Hepatitis B
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hepatitis B"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to write a detailed, well-structured answer on Hepatitis B.
Hepatitis B
The Virus
HBV belongs to the family Hepadnaviridae. The infectious particle is the Dane particle - a 42-47 nm enveloped virion containing a partially double-stranded circular DNA genome of ~3,000 nucleotides (the smallest known human virus genome) and the HBV polymerase. The genome has four overlapping open reading frames:
| Gene | Product | Function |
|---|---|---|
| Pre-S/S | Surface proteins (small, middle, large) | Express HBsAg; coat the virion |
| Pre-C/C | Core protein (HBcAg) + HBeAg | Structural capsid; HBeAg promotes immune tolerance |
| P gene | HBV polymerase (reverse transcriptase + RNAse H) | Viral replication |
| X gene | X protein (transactivator) | HBV replication; bears oncogenic properties |
The HBV receptor on hepatocytes is the sodium taurocholate cotransporting polypeptide (NTCP). After attachment, the virus enters, releases its nucleocapsid into the nucleus, and converts its relaxed circular DNA (rcDNA) into covalently closed circular DNA (cccDNA) - the transcriptional template that persists in the nucleus and is the main barrier to cure.
- Goldman-Cecil Medicine, p. 1568
Epidemiology and Transmission
Two billion people worldwide have been exposed to HBV, with approximately 300 million chronically infected. The four main transmission routes are:
- Sexual transmission - predominant in industrialized countries
- Perinatal (mother-to-infant) - principal route in Asia; carries >90% risk of chronic infection
- Horizontal (non-sexual contact) - common in young children in Africa; ~15% progress to chronicity
- Percutaneous - IV drug use, contaminated medical equipment, blood products (pre-1987)
High-risk groups include: healthcare workers, dialysis patients, household/sexual contacts of HBsAg+ individuals, MSM, injection drug users, inmates, and persons born in endemic regions.
- Goldman-Cecil Medicine, p. 1568
Pathogenesis
HBV is not directly cytopathic to hepatocytes. Liver injury is immunologically mediated:
-
CD8+ cytolytic T cells recognize HBcAg and HBeAg on hepatocyte surfaces (alongside HLA molecules) and destroy infected hepatocytes. A robust, broad, polyclonal CD8+ response drives both viral clearance and liver damage.
-
Innate immune response (NK cells, inflammatory cytokines) eliminates >90% of HBV DNA before peak T-cell infiltration - largely through non-cytopathic clearance of replicative intermediates from the cytoplasm and cccDNA from the nucleus.
-
Immune tolerance explains the chronic carrier state: patients with defective cellular immunity are far more likely to remain chronically infected, reinforcing that the immune response - not the virus itself - drives injury.
-
In chronic infection, T-cell exhaustion and depletion allow viral persistence.
-
Harrison's Principles of Internal Medicine 22E, p. 2691-2692
Serological Markers and Their Interpretation
The kinetics of markers during acute self-resolving infection are illustrated below:
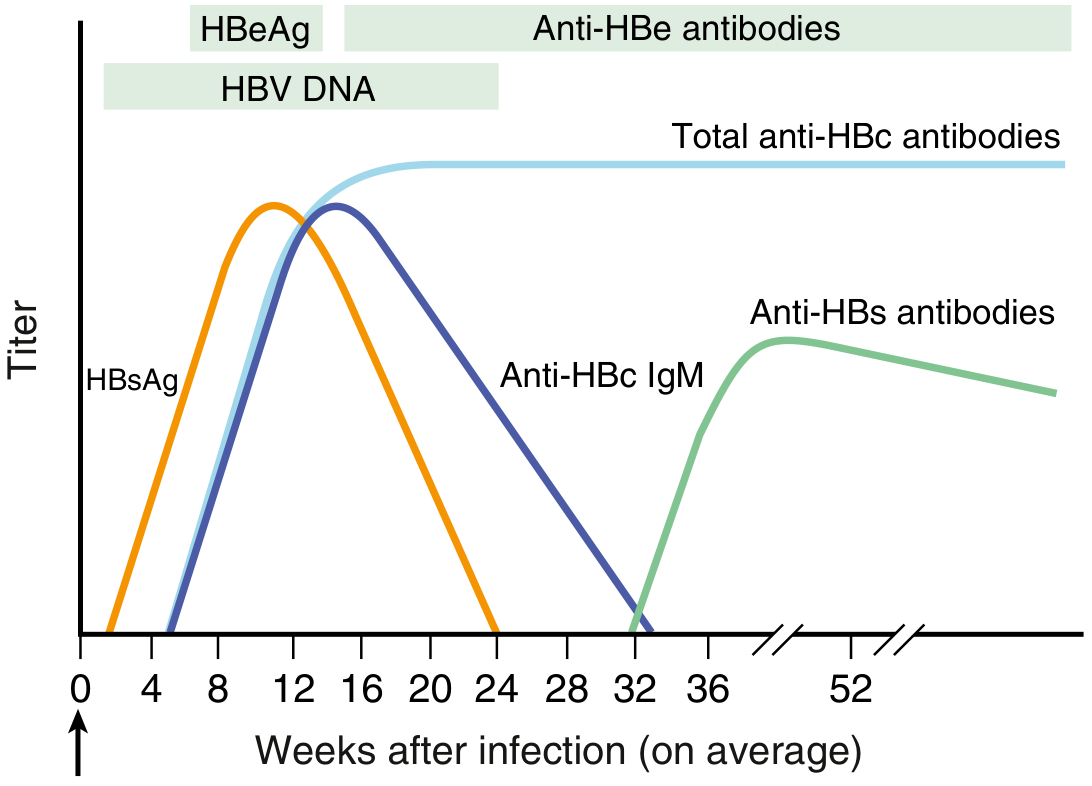
| Marker | Meaning |
|---|---|
| HBsAg | Active infection (acute or chronic); detectable 2-6 weeks before symptoms |
| HBeAg | Active viral replication; high infectivity |
| Anti-HBe | Seroconversion from HBeAg; signals start of resolution |
| IgM anti-HBc | Acute infection / recent exposure; high titer = acute disease |
| IgG anti-HBc | Past exposure (persists for life) |
| Anti-HBs | Immunity (post-infection recovery or vaccination) |
| HBV DNA (PCR) | Most sensitive marker of viral replication; used for treatment monitoring |
Phases of acute infection:
- Incubation: HBsAg+, anti-HBc IgM +/-
- Acute hepatitis: HBsAg+, anti-HBc IgM+
- Convalescence: HBsAg resolves, IgM anti-HBc+, anti-HBs not yet detectable ("window period")
- Recovery: anti-HBc IgG+ and anti-HBs+
Chronic infection is defined as HBsAg persisting >6 months. Blood from infected individuals can contain up to 10^10 viral particles/mL.
