Explain me mi diagnosis with ecg and which ither condition should I ruke out at the same time with images
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have rich content and images. Let me compile the comprehensive answer.
ST-Elevation Myocardial Infarction (STEMI): ECG Explained + Conditions to Rule Out
What is STEMI?
STEMI occurs when a coronary artery is completely blocked - usually by a ruptured atherosclerotic plaque that triggers rapid thrombus formation. This cuts off blood supply to a full thickness ("transmural") region of myocardium, causing irreversible necrosis if not treated urgently. The key window for treatment is <90 minutes door-to-balloon with primary PCI.
ECG Hallmarks of STEMI
The 12-lead ECG is the central triage tool. The sequence of changes progresses over hours:
| Time | ECG Change |
|---|---|
| Minutes (hyperacute) | Tall, peaked "hyperacute" T waves |
| Hours | ST-segment elevation (convex/tombstone shape) in the infarct territory |
| Hours | Reciprocal ST depression in opposite leads |
| Hours-Days | Q waves develop (permanent necrosis) |
| Days-Weeks | T-wave inversion |
Diagnostic criteria: ST elevation ≥1 mm in ≥2 contiguous limb leads, OR ≥2 mm in ≥2 contiguous precordial leads (≥2.5 mm in men <40y / ≥1.5 mm in women in V2-V3).
STEMI Localization by Territory
| Leads with ST Elevation | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCx or LAD diagonal |
