in cell volume - equal pull on both sides |
| Hypotonic (e.g., pure water) | < 290 mOsm/L | Water rushes into the cell → cell swells (may burst) |
| Hypertonic (e.g., concentrated salt water) | > 290 mOsm/L | Water is pulled out of the cell → cell shrinks |
"An isotonic solution has no effect on cell volume, whereas hypotonic and hypertonic solutions increase and decrease cell volume, respectively. Hypertonic plasma draws water out of the cell into the vasculature, causing cell shrinkage. In the setting of hypotonic plasma, cells swell with water."
- Morgan & Mikhail's Clinical Anesthesiology and Tintinalli's Emergency Medicine
Connecting Back to ORS
- It is slightly hypotonic compared to blood (290 mOsm/L)
- So when you drink ORS, the gut contents are less concentrated than the blood
- Water and electrolytes move from gut into blood efficiently
- A solution too concentrated (like juice or soda, >350 mOsm/L) would actually pull water back into the gut, worsening diarrhea
Summary in One Line
- Ganong's Review of Medical Physiology, 26th Ed. - Osmosis, Osmotic Pressure
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed. - Osmolarity, Osmolality & Tonicity
- Tintinalli's Emergency Medicine - Table 17-2: Definitions of Terms
what is mmo/l and mOsm/kg
mmol/L and mOsm/kg - Explained Simply
1. mmol/L (Millimoles per Litre)
What is a Mole first?
"A mole = 6.02 × 10²³ molecules of a substance"
- Tintinalli's Emergency Medicine
- 1 dozen = 12 eggs
- 1 mole = 602,000,000,000,000,000,000,000 particles (6.02 × 10²³)
- 1 mole of carbon = 12 grams (its atomic weight in grams)
- 1 mole of sodium (Na) = 23 grams
- 1 mole of glucose = 180 grams
So what is a Millimole?
- 1 millimole (mmol) = 1/1000 of a mole = 6.02 × 10²⁰ particles
- It is just a smaller, more practical unit used in medicine because body fluid concentrations are tiny
What does mmol/L mean?
Real Examples from Blood Tests:
| Substance | Normal Value | What it means |
|---|---|---|
| Sodium (Na⁺) | 135-145 mmol/L | 135-145 millimoles of sodium in every litre of blood |
| Potassium (K⁺) | 3.5-5.0 mmol/L | 3.5-5 millimoles of potassium per litre |
| Glucose | 4.0-6.0 mmol/L | 4-6 millimoles of glucose per litre (fasting) |
"Sodium is much more concentrated in the ECF (approximately 140 mEq/L) than in the ICF (approximately 10 mEq/L)."
- Tintinalli's Emergency Medicine
2. mOsm/kg (Milliosmoles per Kilogram)
What is an Osmole first?
"One osmole (Osm) equals the gram-molecular weight of a substance divided by the number of freely moving particles that each molecule liberates in solution."
- Ganong's Review of Medical Physiology
- mmol counts molecules
- mOsm counts the actual NUMBER OF FREE PARTICLES produced when those molecules dissolve
Why is this different?
| Substance | 1 mmol dissolved gives... | = how many mOsm? |
|---|---|---|
| Glucose | 1 glucose molecule (stays whole) | 1 mOsm |
| NaCl | Na⁺ + Cl⁻ (breaks into 2 ions) | ~2 mOsm |
| KCl | K⁺ + Cl⁻ (breaks into 2 ions) | ~2 mOsm |
"1 mmol of sodium chloride contributes 2 mOsm (one from sodium and one from chloride)."
- Schwartz's Principles of Surgery, 11th Ed.
What does mOsm/kg mean?
Side-by-Side Comparison
| Feature | mmol/L | mOsm/kg |
|---|---|---|
| Full name | Millimoles per litre | Milliosmoles per kilogram |
| What it counts | Molecules of ONE specific substance | ALL dissolved particles in total |
| Depends on ionization? | No | Yes |
| Used for | Individual electrolyte levels (Na, K, glucose) | Overall osmotic strength of a solution |
| Normal blood value | Na: 135-145 mmol/L | 275-290 mOsm/kg |
Easy Analogy
- mmol/L asks: "How many NaCl molecules did you put in?"
- mOsm/kg asks: "How many actual particles (Na⁺ + Cl⁻) are floating around pulling water?"
Connecting to ORS
- Glucose: 75 mmol/L → contributes 75 mOsm (does not ionize)
- Na⁺: 75 mmol/L → contributes 75 mOsm
- K⁺: 20 mmol/L → contributes 20 mOsm
- Cl⁻: 65 mmol/L → contributes 65 mOsm
- Citrate: 10 mmol/L → contributes 10 mOsm
- Total = 245 mOsm/kg ✓
- Tintinalli's Emergency Medicine - Table 17-2: Definitions of Terms (Mole, Osmole, Osmolarity, Osmolality)
- Ganong's Review of Medical Physiology, 26th Ed. - Osmoles and Milliosmoles
- Schwartz's Principles of Surgery, 11th Ed. - Fluid and Electrolytes, Osmolality
Intramuscular site of diclofenac
Intramuscular (IM) Site for Diclofenac Injection
The Drug First - What is Diclofenac IM?
"Diclofenac is a phenylacetic acid derivative that is a relatively nonselective COX inhibitor. It is available as sodium, potassium, and epolamine salts. In Europe, diclofenac is also available for intramuscular administration."
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Acute severe pain (renal colic, biliary colic, post-operative pain)
- Acute musculoskeletal pain
- Migraine
- Acute gout
The IM Injection Site
Upper Outer Quadrant of the Gluteal Region (Buttock)
How to Find the Safe Zone
|
Upper | Upper
Outer | Inner
(SAFE) | (UNSAFE)
---------+----------
Lower | Lower
Outer | Inner
|
Why? - Anatomy of the Gluteal Region
- Sciatic nerve - runs from lower inner quadrant downward into the thigh
- Superior gluteal vessels and nerve - run in the upper region but are safe in the outer part
- Inferior gluteal nerve and vessels - in lower portion
The upper outer quadrant is the safe zone because it is farthest from the sciatic nerve, the superior gluteal nerve, and major gluteal blood vessels.