Pre-core mutant (HBeAg-negative chronic hepatitis): A stop codon mutation at nucleotide 1896 abolishes HBeAg production but allows continued viral replication - associated with more aggressive chronic disease.
- Jawetz Medical Microbiology 28E, p. 2374-2377; Goldman-Cecil Medicine, p. 1552
Clinical Phases of Chronic HBV Infection
| Phase | HBeAg | Anti-HBe | HBV DNA | ALT | Liver Histology |
|---|---|---|---|---|---|
| Immune tolerant | + | - | Very high | Normal | Minimal inflammation |
| Immune active (HBeAg+) | + | - | High | Elevated | Active hepatitis |
| Inactive carrier | - | + | Low/undetectable | Normal | Mild/absent |
| HBeAg-negative active hepatitis | - | + | Moderate-high | Elevated | Active hepatitis |
| HBsAg-negative (occult) | - | - | Low/undetectable | Normal | Variable |
Complications
- Cirrhosis - from repeated cycles of necroinflammation
- Hepatocellular carcinoma (HCC) - HBV is a major risk factor; the X protein has direct oncogenic properties; HCC can occur even without cirrhosis. A 2025 umbrella review (PMID 39834076) confirmed HBV as among the strongest independent risk factors for HCC.
- Fulminant hepatitis - rare in acute HBV (~1%), but life-threatening
- Extrahepatic manifestations: membranous nephropathy, polyarteritis nodosa, mixed cryoglobulinemia, serum sickness-like prodrome (urticaria, arthralgias)
Treatment
Acute HBV
Most previously healthy adults (~99%) recover spontaneously. Antiviral therapy is not routinely required. However, it is recommended in severe acute HBV - defined by coagulopathy, persistent symptoms, or marked jaundice >4 weeks - to prevent progression to acute liver failure:
-
Entecavir 0.5 mg/day or Tenofovir (TDF 245 mg/day or TAF 25 mg/day) until severity resolves
-
Treatment does not increase risk of chronicity.
-
Goldman-Cecil Medicine, p. 1544
Chronic HBV - Approved Agents
Nucleos(t)ide analogues (NAs):
| Drug | Notes |
|---|---|
| Tenofovir alafenamide (TAF) | Preferred; better renal/bone safety than TDF |
| Tenofovir disoproxil fumarate (TDF) | Highly effective; also active in lamivudine-resistant HBV |
| Entecavir | Highly effective, high barrier to resistance; preferred first-line |
| Lamivudine | Older; high resistance rates with long-term use |
| Adefovir | Superseded by tenofovir |
| Telbivudine | Rarely used |
Tenofovir is more effective than adefovir or entecavir for histologic improvement and viral suppression in both HBeAg-positive and HBeAg-negative chronic HBV. Entecavir is more efficacious than lamivudine or telbivudine.
Immune modulators:
-
Pegylated interferon-alfa-2a (48 weeks): finite treatment; can achieve HBsAg loss in select patients; not suitable for cirrhotics
-
Standard interferon-alfa-2b (less commonly used)
-
Goldman-Cecil Medicine, p. 1783-1795; Harrison's Principles of Internal Medicine 22E
Prevention and Vaccination
- Recombinant HBsAg vaccine: 3-dose series; universal infant vaccination is practiced in most countries.
- High-risk individuals (HCWs, dialysis patients, contacts of carriers, MSM, pregnant women) should be screened and seronegative persons vaccinated.
- Post-exposure prophylaxis: Hepatitis B immune globulin (HBIG) + vaccine for unvaccinated exposures (e.g., newborns of HBsAg+ mothers).
- Barrier protection, not sharing personal items (razors, toothbrushes), and not donating blood/organs if infected.
Recent Evidence (2024-2026)
- A 2025 systematic review and meta-analysis (PMID 39983746) in Lancet Gastroenterol Hepatol evaluated non-invasive tests for staging liver fibrosis/cirrhosis in chronic HBV, informing WHO 2024 guidelines - supporting use of elastography and other non-invasive tools to reduce reliance on liver biopsy.
- A 2025 AGA Clinical Practice Guideline (PMID 39863345) in Gastroenterology addressed prevention and treatment of HBV reactivation in at-risk individuals (e.g., those on immunosuppressive therapy), recommending prophylactic antivirals for HBsAg+ or anti-HBc+ patients receiving biologic therapy.
Sources: Jawetz Melnick & Adelberg's Medical Microbiology 28E | Goldman-Cecil Medicine | Harrison's Principles of Internal Medicine 22E (2025) | Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.