Explain me about dermatomes
Reading File
Finding Sources
Searching the Web
dermatomes spinal nerve roots anatomy clinical significance diagram
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Now I have rich material from multiple authoritative textbooks. Let me compile the full answer.
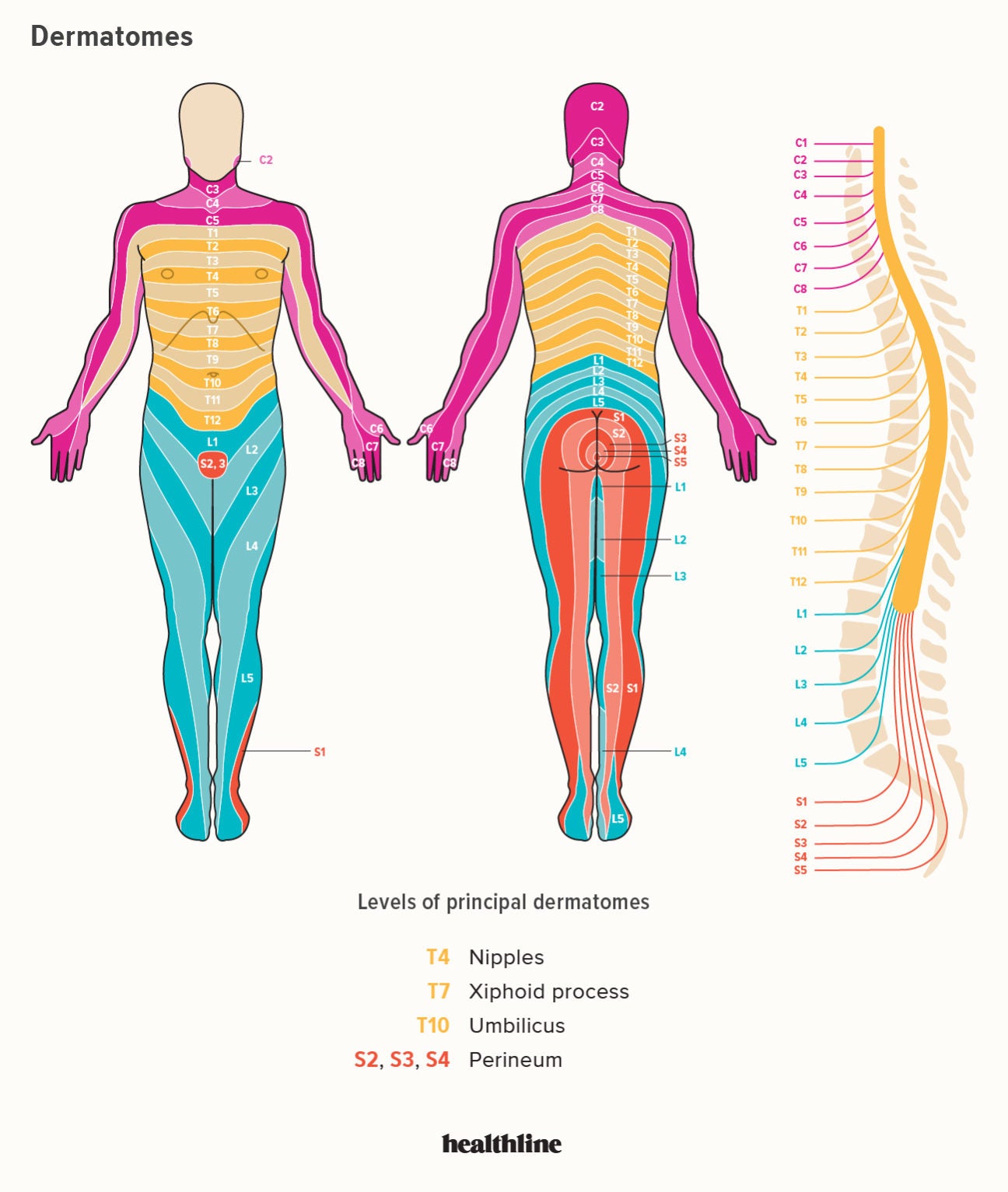
Dermatomes
A dermatome is the area of skin innervated by the sensory fibers of a single posterior (dorsal) spinal nerve root. The word comes from the Greek derma (skin) + tome (segment). There are 30 functional dermatomes - corresponding to 31 spinal nerve pairs minus C1, which is purely motor and has no sensory field.
Anatomy and Organization
Each spinal cord segment gives rise to a pair of spinal nerves (one left, one right). These form from the union of:
- A dorsal (posterior) root - carries sensory (afferent) fibers from the dermatome
- A ventral (anterior) root - carries motor (efferent) fibers to the corresponding myotome
Sensory fibers pass from the skin through the intervertebral foramen, where they join motor fibers to form the mixed spinal nerve, which then divides into anterior and posterior rami.