Landmark Method (for Accurate Identification):
Alternative Site - Ventrogluteal (Preferred in Modern Practice)
- Place your hand so the palm is on the greater trochanter
- Point your index finger to the ASIS (anterior superior iliac spine)
- Spread your middle finger posteriorly along the iliac crest
- Inject in the V-shaped area between index and middle fingers
- Thicker muscle mass
- No major nerves or vessels nearby
- Less subcutaneous fat in this area
- Better drug absorption
Important Points for Diclofenac IM Specifically
| Point | Detail |
|---|---|
| Dose | 75 mg IM (single dose), maximum 150 mg/day |
| Volume | Not more than 3 mL per injection site |
| Only gluteal site | Never give in deltoid or thigh - too painful, risk of local necrosis |
| Deep injection | Must go deep into muscle, not into subcutaneous fat |
| Rotate sites | If repeated doses needed, alternate left and right sides |
| Never give IV | Diclofenac IM formulation must NOT be given intravenously |
| Duration of IM use | Maximum 2 days IM, then switch to oral form |
Why NOT Other Sites?
| Site | Why Avoided for Diclofenac |
|---|---|
| Deltoid (arm) | Small muscle, not enough mass; risk of severe local pain and tissue damage |
| Vastus lateralis (thigh) | Used for vaccines in infants but NOT for irritant drugs like diclofenac |
| Lower inner gluteal | Risk of sciatic nerve injury → foot drop, permanent paralysis |
Summary
- Katzung's Basic and Clinical Pharmacology, 16th Ed. - Diclofenac (pharmacology, routes of administration)
- Gray's Anatomy - Gluteal region anatomy, sciatic nerve course
- Clinical practice guidelines - IM injection technique (dorsogluteal and ventrogluteal landmarks)
tell me about bone tumor in metaphysis,epiphysis and dyphysis
Bone Tumors by Location: Metaphysis, Epiphysis, Diaphysis
Parts of a Long Bone (Quick Recap)
┌──────────┐
│ EPIPHYSIS │ ← end of bone (beyond growth plate)
├──────────┤
│ METAPHYSIS│ ← flared region just below growth plate
│ │
│ DIAPHYSIS │ ← shaft (middle long portion)
│ │
│ METAPHYSIS│
├──────────┤
│ EPIPHYSIS │
└──────────┘
Master Table - Tumor Location in Bone
From Schwartz's Principles of Surgery, 11th Ed. (Table 43-2):
| Location | Tumors Found |
|---|---|
| Epiphysis | Chondroblastoma, Clear cell chondrosarcoma, Giant Cell Tumor (GCT), Infection, Dysplasia epiphysealis hemimelica |
| Metaphysis | Most common site - Osteosarcoma, Osteochondroma, Osteoid osteoma, Giant Cell Tumor (extends from epiphysis), Chondrosarcoma, Aneurysmal Bone Cyst |
| Diaphysis | Mnemonic: FENOMAISH - Fibrous dysplasia, Eosinophilic Granuloma, Nonossifying Fibroma, Osteoid osteoma, Myeloma, Adamantinoma, Infection, Simple Bone Cyst, Histiocytosis |
1. EPIPHYSIS Tumors
A. Chondroblastoma (Benign)
- Location: Epiphysis of long bones (before growth plate closure)
- Age: 10-20 years
- Key features: Circumscribed lesion with characteristic pericellular ("chicken-wire") calcification on histology
- Presents with joint pain, often mistaken for arthritis
- Treated by curettage and bone grafting
"Chondroblastoma: Epiphysis of long bones, age 10-20, circumscribed with pericellular calcification."
- Robbins Pathologic Basis of Disease
B. Giant Cell Tumor (GCT) - also called Osteoclastoma
- Location: Epiphysis of long bones (most commonly distal femur, proximal tibia, distal radius) - always extends to the subchondral bone (right under the joint cartilage)
- Age: 20-40 years; more common in females
- Key features: Sheets of mononuclear stromal cells with scattered multinucleate giant cells (osteoclast-like)
- Locally aggressive - "soap bubble" appearance on X-ray
- Can be benign but has malignant potential
"Giant Cell Tumor: Epiphysis of long bones, age 20-40, destroys medulla and cortex, sheets of mononuclear stromal cells with scattered multinucleate giant cells."
- Robbins Pathologic Basis of Disease
"Giant cell tumor is more common in females."
- Schwartz's Principles of Surgery, 11th Ed.
C. Clear Cell Chondrosarcoma (Malignant)
- Rare malignant variant
- Located in epiphysis of proximal femur or proximal humerus
- Low grade but locally destructive
2. METAPHYSIS Tumors
"Metaphysis: Most common site of involvement."
- Schwartz's Principles of Surgery, 11th Ed.
A. Osteosarcoma (Most Common Primary Malignant Bone Tumor)
- Location: Metaphysis of long bones - distal femur (most common), proximal tibia, proximal humerus
- Age: Bimodal - peak at 10-20 years (primary); second peak in older adults (secondary - associated with Paget's disease)
- Sex: Males > Females (1.6:1)
- Key features:
- Produces osteoid/woven bone
- Codman's triangle - periosteal reaction on X-ray (periosteum lifted by tumor)
- Sunburst pattern on X-ray
- Alkaline phosphatase elevated
- Metastasizes to lungs first
"Although any bone can be involved, tumors usually arise in the metaphyseal region of the long bones; almost 50% are near the knee in the distal femur or proximal tibia."
- Robbins Pathologic Basis of Disease
"Osteosarcomas are classified as osteoblastic, chondroblastic, fibroblastic, telangiectatic... Most osteosarcomas present in patients between 10 and 20 years of age."
- Schwartz's Principles of Surgery, 11th Ed.
"The peak incidence of osteosarcoma is during the adolescent growth spurt. The tumor occurs most frequently in the growth plate of rapidly growing bones, where increased proliferation may predispose to mutations."
- Robbins Pathologic Basis of Disease
B. Osteochondroma (Most Common Benign Bone Tumor)
- Location: Metaphysis of long bones (distal femur, proximal tibia, proximal humerus)
- Age: 10-30 years
- Key features: Bony excrescence (outgrowth) with a cartilage cap pointing away from the joint
- Usually solitary; multiple = hereditary multiple exostoses (autosomal dominant)
- Risk of malignant transformation into chondrosarcoma (rare, <1%)
"Osteochondroma: Metaphysis of long bones, age 10-30, bony excrescence with cartilage cap."
- Robbins Pathologic Basis of Disease
C. Osteoid Osteoma (Benign)
- Location: Cortex of metaphysis/diaphysis of femur or tibia (50% of cases)
- Age: Young males predominantly
- Key features:
- Severe nocturnal pain relieved by aspirin/NSAIDs (due to PGE2 production)
- Small lesion < 2 cm with radiolucent nidus surrounded by reactive sclerotic bone
- Treated by radiofrequency ablation
"About 50% of cases involve the cortex of the femur or tibia. Severe nocturnal pain... is relieved by aspirin and other NSAIDs."