| V1-V6 + I, aVL | Anterolateral | Proximal LAD |
| II, III, aVF | Inferior | RCA (90%) or LCx |
| Tall R + ST depression in V1-V3 | Posterior | RCA or LCx |
| ST elevation in RV leads (RV3-RV6) | Right ventricular | Proximal RCA |
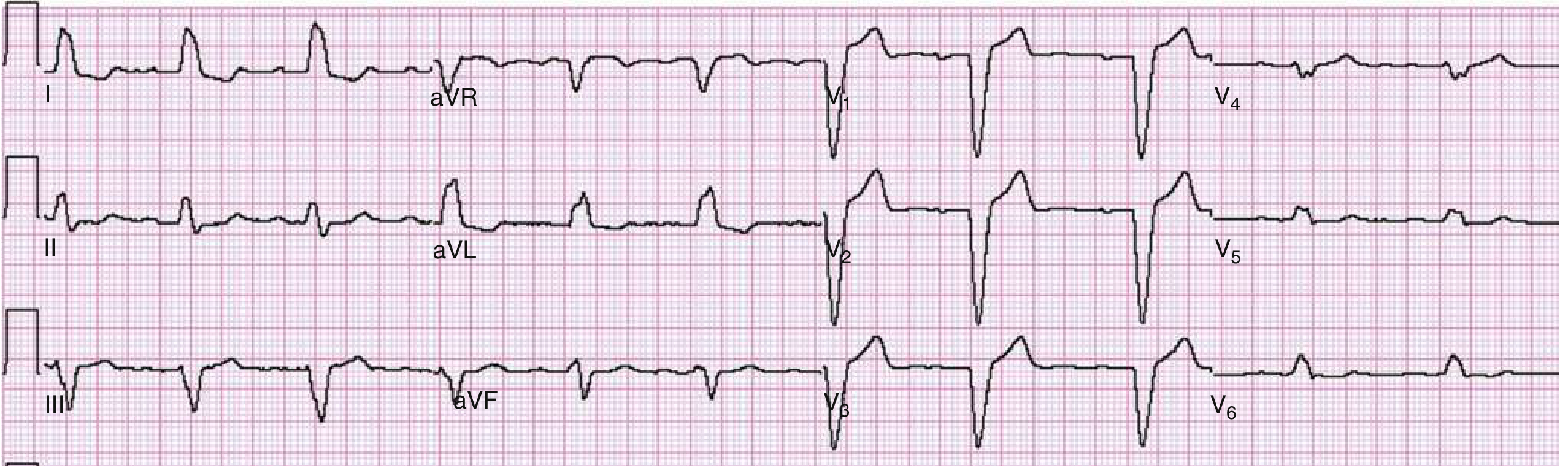
ECG Example: Anterolateral STEMI
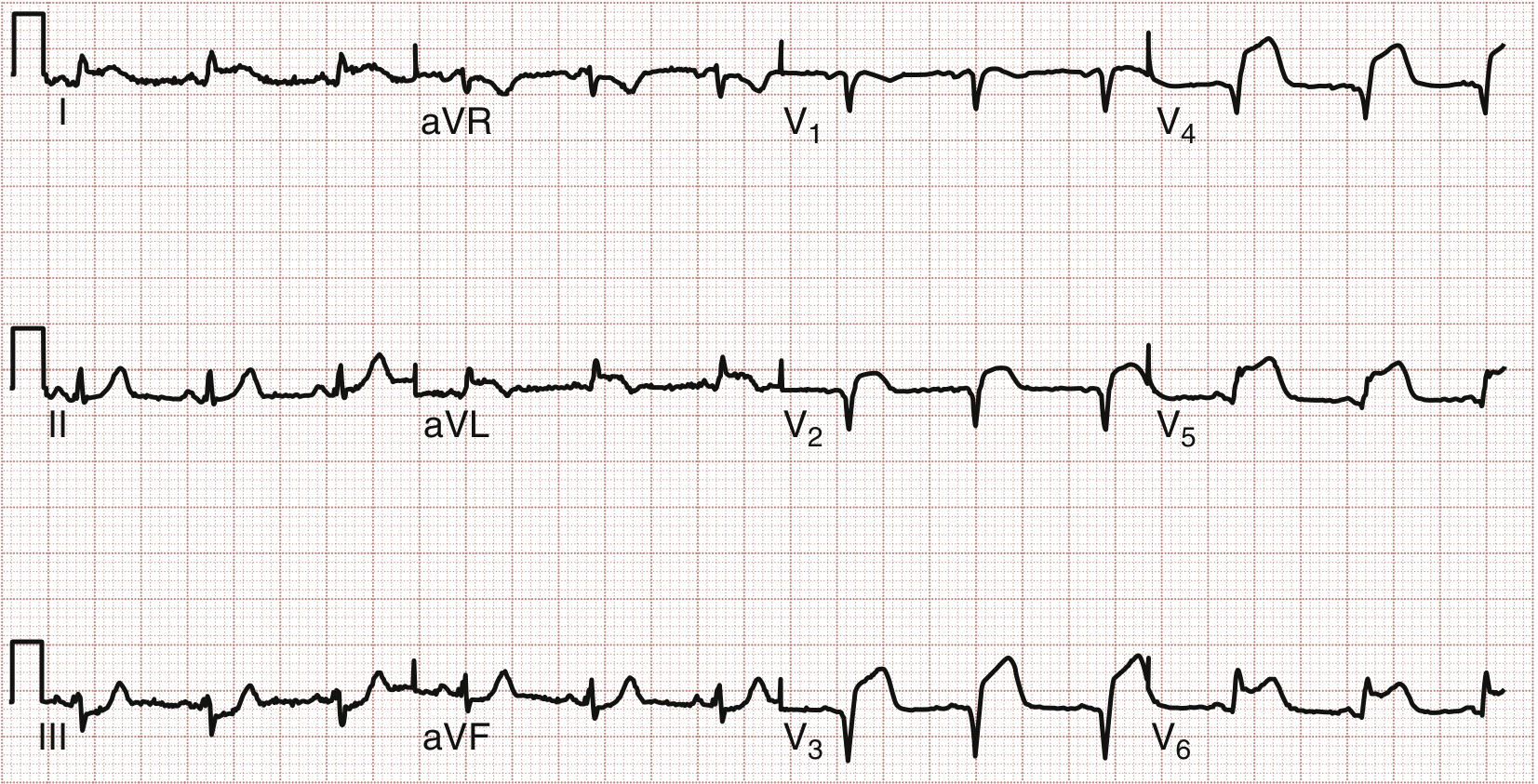
Anterolateral STEMI: ST elevation in leads V1-V4 (anterior) and I, aVL, V5-V6 (lateral). Proximal LAD occlusion confirmed at PCI. - Rosen's Emergency Medicine, 10e
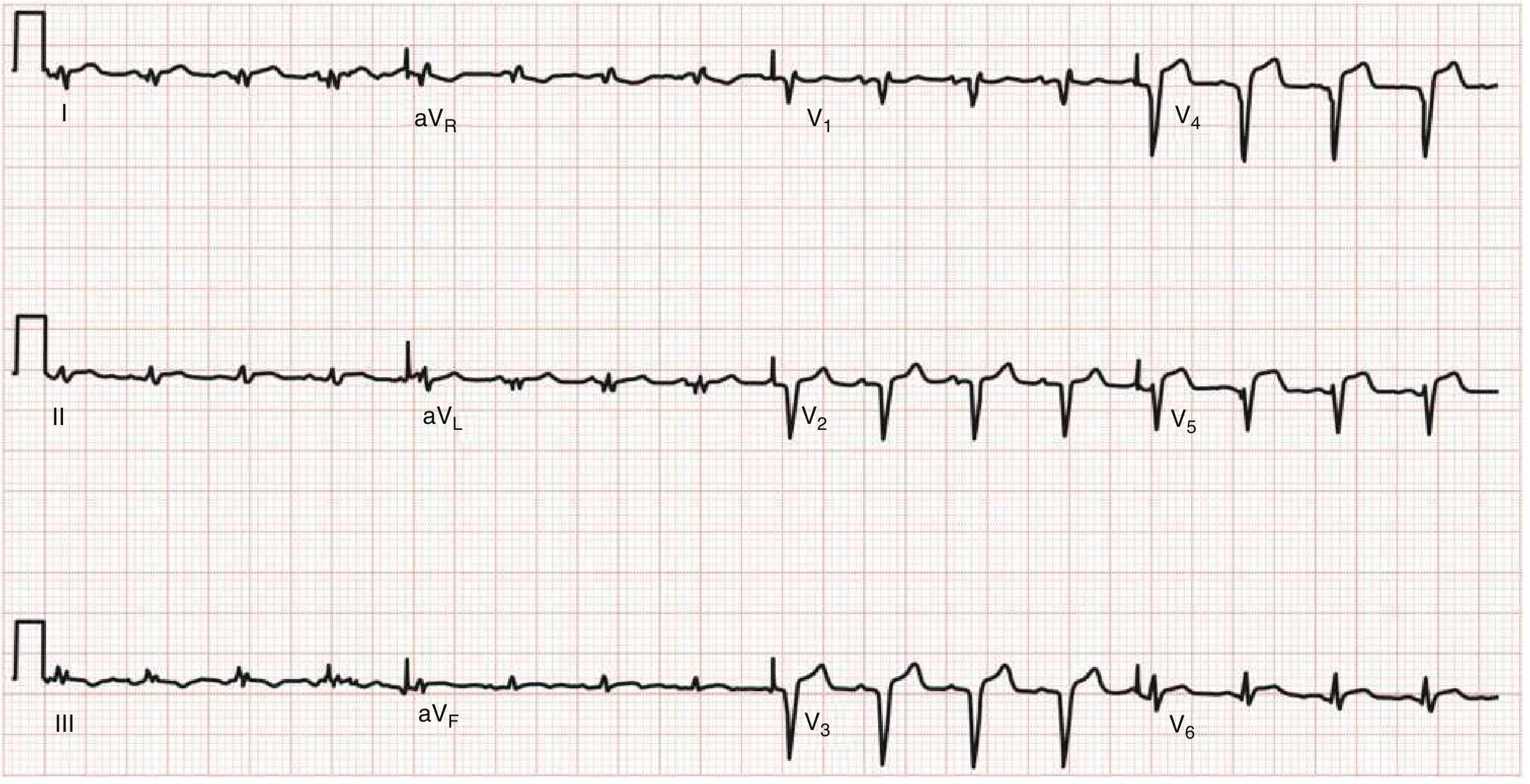
ECG Example: High Lateral STEMI
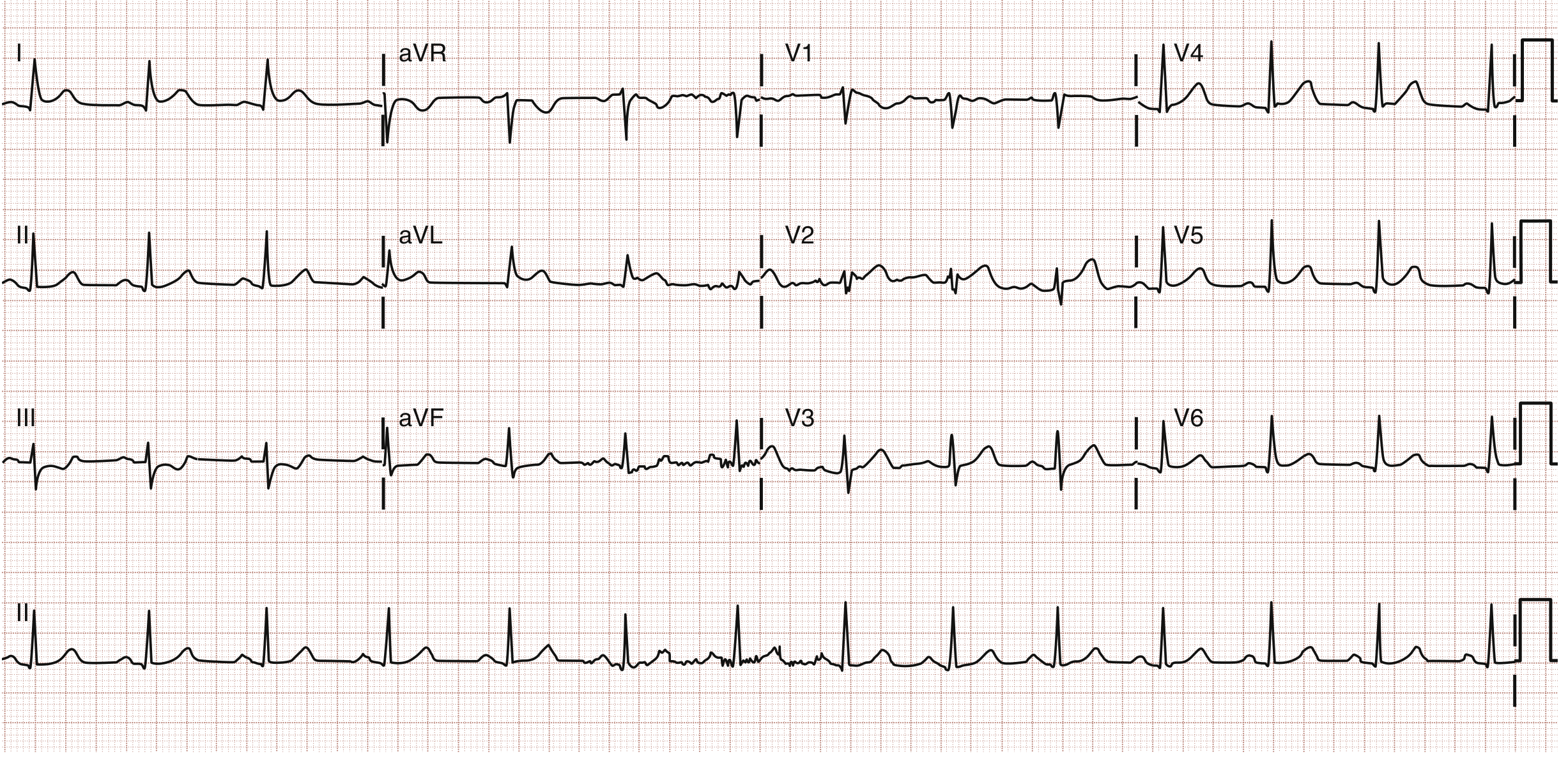