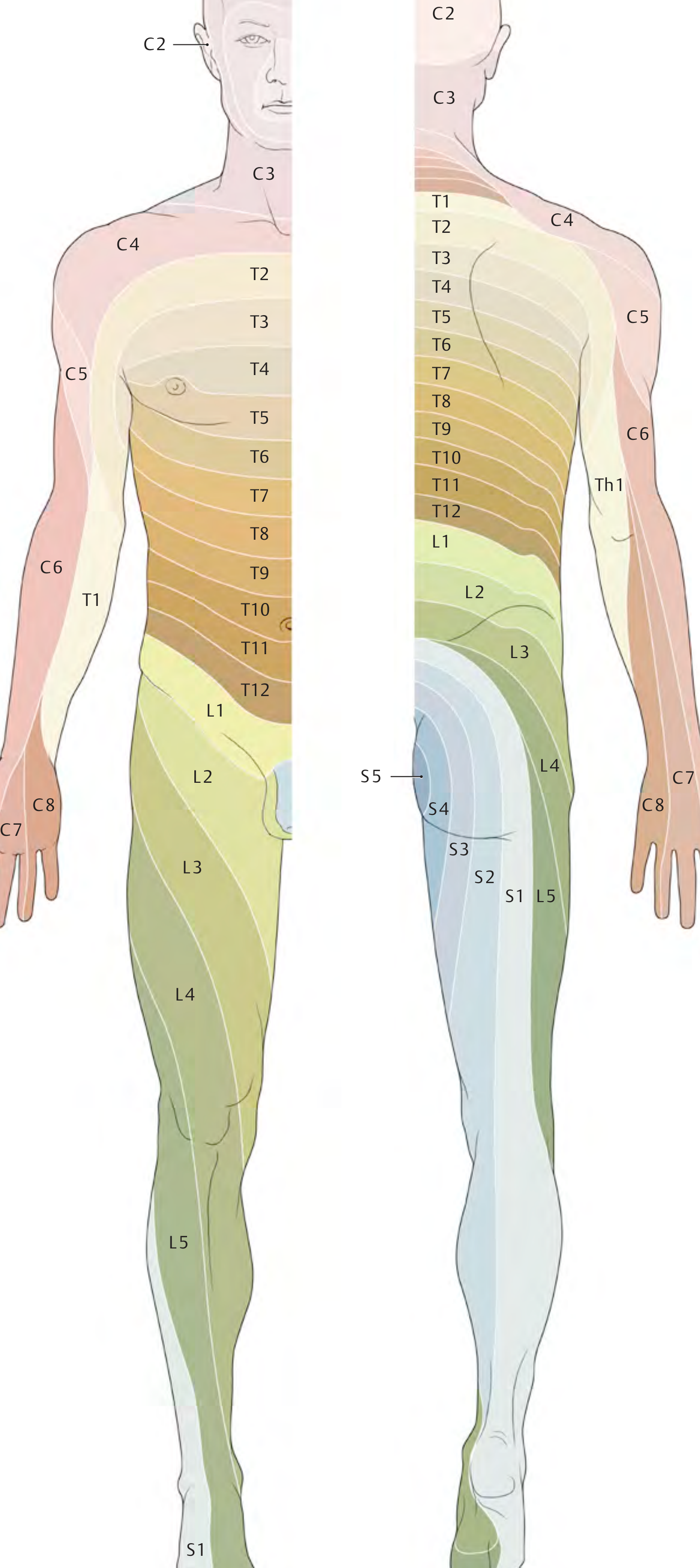
The full dermatome map from the THIEME Atlas:
Regional Breakdown
Cervical (C2-C8)
| Level | Region Supplied |
|---|---|
| C2 | Posterior scalp, occiput |
| C3 | Posterior neck, lower occiput |
| C4 | Shoulder top, upper chest |
| C5 | Lateral arm, deltoid patch |
| C6 | Lateral forearm, thumb and index finger |
| C7 | Middle finger, central hand (posterior) |
| C8 | Ring and little finger, medial hand |
(Note: C1 has no dermatome - it consists entirely of motor fibers.)
Thoracic (T1-T12)
The thoracic dermatomes form even, stacked horizontal bands across the trunk. Key landmarks:
- T4 - Nipple line
- T7 - Xiphoid process
- T10 - Umbilicus
- T12 - Inguinal region
These are the most orderly dermatomes because limb bud formation has not mixed them with adjacent segments.