- Robbins Pathologic Basis of Disease
D. Aneurysmal Bone Cyst
- Location: Metaphysis of long bones and posterior spine
- Age: <20 years
- Blood-filled cystic spaces; "blown out" expansile lesion on X-ray
3. DIAPHYSIS Tumors
| Letter | Tumor |
|---|---|
| F | Fibrous dysplasia |
| E | Eosinophilic Granuloma (Langerhans cell histiocytosis) |
| N | Nonossifying Fibroma |
| O | Osteoid osteoma |
| M | Myeloma (Multiple myeloma) |
| A | Adamantinoma |
| I | Infection (osteomyelitis) |
| S | Simple (Unicameral) Bone Cyst |
| H | Histiocytosis |
Key Diaphysis Tumor - Ewing's Sarcoma
- Location: Diaphysis of long bones (femur, tibia, fibula) and flat bones (pelvis, ribs, scapula)
- Age: 5-20 years (most common malignant bone tumor in children under 10)
- Key features:
- "Onion skin" periosteal reaction on X-ray - layers of periosteum lifted
- Small round blue cells on histology - looks like lymphoma, neuroblastoma
- Associated with t(11;22) chromosomal translocation
- Presents with pain, fever, raised ESR (can mimic osteomyelitis)
"Ewing's sarcoma has a characteristic 'onion skin' periosteal reaction pattern."
- Schwartz's Principles of Surgery, 11th Ed.
"Round blue cell lesions are most likely neuroblastoma in a 5-year-old, Ewing's sarcoma in a 10-year-old, lymphoma in a 20-year-old, and myeloma in a 60-year-old."
- Schwartz's Principles of Surgery, 11th Ed.
Multiple Myeloma
- Location: Diaphysis and axial skeleton (vertebrae, skull, ribs, pelvis)
- Age: >60 years
- Key features: "Punched out" lytic lesions; Bence Jones protein in urine; monoclonal protein spike
Quick Summary Table
| Location | Benign Tumors | Malignant Tumors | Memory Clue |
|---|---|---|---|
| Epiphysis | Chondroblastoma, GCT | Clear cell chondrosarcoma | "E for End - GCT and Chondroblastoma at the End" |
| Metaphysis | Osteochondroma, Osteoid osteoma, Aneurysmal BC | Osteosarcoma, Chondrosarcoma | "Most common site - Met = Most" |
| Diaphysis | Fibrous dysplasia, Simple BC, Nonossifying fibroma | Ewing's sarcoma, Myeloma, Adamantinoma | "FENOMAISH" mnemonic |
Age-Based Differential (Bonus for PBL)
| Age | Most Likely Tumor |
|---|---|
| 5 years | Neuroblastoma (metastasis) |
| 10 years | Ewing's sarcoma |
| 10-20 years | Osteosarcoma |
| 20-40 years | Giant Cell Tumor |
| >60 years | Myeloma, Metastasis (prostate, breast, lung, kidney, thyroid) |
"The predilection of specific types of tumors to affect certain age groups and particular anatomic sites provides a diagnostic clue."
- Robbins Pathologic Basis of Disease
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (Latest Ed.) - Table 26.4: Classification of Primary Bone Tumors; Osteosarcoma, GCT, Chondroblastoma
- Schwartz's Principles of Surgery, 11th Ed. - Table 43-2: Tumor Location in Bone; Osteosarcoma; Ewing's Sarcoma
now tell me about osteosarcoma
Osteosarcoma - Complete Overview
Definition
"Osteosarcoma is a malignant tumor that produces osteoid matrix or mineralized bone. Excluding hematopoietic tumors, osteosarcoma is the most common primary malignant tumor of bone."
- Robbins & Kumar Basic Pathology
"Osteosarcoma is a tumor characterized by the production of osteoid by malignant cells."
- Campbell's Operative Orthopaedics, 15th Ed. (2026)
Epidemiology
| Feature | Detail |
|---|---|
| Incidence | ~4 per million population per year |
| Most common | Most common primary non-haematological malignant bone tumor |
| Age | Bimodal - 75% under 20 years (peak: 10-20 yrs); second peak in older adults (secondary) |
| Sex | Males > Females (1.6:1) overall; exception: parosteal type is more common in females |
| Race | No significant racial difference |
"The age distribution is bimodal, with about 75% occurring before 20 years of age, while a second smaller peak occurs in older adults in the setting of predisposing factors such as Paget disease, bone infarcts, and previous radiation."
- Robbins & Kumar Basic Pathology
Location
- Bone: Metaphysis of long bones (sites of most rapid growth)
- Most common bones: Distal femur > Proximal tibia > Proximal humerus
- ~50% occur around the knee
- ~10% are diaphyseal; <1% are epiphyseal
"Most primary osteosarcomas occur at the sites of the most rapid bone growth, including the distal femur, the proximal tibia, and the proximal humerus."
- Campbell's Operative Orthopaedics, 15th Ed.
Classification (WHO 2013)
"In 2013, the WHO Committee for the Classification of Bone Tumours divided them into seven distinct categories."
- Grainger & Allison's Diagnostic Radiology
| Type | Key Feature |
|---|---|
| 1. Conventional osteosarcoma | Most common (75%); high-grade intramedullary |
| 2. Telangiectatic osteosarcoma | Blood-filled spaces; looks like aneurysmal bone cyst |
| 3. Low-grade central osteosarcoma | Intramedullary, well-differentiated |
| 4. Small cell osteosarcoma | Resembles Ewing's sarcoma |
| 5. Parosteal osteosarcoma | Surface tumor, LOW grade, posterior distal femur, better prognosis |
| 6. Periosteal osteosarcoma | Surface tumor, intermediate grade |
| 7. High-grade surface osteosarcoma | Surface, high grade |
- Osteoblastic (most common)
- Chondroblastic
- Fibroblastic
Predisposing Conditions (Secondary Osteosarcoma)
"Secondary osteosarcomas occur in older patients in abnormal bone affected by Paget's disease, radiation, or bone infarct."
- Schwartz's Principles of Surgery
- Li-Fraumeni syndrome (TP53 germline mutation)
- Hereditary retinoblastoma (RB mutation - 1000-fold increased risk)
- Rothmund-Thomson syndrome
Pathogenesis / Molecular Biology
"RB mutations are present in up to 70% of sporadic osteosarcomas; germline RB mutations increase risk 1000-fold."