High lateral STEMI: ST elevation in I and aVL, reciprocal ST depression in III, aVF, and V1. LAD/D1 bifurcation lesion treated with PCI. - Rosen's Emergency Medicine, 10e
ECG: Right Ventricular Infarction (RV leads)
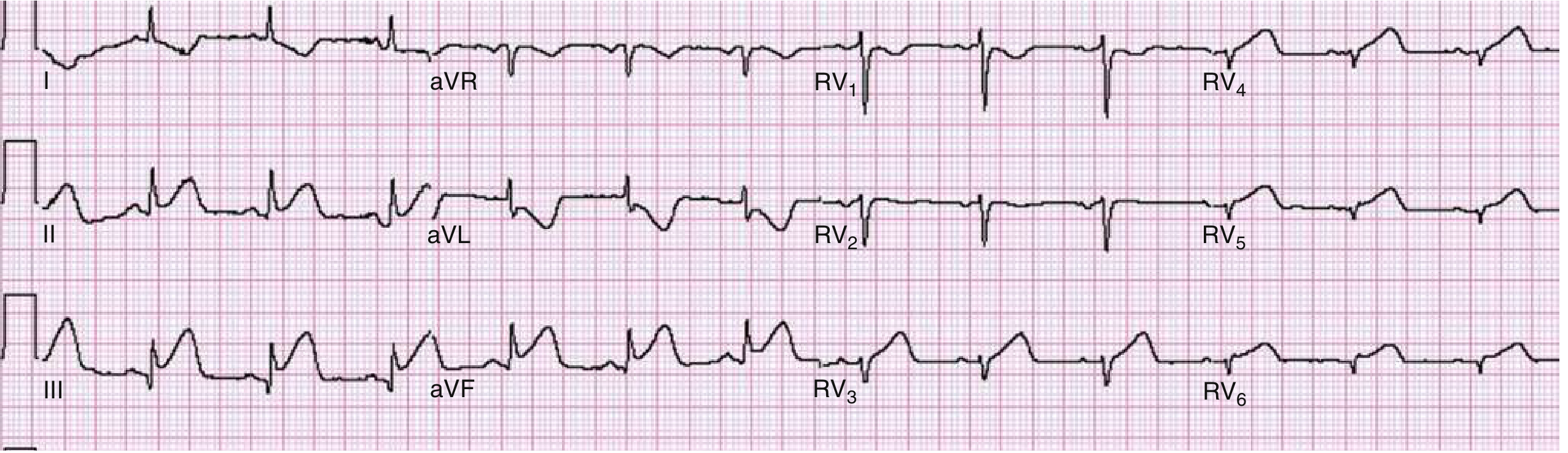
Right ventricular infarction: ST elevation in right-sided leads RV3-RV6. Always order right-sided leads in inferior STEMI to look for this - it changes management (avoid nitrates/diuretics). - Rosen's Emergency Medicine, 10e
Conditions to Rule Out (STEMI Mimics)
ST-segment elevation on ECG does not always mean STEMI. The following conditions must be considered and excluded, because giving thrombolytics or rushing to the cath lab for these can cause serious harm.
1. Pericarditis / Myopericarditis
The most important and common mimic. Caused by viral infections, autoimmune disease, or post-cardiac surgery.
Key ECG differences from STEMI:
- ST elevation is diffuse (almost all leads) vs. regional in STEMI
- ST morphology is concave upward ("saddle-shaped") vs. convex/tombstone in STEMI
- PR segment depression in inferior leads and V6 (very specific for pericarditis)
- PR elevation in aVR (mirror image)
- No reciprocal ST depression (except in aVR)
- No Q waves develop
- Stable over time without the evolving pattern of STEMI
2. Benign Early Repolarization (BER)
A normal ECG variant - one of the most common causes of ST elevation in young, healthy adults presenting with chest pain.