Lumbar (L1-L5)
| Level | Region Supplied |
|---|---|
| L1 | Inguinal ligament, upper groin |
| L2 | Upper/anterior thigh |
| L3 | Medial thigh, anterior knee |
| L4 | Anterior thigh, anterior knee, pretibial shin |
| L5 | Lateral thigh, anterolateral calf, dorsum of foot, great toe |
Sacral (S1-S5)
| Level | Region Supplied |
|---|---|
| S1 | Posterior thigh, posterior calf, lateral foot, little toe |
| S2-S4 | Perineum, perianal area (saddle region) |
| S5 | Perianal skin |
Embryological Origin
Dermatomes arise from somites - segmented blocks of paraxial mesoderm that form alongside the neural tube during early embryonic development. Each somite differentiates into:
- Sclerotome - forms vertebrae and ribs
- Myotome - forms skeletal muscle
- Dermatome - forms the dermis
A key rule: Each myotome and dermatome retains its segmental innervation from its site of origin, regardless of where the cells migrate. This is why the dermatome map of the limbs appears twisted - as limb buds grow and rotate, the dermal primordia drag their nerve supply with them.
Dermatome Overlap
Adjacent dermatomes broadly overlap. This has a critical clinical consequence:
-
A single nerve root lesion often produces a smaller sensory deficit than the anatomical dermatome
-
The "autonomous zone" is the small central area of each dermatome that receives supply from only that root, with no overlap from neighbors
-
This is why testing the autonomous zone gives the most reliable result in clinical examination
-
General Anatomy and Musculoskeletal System (THIEME Atlas), p. 105
Dermatomes vs. Peripheral Nerve Territories
This distinction is fundamental to neurological examination:
| Feature | Dermatomal (radicular) | Peripheral nerve |
|---|---|---|
| Cause | Nerve root compression (e.g., disc herniation) | Peripheral nerve injury |
| Pattern | Follows a spinal level; often striped/band | Follows anatomical nerve distribution |
| Example | L5 radiculopathy - pain down lateral leg to great toe | Common peroneal nerve injury - loss over dorsum of foot |
| Associated findings | Reflex changes at that level | No reflex change unless a mixed nerve |
Clinical Applications
1. Localizing spinal cord and nerve root lesions
When a herniated intervertebral disc compresses a nerve root, the patient develops pain and sensory loss in the corresponding dermatome. This allows the clinician to identify the spinal level:
- C4-C6 lesion: radicular pain along radial forearm, thumb - weakness of elbow flexion, depressed biceps reflex
- C7-T1 lesion: pain over ulnar forearm and hand - elbow extension weakness, depressed triceps reflex
2. Assessing spinal cord injury
After trauma, sensory testing of all dermatomes maps the "most caudal dermatome with normal sensation," defining the neurological level of injury. Key landmarks used at the bedside: T4 (nipple line), T10 (umbilicus).
3. Herpes Zoster (Shingles)
The varicella-zoster virus reactivates within a single dorsal root ganglion and travels anterograde down its axons - producing a painful vesicular rash strictly confined to one dermatome on one side. The most common levels affected are thoracic, but ophthalmic (V1) and facial involvement is also seen. The dermatomal distribution itself is the key diagnostic feature.
- Andrews' Diseases of the Skin, p. 1311: "A unilateral, painful eruption of grouped vesicles along a dermatome, with hyperesthesia and regional lymph node enlargement, is typical."
4. Regional anesthesia
Epidural and spinal anesthesia aim to block specific dermatomal levels. For example, spinal anesthesia for C-section targets T4 (blocking sensation to the nipple line).
5. Radiculopathy (clinical summary)
Radiculopathy = compression or irritation of a nerve root. Symptoms (numbness, tingling, pain) start proximally and radiate distally in a dermatomal distribution. This is distinct from peripheral neuropathy, which follows peripheral nerve territories.
- Frameworks for Internal Medicine, p. 8900: "Clinical manifestations involve the corresponding dermatome and myotome. Sensory symptoms often start in the back or neck and radiate to an extremity in a dermatomal distribution."
Summary Table - Key Dermatomal Landmarks to Memorize
| Landmark | Level |
|---|---|
| Vertex of skull | C2 |
| Shoulder tip | C4 |
| Thumb | C6 |
| Middle finger | C7 |
| Little finger | C8 |
| Nipple | T4 |
| Xiphoid | T7 |
| Umbilicus | T10 |
| Inguinal ligament | L1 |
| Great toe | L5 |
| Lateral foot / heel | S1 |
| Saddle area / perineum | S2-S4 |
Sources: General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy); Bradley and Daroff's Neurology in Clinical Practice; Rheumatology 2-Volume Set (Elsevier); Andrews' Diseases of the Skin; Frameworks for Internal Medicine; TeachMeAnatomy; Medscape
This is a shared conversation. Sign in to Orris to start your own chat.