"TP53 is mutated in Li-Fraumeni syndrome. CDKN2A (p16 and p14) is inactivated in many osteosarcomas. MDM2 and CDK4, which inhibit p53 and RB, are overexpressed in low-grade osteosarcomas. MYC amplification is seen in up to half of cases and may be associated with particularly poor prognosis."
- Robbins & Kumar Basic Pathology
Clinical Features
| Feature | Detail |
|---|---|
| Pain | Progressive, initially activity-related → later constant, night pain is an important clue |
| Swelling/mass | Progressively enlarging, firm, tender mass |
| Pathologic fracture | May be the first presentation |
| Systemic | Usually no fever (unlike Ewing's) |
| Alkaline phosphatase | Elevated (marker of bone turnover) |
| LDH | Elevated (marker of cellular turnover) |
"Almost all patients with high-grade osteosarcoma report progressive pain. Night pain may be an important clue to the true diagnosis. The average delay from onset of symptoms to correct diagnosis was approximately 15 weeks."
- Campbell's Operative Orthopaedics, 15th Ed.
Radiology (X-ray Findings)
| X-ray Sign | What it Means |
|---|---|
| Codman's Triangle | Periosteum lifted by tumor → reactive bone forms a triangle at the edge; indicates aggressive tumor |
| Sunburst pattern | Tumor breaking through cortex with radiating bone spicules in soft tissue |
| Hair-on-end pattern | Variant periosteal reaction |
| Mixed lytic and sclerotic | Areas of bone destruction + bone formation (most common pattern) |
| Soft tissue mass | Tumor has broken through cortex |
| Ill-defined borders | Aggressive, permeative tumor |

"The most common appearance is that of an aggressive lesion in the metaphysis of a long bone. Periosteal reaction may take the form of a 'Codman triangle,' or it may have a 'sunburst' or 'hair-on-end' appearance."
- Campbell's Operative Orthopaedics, 15th Ed.
Investigations
| Investigation | Purpose |
|---|---|
| Plain X-ray | First investigation - characteristic appearance |
| MRI | Best for extent within bone, soft tissue involvement, relationship to neurovascular structures |
| CT chest | Look for lung metastases (lungs = most common site of metastasis) |
| Bone scan | Look for skip lesions and bone metastases |
| PET-CT | Superior to bone scan for bone metastases detection |
| Alkaline phosphatase, LDH | Elevated; used for monitoring |
| Biopsy | Definitive diagnosis - must be done after staging, by the same surgeon who will operate |
"MRI is the best imaging modality to measure the extent of the tumor within the bone and soft tissue. CT of the chest should be done to search for pulmonary metastases; the lungs are the most common sites of metastases. These tests should be done before biopsy."
- Campbell's Operative Orthopaedics, 15th Ed.
Morphology / Histopathology
"Osteosarcomas are bulky tumors that are gritty and tan-white, often with areas of hemorrhage, and tend to destroy the surrounding cortices and invade into soft tissue."
"The tumor cells demonstrate pleomorphism, large hyperchromatic nuclei, bizarre tumor giant cells, and abundant mitoses including abnormal forms. Diagnosis of osteosarcoma requires the presence of malignant tumor cells producing unmineralized osteoid or mineralized bone, which is typically fine and lace-like."
- Robbins & Kumar Basic Pathology
Treatment
| Step | Treatment |
|---|---|
| 1. Neoadjuvant chemotherapy (before surgery) | Shrinks tumor, treats micrometastases, assesses tumor response |
| 2. Wide surgical resection | Limb-salvage surgery (preferred) or amputation |
| 3. Adjuvant chemotherapy (after surgery) | Kills remaining cancer cells |
"Treatment generally includes neoadjuvant chemotherapy, surgery, and postoperative adjuvant chemotherapy."
- Robbins & Kumar Basic Pathology
"Treatment of osteosarcoma will be preoperative chemotherapy and wide resection, followed by postoperative chemotherapy. Young patients may present with pain and swelling, with X-rays showing plastic lesions in some areas of destruction with periosteal reaction called 'Codman's Triangle.'"
- Schwartz's Principles of Surgery, 11th Ed.
Prognosis
| Situation | 5-Year Survival |
|---|---|
| Non-metastatic at diagnosis (with chemotherapy) | ~70% |
| Metastatic / recurrent / secondary | < 20% |
"Chemotherapy has greatly improved osteosarcoma prognosis, with 5-year survival reaching 70% in individuals without overt metastases at initial diagnosis."
- Robbins & Kumar Basic Pathology
- Response to neoadjuvant chemotherapy (98% necrosis = good response = better prognosis)
- Stage at diagnosis (presence of metastases)
- Surgical margins achieved
- Tumor size and location
Skip Lesions
"It can metastasize to the bone, which is called a 'skip lesion,' but the lung is the primary site of metastases. MRI should involve the entire bone to diagnose skip metastasis."
- Schwartz's Principles of Surgery, 11th Ed.
Summary at a Glance
| Feature | Osteosarcoma |
|---|---|
| Definition | Malignant tumor producing osteoid |
| Most common | Primary malignant bone tumor |
| Age | 10-20 years (primary) |
| Sex | Male > Female |
| Location | Metaphysis, distal femur/proximal tibia |
| X-ray | Codman's triangle + sunburst pattern |
| Histology | Malignant cells + lace-like osteoid |
| Metastasis | Lungs (first), then bone |
| Treatment | Neoadjuvant chemo + surgery + adjuvant chemo |
| Prognosis | 70% 5-year survival (no metastases) |
- Robbins & Kumar Basic Pathology - Osteosarcoma (definition, epidemiology, pathogenesis, morphology, prognosis)
- Campbell's Operative Orthopaedics, 15th Ed. (2026) - Clinical presentation, imaging, treatment
- Schwartz's Principles of Surgery, 11th Ed. - Classification, imaging, treatment
- Grainger & Allison's Diagnostic Radiology - WHO classification, types
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Molecular genetics
normal range of esr
ESR (Erythrocyte Sedimentation Rate)
What is ESR?
"The erythrocyte sedimentation rate (ESR) is one of the oldest laboratory tests still in clinical use. The test measures the distance that erythrocytes (RBCs) fall in a column of anticoagulated blood in 1 hour."
- Textbook of Family Medicine, 9th Ed.