Key ECG features:
- ST elevation in V2-V5 (rarely in limb leads)
- ST morphology is concave upward (not convex)
- J-point notching - a small notch at the junction of QRS and ST
- Large, symmetric T waves
- Stable over time (does NOT evolve like STEMI)
- J-point elevation usually <3.5 mm
Warning: Isolated BER in limb leads is rare and should prompt reconsideration of STEMI.
3. Left Bundle Branch Block (LBBB)
LBBB causes ST changes that look like STEMI because of abnormal ventricular depolarization.
Normal LBBB ST features (not AMI):
- QRS width >0.12 sec
- No Q wave in lead V6
- Broad monophasic R in V5, V6, I, aVL
- Discordant ST changes - ST goes opposite to the QRS (normal in LBBB)
Diagnosing AMI within LBBB - Sgarbossa Criteria:
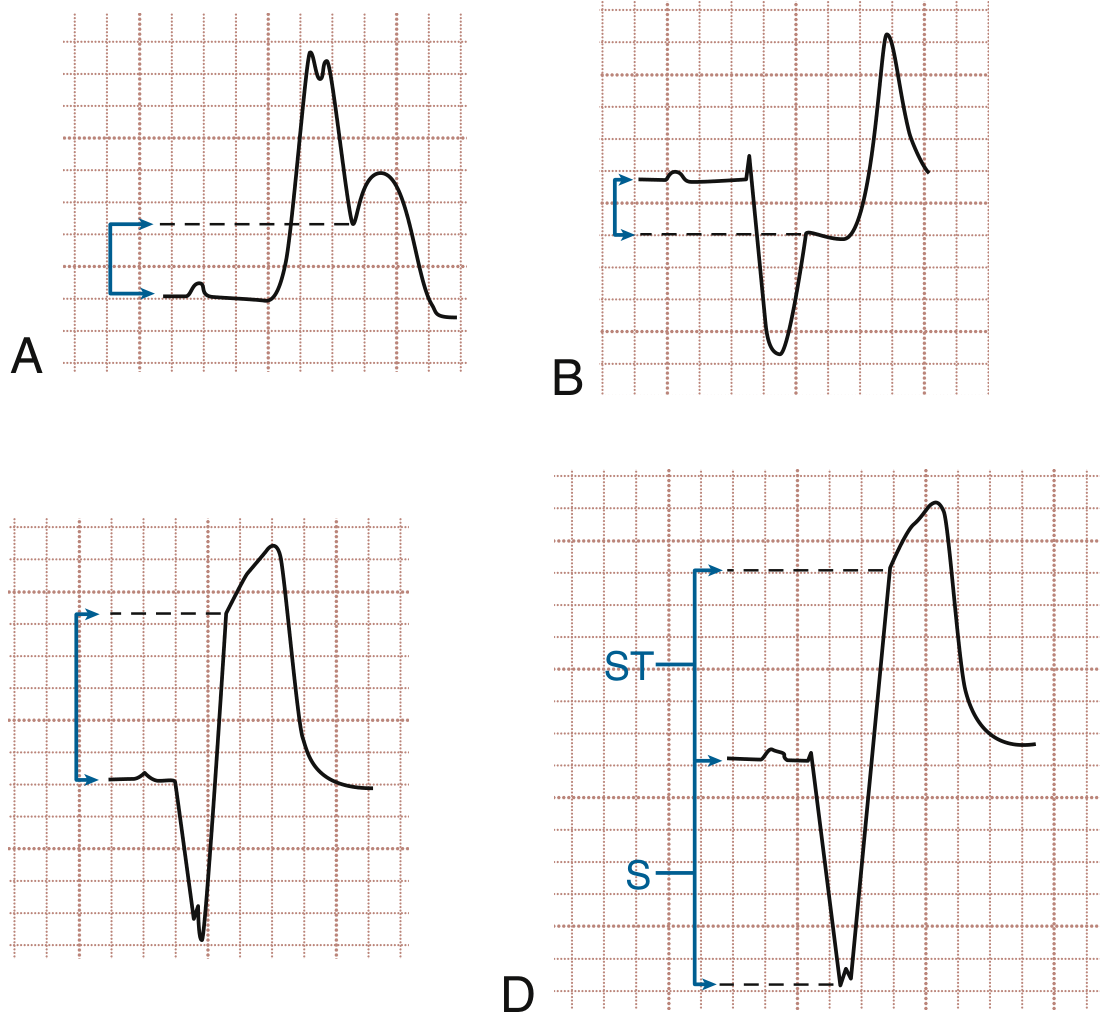
Sgarbossa criteria: (A) Concordant ST elevation ≥1 mm, (B) ST depression ≥1 mm in V1-V3, (C) Discordant ST elevation ≥5 mm, (D) Modified criteria: ST/S ratio >0.25. - Rosen's Emergency Medicine, 10e
| Sgarbossa Criterion | Points |
|---|---|
| Concordant ST elevation ≥1 mm | 5 |
| ST depression ≥1 mm in V1, V2, or V3 | 3 |
| Discordant ST elevation ≥5 mm | 2 |
Score ≥3 = AMI likely. The modified Sgarbossa criterion (ST/S ratio >0.25) has higher sensitivity.
LBBB without AMI: discordant ST elevation in V1-V3 is expected and does NOT indicate infarction - Rosen's Emergency Medicine, 10e
4. Left Ventricular Aneurysm (LVA)
A complication of prior MI where a segment of the LV wall bulges outward permanently.
ECG features:
- Persistent ST elevation in anterior leads (V1-V4) - does not resolve after acute MI
- Well-formed Q waves (indicating old infarction) - the key distinguishing feature vs. acute STEMI
- No reciprocal changes in contiguous leads
- Changes are regional, not diffuse
Left ventricular aneurysm: Well-formed Q waves in V2-V5 with persistent ST elevation. No reciprocal changes. Compare with prior ECGs to distinguish from new STEMI. - Rosen's Emergency Medicine, 10e
5. Left Ventricular Hypertrophy (LVH)
LVH can produce ST elevation that mimics STEMI.
How to differentiate:
- Prominent negative QRS complexes in V1-V2 (large rS or QS pattern)
- Discordant ST elevation with concave initial portion (vs. straight/convex in STEMI)
- Tall R waves in V5-V6 (voltage criteria)
- ST changes usually extend beyond V1-V2 only in LVH
6. Ventricular Paced Rhythm (VPR)
Pacemakers generate a pseudo-LBBB pattern that mimics STEMI.
Key clue: Look for pacemaker spikes before QRS complexes. The same Sgarbossa criteria apply to VPR as to LBBB.
Quick Summary Table
| Condition | ST Shape | Distribution | PR Changes | Q Waves | Reciprocal Changes |
|---|---|---|---|---|---|
| STEMI | Convex/tombstone | Regional (territory) | Normal | Develop over hours | Yes |
| Pericarditis | Concave (saddle) | Diffuse (all leads) | PR depression | No | No (except aVR) |
| BER | Concave + J notch | V2-V5 | Normal | No | No |
| LBBB | Discordant | Right precordial | Normal | Absent in V6 | Discordant only |
| LV Aneurysm | Persistent STE | Anterior | Normal | Present (old) | None |
| LVH | Concave | V1-V2 | Normal | No | Discordant |
| VPR | Discordant | Variable | Pacemaker spike | Variable | Discordant |
The Bottom Line for Clinical Practice
In any patient with chest pain and ST elevation, the emergency approach is:
- STEMI until proven otherwise - treat urgently
- Check for pericarditis clues (diffuse elevation, PR depression, saddle shape)
- If LBBB or paced rhythm - apply Sgarbossa criteria
- Compare with prior ECGs (LV aneurysm stays persistent; STEMI evolves)
- Use serial ECGs, troponins, and echo to resolve uncertainty
Disclaimer: This is educational information from peer-reviewed medical textbooks (Rosen's Emergency Medicine 10e, Harrison's 22e, Textbook of Family Medicine 9e). Always consult your treating physician for clinical decisions about your specific case.
This is a shared conversation. Sign in to Orris to start your own chat.