Normal Range of ESR
By Age and Sex (Westergren Method - the standard reference method):
| Group | Normal ESR |
|---|---|
| Newborn (0 to <1 month) | ≤ 2 mm/hr |
| Infant/Child (1 month - 12 years) | ≤ 20 mm/hr |
| Adult Male (>12 years) | ≤ 15 mm/hr |
| Adult Female (>12 years) | ≤ 20 mm/hr |
">12 years (male) ≤15 mm/hr; >12 years (female) ≤20 mm/hr"
- Harriet Lane Handbook, 23rd Ed. (Johns Hopkins)
Age-Adjusted Formula for Adults (Practical Rule):
"To determine ESR for healthy adult men, age in years is divided by 2, and for women, age in years plus 10 is divided by 2."
- Textbook of Family Medicine, 9th Ed.
| Sex | Formula | Example (50 years old) |
|---|---|---|
| Male | Age ÷ 2 | 50 ÷ 2 = 25 mm/hr |
| Female | (Age + 10) ÷ 2 | (50 + 10) ÷ 2 = 30 mm/hr |
How is ESR Measured? (Westergren Method)
"The Westergren method is widely used and has been recommended by the ICSH as the reference method. When well-mixed venous blood is placed in a vertical tube, erythrocytes fall toward the bottom. The length of fall of the top of the column of erythrocytes over a given interval (1 hour) is called the ESR."
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Blood is placed in a tall, vertical Westergren tube
- Left to stand for exactly 1 hour
- Distance (in mm) that RBCs fall = ESR in mm/hr
Why Does ESR Change? (Mechanism)
"Plasma proteins (fibrinogen, globulins) decrease the negative charge of erythrocytes (zeta potential) that keeps them apart. The decreased zeta potential promotes rouleaux formation, which sediment more rapidly than single cells."
- Henry's Clinical Diagnosis and Management
Factors That ALTER ESR
(From Textbook of Family Medicine, 9th Ed.)
| Increases ESR | Decreases ESR | No Effect |
|---|---|---|
| Anemia | Polycythemia | Body temperature |
| Macrocytosis | Microcytosis | Recent meal |
| Female gender | Spherocytosis | Aspirin |
| Advanced age | Extreme leukocytosis | NSAIDs |
| 2nd & 3rd trimester pregnancy | Sickle cell disease | 1st trimester pregnancy |
| Hypoalbuminemia | Excessive anticoagulant | |
| Tilted ESR tube | Short ESR tube | |
| High room temperature | Low room temperature / clotted blood |
Clinical Significance - When is ESR Elevated?
"Inflammatory, infectious, neoplastic, and collagen vascular diseases increase the ESR."
- Textbook of Family Medicine, 9th Ed.
| Cause | Example |
|---|---|
| Infection | Tuberculosis, osteomyelitis, bacterial endocarditis |
| Inflammation | Rheumatoid arthritis, SLE |
| Malignancy | Osteosarcoma, Ewing's sarcoma, multiple myeloma, lymphoma |
| Polymyalgia rheumatica/Temporal arteritis | ESR often >100 mm/hr (mean ESR ~90 mm/hr) |
| Anemia | Any cause |
| Pregnancy | 2nd and 3rd trimester |
- Temporal arteritis / polymyalgia rheumatica
- Multiple myeloma
- Severe infection (TB, osteomyelitis)
- Malignancy
Important Limitations
"ESR is both nonsensitive and nonspecific. It should not be used as a screening test for disease in asymptomatic persons. The underlying cause of an elevated ESR is usually apparent from the history and physical examination."
- Textbook of Family Medicine, 9th Ed.
- ESR is a nonspecific marker - it goes up in many conditions
- A normal ESR does NOT rule out serious disease (e.g., 4% of temporal arteritis patients have normal ESR)
- More specific markers like CRP (C-reactive protein) are now preferred for many conditions
Summary
| Value | |
|---|---|
| Unit | mm/hour |
| Method | Westergren (gold standard) |
| Adult Male | ≤ 15 mm/hr (or Age ÷ 2) |
| Adult Female | ≤ 20 mm/hr (or [Age+10] ÷ 2) |
| Child (1 mo - 12 yr) | ≤ 20 mm/hr |
| Newborn | ≤ 2 mm/hr |
| Very elevated (>100) | Temporal arteritis, myeloma, TB, malignancy |
- Harriet Lane Handbook, 23rd Ed. (Johns Hopkins Hospital) - ESR normal values by age and sex
- Textbook of Family Medicine, 9th Ed. - ESR clinical use, factors affecting, normal values, formula
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Westergren method, mechanism of rouleaux formation
what is mm/hr?
What is mm/hr?
Breaking It Down
| Part | Meaning |
|---|---|
| mm | millimetre - a unit of length (1 mm = 1/1000 of a metre) |
| hr | hour - a unit of time |
| mm/hr | how many millimetres of distance are covered in 1 hour |
In the Context of ESR
- Blood is placed in a tall vertical Westergren tube (200 mm long)
- You leave it for exactly 1 hour
- You then measure how far (in mm) the red blood cells have fallen down the tube
Top of tube
| ← RBCs start here
|
| ← RBCs fall this far in 1 hour
| = 15 mm
| ← top of RBC column after 1 hour
|
|
|
Bottom of tube (where RBCs collect)
Simple Analogy
diff between refer pain, radiation and migratory pain in short
Referred Pain vs Radiating Pain vs Migratory Pain
1. Referred Pain
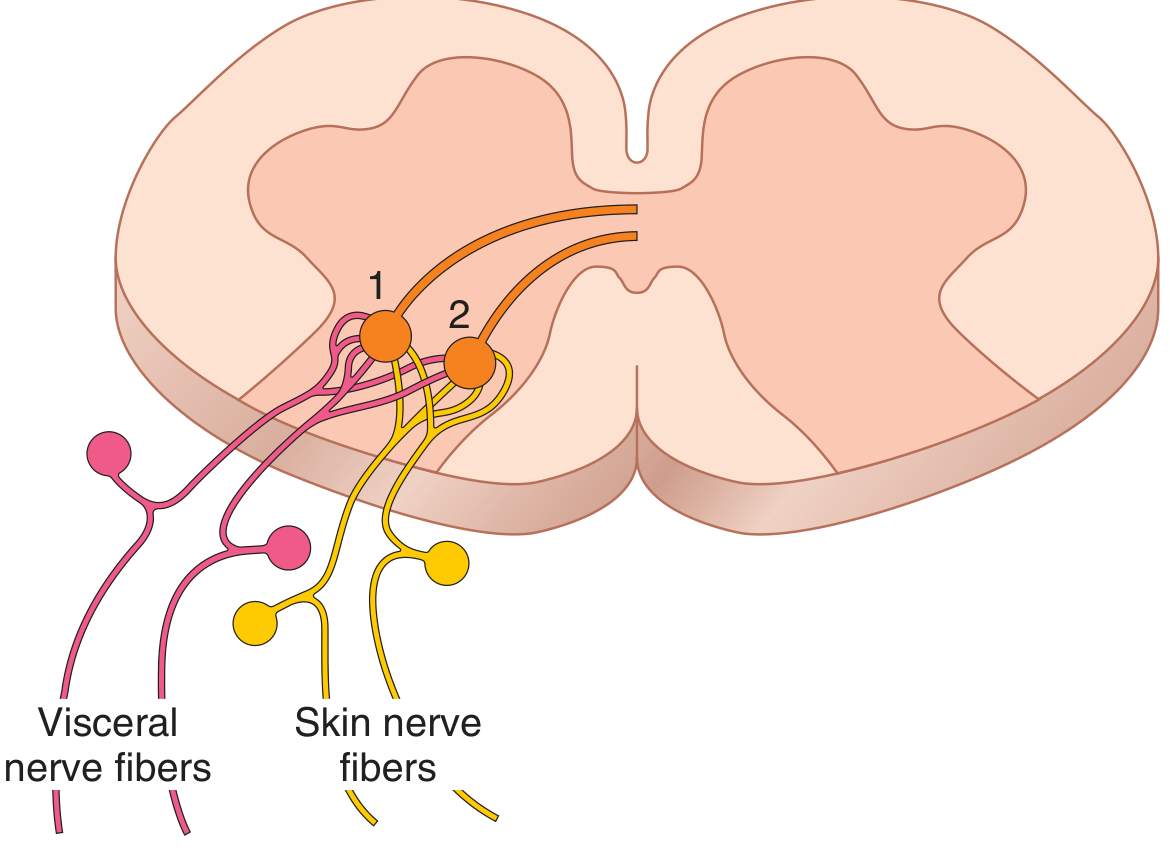
"Sometimes a person feels pain in a part of the body that is fairly remote from the tissue causing the pain. This phenomenon is called referred pain."
- Guyton & Hall Textbook of Medical Physiology
"Visceral pain fibers synapse in the spinal cord on the same second-order neurons that receive pain signals from the skin. When visceral pain fibers are stimulated, pain signals are conducted through the same neurons that conduct pain from the skin - so the person feels the pain as coming from the skin."
- Guyton & Hall
- Pain is felt at a fixed, predictable distant site
- The painful site is not the actual source of the problem
- Pain does NOT travel - it is felt directly at the referred site
- The original source and referred site share the same spinal cord segment
| Organ Affected | Referred Pain Site |
|---|---|
| Heart (MI) | Left arm, jaw, left shoulder |
| Appendix (early) | Umbilicus (T10 dermatome) |
| Diaphragm irritation | Tip of shoulder (C3, C4) |
| Gallbladder | Right shoulder tip |
| Kidney/ureter | Groin, inner thigh |
"When the appendix initially becomes inflamed, visceral fibers enter at T10. The pain is referred to the T10 dermatome = umbilical region."
- Gray's Anatomy for Students
2. Radiating Pain (Radiation of Pain)
- Pain starts at the source and travels along a nerve to a distant site
- Follows a specific nerve or dermatome path
- Both the origin AND the path of radiation are painful
- Caused by direct nerve compression or irritation
- Sharp, shooting, electric in quality
| Cause | Radiation Pattern |
|---|---|
| Sciatica (L4/L5/S1 disc herniation) | Pain starts in lower back → travels down buttock → thigh → leg → foot |
| Cervical disc prolapse | Pain from neck → shoulder → arm → fingers |
| Renal colic | Loin → radiates to groin along the course of ureter |
| Angina | Chest pain → radiates to left arm/jaw |
3. Migratory Pain
- Pain shifts location - one joint/area hurts, then that stops, and another area begins to hurt
- The old site resolves as the new site becomes painful
- No continuous path - pain just relocates
- Typically involves multiple joints sequentially
| Condition | Pattern |
|---|---|
| Rheumatic fever | Migratory polyarthritis - pain moves from joint to joint (knee → ankle → wrist) |
| Gonococcal arthritis | Pain migrates between joints |
| Reactive arthritis | Asymmetric migratory joint involvement |
| Appendicitis | Pain starts at umbilicus (referred/visceral) → migrates to right iliac fossa (somatic) |
Side-by-Side Comparison Table
| Feature | Referred Pain | Radiating Pain | Migratory Pain |
|---|---|---|---|
| Origin | Visceral organ or deep structure | Nerve root/compressed nerve | Joint or region |
| Where felt | Fixed distant site (predictable) | Along a nerve path from origin | Different sites at different times |
| Does pain travel? | No - appears directly at distant site | Yes - spreads along nerve route | No - it relocates |
| Old site still hurts? | Yes (original organ hurts too) | Yes (origin + whole path hurts) | No - old site resolves |
| Mechanism | Convergence of visceral + somatic neurons in spinal cord | Direct nerve compression/irritation | Inflammation moves between sites |
| Quality | Dull, aching | Sharp, shooting, electric | Variable |
| Classic example | Heart attack → left arm pain | Sciatica → down the leg | Rheumatic fever → joint to joint |
Simple Memory Aid
| Type | Think of it as... |
|---|---|
| Referred | Brain gets the wrong address - pain signal from organ A is delivered to skin area B |
| Radiating | Pain travels like electricity along a wire (nerve) from source outward |
| Migratory | Pain moves house - leaves one joint and sets up in another |
- Guyton & Hall Textbook of Medical Physiology - Referred Pain (mechanism, convergence theory)
- Gray's Anatomy for Students - Referred pain (appendicitis example, viscerosomatic convergence)
Coris Cycle
Cori Cycle (Lactic Acid Cycle)
Definition
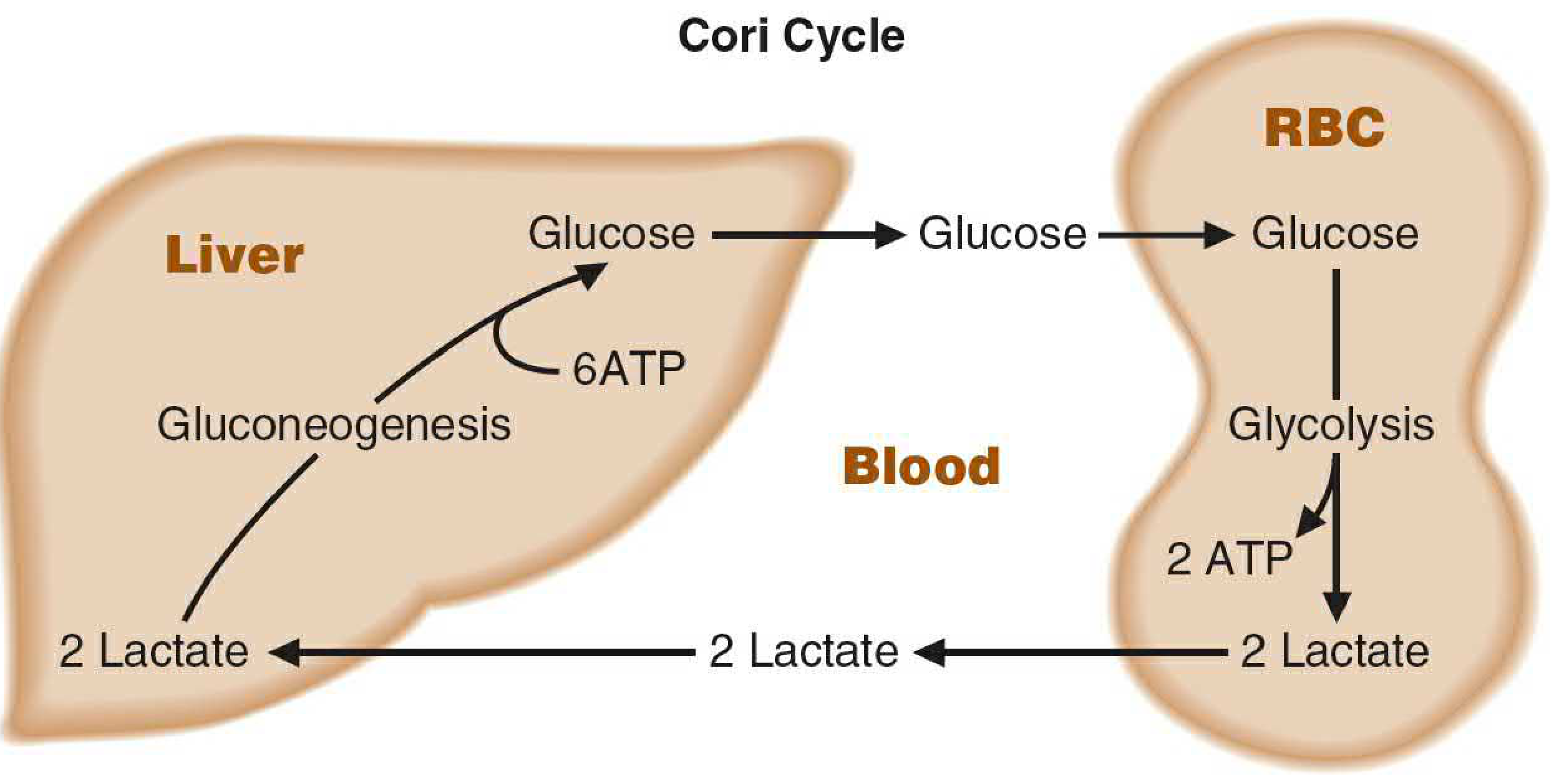
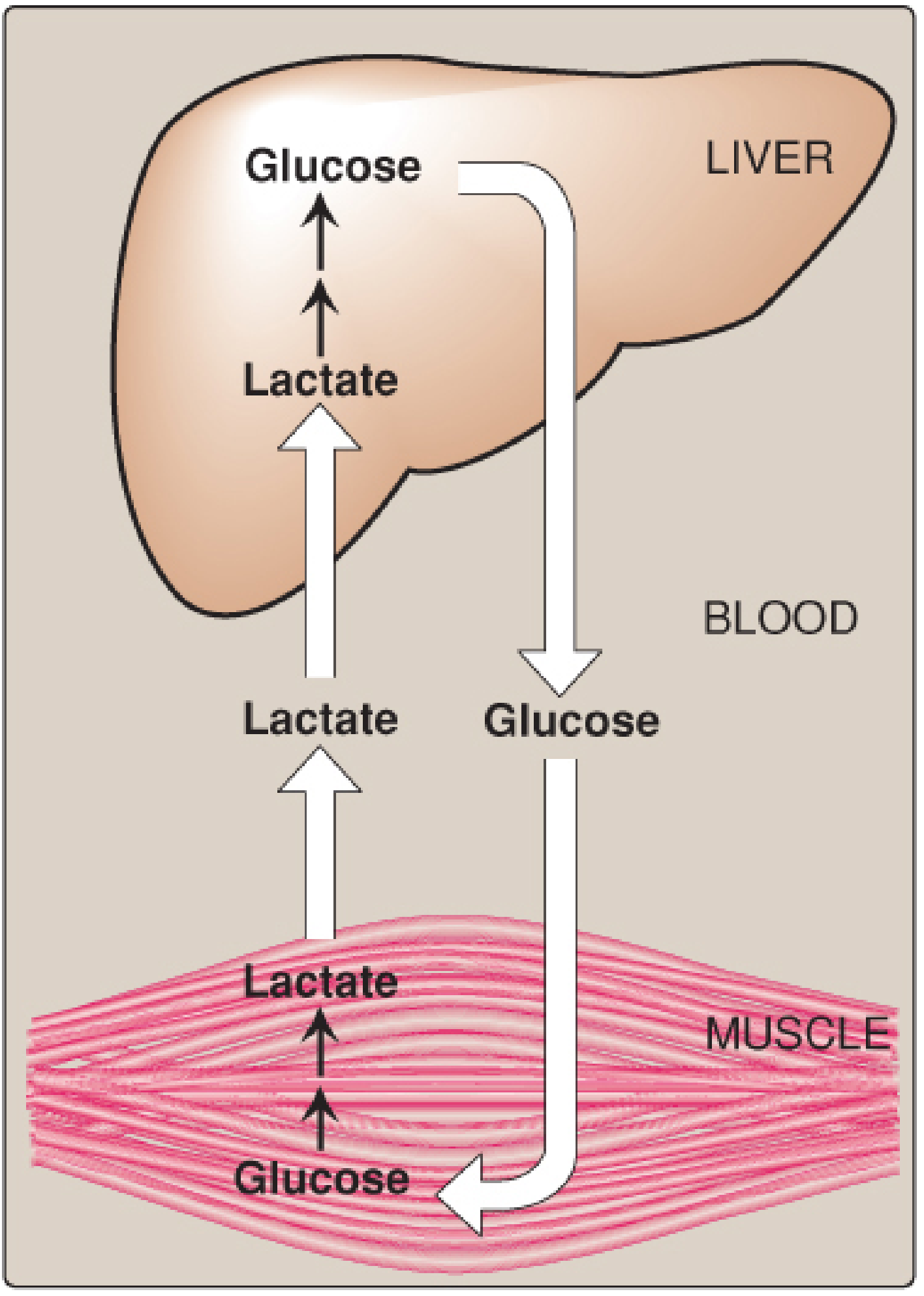
"The cycling of lactate and glucose between peripheral tissues and the liver is called the Cori cycle."
- Basic Medical Biochemistry, 6th Ed.
"The Cori cycle (or lactic acid cycle) resynthesizes glucose that has been partially metabolized to lactate by peripheral tissues. Lactate produced principally by muscle, erythrocytes, and adipose tissue is transported to the liver and kidneys, where it is converted to glucose."
- Yamada's Textbook of Gastroenterology, 7th Ed.
Why Does the Cori Cycle Exist?
The Two Organs Involved
| Organ | What it Does |
|---|---|
| Muscle / RBCs | Glucose → Lactate (anaerobic glycolysis) - produces 2 ATP |
| Liver | Lactate → Glucose (gluconeogenesis) - consumes 6 ATP |
Step-by-Step Pathway
In Muscle / RBCs (Anaerobic Glycolysis):
Glucose (6C)
↓ Glycolysis (10 steps)
Pyruvate (3C)
↓ Lactate dehydrogenase (LDH)
[NADH → NAD+]
Lactate (3C)
↓ Released into blood
- Net gain: 2 ATP per glucose
- NAD⁺ is regenerated (important - allows glycolysis to keep running)
- Lactate enters the bloodstream
In the Liver (Gluconeogenesis):
Lactate (from blood)
↓ Lactate dehydrogenase (LDH)
[NAD+ → NADH]
Pyruvate
↓ Gluconeogenesis (reverse of glycolysis, with bypasses)
Key enzymes: Pyruvate carboxylase → PEPCK → Fructose-1,6-bisphosphatase → Glucose-6-phosphatase
Glucose
↓ Released back into blood → taken up by muscle again
- Net cost: 6 ATP per glucose
- Glucose is released back into the bloodstream
Diagrams
ATP Balance (Energy Economics)
| Site | Process | ATP |
|---|---|---|
| Muscle/RBC | Glycolysis: Glucose → 2 Lactate | +2 ATP (gained) |
| Liver | Gluconeogenesis: 2 Lactate → Glucose | -6 ATP (consumed) |
| Net | -4 ATP overall |
"Glucose, produced in the liver by gluconeogenesis, is converted by glycolysis in muscle, RBCs, and many other cells to lactate. Lactate returns to the liver and is reconverted to glucose by gluconeogenesis. ATP consumed = 6; ATP produced = 2."
- Basic Medical Biochemistry, 6th Ed.
- The muscle gets immediate ATP for contraction even without oxygen
- The liver pays the energy cost using fatty acid oxidation
- The net result is that the body keeps muscles working during intense exercise
Tissues That Produce Lactate (Send to Liver)
"Large quantities of lactate are made from active skeletal muscles and erythrocytes. Lactate can also be made during seizures, in the setting of shock, and in patients with large wounds or burns."
- Mulholland and Greenfield's Surgery, 7th Ed.
| Tissue | Why it produces lactate |
|---|---|
| Skeletal muscle (exercising) | Oxygen demand exceeds supply → anaerobic glycolysis |
| RBCs (erythrocytes) | Have NO mitochondria - can only do anaerobic glycolysis |
| Skin | Low oxidative capacity |
| Brain (astrocytes) | Produce lactate for neurons |
| Intestinal mucosa | High turnover, partly anaerobic |
Organs That Clear Lactate
"The liver is exceptionally efficient at converting lactate to pyruvate through the Cori cycle. The kidneys also play a key role in lactate clearance with up to 20-30% of serum loads being metabolized and/or actively excreted."
- Mulholland and Greenfield's Surgery, 7th Ed.
- Liver - primary (gluconeogenesis)
- Kidneys - 20-30% of lactate cleared here
- Heart - oxidizes lactate directly in TCA cycle (excellent fuel for cardiac muscle)
- Resting skeletal muscle - can oxidize lactate from exercising muscles
Clinical Significance
| Condition | Relevance to Cori Cycle |
|---|---|
| Lactic acidosis | Cori cycle overwhelmed (severe exercise, shock, sepsis, liver failure) → lactate accumulates |
| Liver failure (cirrhosis) | Liver cannot run gluconeogenesis efficiently → lactate clearance reduced |
| Metformin toxicity | Metformin inhibits hepatic gluconeogenesis → lactic acidosis |
| Renal failure | Reduces 20-30% of lactate clearance → elevated serum lactate |
| Warburg effect (cancer) | Cancer cells preferentially use anaerobic glycolysis → excessive lactate production (similar to Cori cycle) |
"Even patients with cirrhosis do not exhibit elevated lactate levels at baseline, although the rate at which a lactate load is cleared does correlate with liver function."
- Mulholland and Greenfield's Surgery, 7th Ed.
Summary in One Paragraph
- Basic Medical Biochemistry: A Clinical Approach, 6th Ed. - Fate of Lactate, Cori Cycle (Fig. 22.12)
- Lippincott's Illustrated Reviews: Biochemistry, 8th Ed. - Gluconeogenesis, Cori Cycle (Fig. 10.2)
- Mulholland and Greenfield's Surgery, 7th Ed. - The Cori Cycle (clinical context)
- Yamada's Textbook of Gastroenterology, 7th Ed. - Glucose production, Cori cycle
what is glycolysis and gluconeogenesis
Tell me about osteosarcoma
now again i have another session of pbl today and remember the rule each information you provide must be from a medical book either gold standard or indian writer book prefer mbbs books
now again i have another session of pbl today and remember the rule each information you provide must be from a medical book either gold standard or indian writer book prefer mbbs books
Tell me the Normal range of Hb, RBC, PCV, MCV, MCHC, MCH