Management of stroke
Reading File
Finding Sources
Searching PubMed
"ischemic stroke" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive textbook data. Let me compile the full answer.
Management of Stroke
Stroke is a medical emergency requiring immediate classification, stabilization, and targeted intervention. The approach differs substantially between ischemic stroke (~85% of cases) and hemorrhagic stroke (~15%), and within hemorrhagic stroke between intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH).
1. Immediate Assessment (All Stroke Types)
The first priority is rapid diagnosis and initiation of care, ideally in a dedicated stroke unit or ICU.
Airway, Breathing, Circulation:
- Protect the airway - avoid obstruction, hypoventilation, aspiration
- Pulse oximetry or ABGs; supplemental oxygen if SpO2 < 94%
- Avoid hyperthermia (worsens ischemic outcome); treat fever aggressively
- Head of bed > 30 degrees to reduce aspiration risk
- Cardiac monitoring for at least 48 hours (cardiac arrhythmias complicating stroke are common); 12-lead ECG and troponin on admission
Glucose: Persistent hyperglycemia in the first 24 hours worsens outcomes. Target blood glucose 140-180 mg/dL. Treat hypoglycemia (< 60 mg/dL) with IV dextrose.
Key imaging: Non-contrast CT brain immediately to differentiate ischemic from hemorrhagic stroke. MRI (DWI/FLAIR) provides more detailed information when time permits.
"Rapid diagnosis of stroke and initiation of treatment are important to maximize recovery, prevent recurrence of stroke, and prevent complications." - Bradley and Daroff's Neurology in Clinical Practice
2. Ischemic Stroke
2a. Blood Pressure Management
After acute ischemic stroke, BP is often transiently elevated - this is a physiological response to maintain cerebral perfusion in the setting of impaired autoregulation. Optimal BP post-stroke appears to be SBP 160-200 mmHg and DBP 70-110 mmHg acutely (Castillo et al., 2004). Over-treatment causing hypotension is harmful.
When to treat BP before thrombolysis: BP must be < 185/110 mmHg to administer IV alteplase. Agents used:
- Labetalol 10 mg IV over 1-2 min (repeat q10-20 min, max 300 mg)
- Nicardipine infusion 5 mg/h, titrate up to 15 mg/h
- If uncontrolled: sodium nitroprusside
Post-thrombolysis: Monitor BP every 15 min during treatment, then q30 min x6h, then q1h x16h. If SBP 180-230 or DBP 105-120: labetalol 10 mg IV or infusion.
2b. Reperfusion Therapy
IV Thrombolysis (Alteplase / Tenecteplase)
| Parameter | Detail |
|---|---|
| Dose | Alteplase 0.9 mg/kg IV (max 90 mg): 10% as bolus over 1 min, remainder over 60 min |
| Window | Within 3 hours of symptom onset (FDA approved); extended to 4.5 hours in selected patients |
| Approval basis | NINDS trial |
Eligible within 3-4.5 hours (extended window criteria - AHA/ASA):
- Age ≤ 80
- No prior stroke + diabetes combination
- NIHSS ≤ 25
- Not on anticoagulants
- No extensive early ischemic changes on CT
Not recommended for mild non-disabling symptoms (NIHSS 0-5 where deficits do not interfere with ADLs) - the PRISMS trial showed no benefit over aspirin (78% vs 82% favorable outcome at 90 days).
Tenecteplase: A single-bolus IV alternative, with pharmacokinetic advantages, now considered a reasonable alternative to alteplase for eligible patients.
DWI-FLAIR mismatch on MRI can be used to extend thrombolysis to patients with unknown time of onset (woke-up stroke) - if DWI lesion is visible but FLAIR is negative, the infarct is likely < 4.5 hours old.
Mechanical Thrombectomy (Endovascular)
Mechanical thrombectomy with stent retrievers is now the standard of care for large vessel occlusion (LVO), independent of whether the patient receives IV alteplase.
Indications (0-6 hours):
- No significant pre-stroke disability (mRS ≤ 1)
- Occlusion of ICA or MCA M1 segment
- NIHSS ≥ 6
- ASPECTS ≥ 6
Extended window (6-16 hours): DAWN and DEFUSE-3 criteria - perfusion-core mismatch imaging used to select patients with salvageable tissue. DAWN trial showed 49% vs 13% favorable outcome (mRS 0-2 at 90 days).
16-24 hours: DAWN criteria in selected patients.
"Mechanical thrombectomy is now indicated for patients with acute ischemic stroke with large artery occlusion in the anterior circulation who meet selected criteria and who present within 24 hours of last known to be well regardless of whether they receive IV alteplase." - Rosen's Emergency Medicine
Each 1-hour delay to reperfusion is associated with worse functional independence (pooled HERMES data).
2c. Antiplatelet Therapy
- Aspirin 160-325 mg should be given within 24-48 hours of ischemic stroke (not if given alteplase - delay 24 hours)
- IST and CAST trials established modest mortality and recurrence reduction
- Dual antiplatelet therapy (aspirin + clopidogrel) for 21 days is recommended after minor stroke/high-risk TIA (CHANCE trial; POINT trial). Benefit is greatest in the first 3 weeks; extending beyond 90 days increases hemorrhage risk without added benefit.
2d. Prevention of Complications
| Complication | Management |
|---|---|
| DVT/PE | LMWH (enoxaparin 40 mg SC OD) or UFH 5000 U SC BD if no contraindications; IPC if anticoagulation contraindicated (CLOTS-3 trial) |
| Aspiration pneumonia | NPO until formal swallowing assessment; HOB > 30°; enteral feeding tube if dysphagia |
| Urinary complications | Avoid indwelling catheter unless essential; remove early; treat symptomatic UTI |
| Pressure sores | Frequent repositioning, special mattresses, early mobility |
| Falls | Risk assessment at regular intervals |
| Depression | Screen for post-stroke depression (>25% of patients); antidepressants effective |
| Elevated ICP | Mannitol, hypertonic saline, intubation, hemicraniectomy |
3. Intracerebral Hemorrhage (ICH)
30-day mortality approaches 50%.
Blood Pressure
- For SBP 150-220 mmHg: acutely lowering to 140 mmHg is safe and reduces hematoma expansion
- Use IV labetalol, nicardipine, or clevidipine for smooth control
Reversal of Coagulopathy
- Elevated INR (warfarin): reverse with 4-factor PCC (prothrombin complex concentrate) + Vitamin K
- Heparin: protamine sulfate
- DOACs: specific reversal agents (idarucizumab for dabigatran; andexanet alfa for Xa inhibitors)
Elevated ICP
- Intubation + sedation, HOB elevation, hypertonic saline/mannitol
- Ventriculostomy (EVD) for hydrocephalus
- Decompressive hemicraniectomy in refractory cases
Seizures
- Treat clinical seizures with antiepileptics
- Prophylactic AEDs are not routinely recommended
Surgical Evacuation
- Benefit clearest for cerebellar hematoma > 3 cm or with brainstem compression
- Supratentorial hematoma: role of surgery remains debated (STICH trials showed no clear benefit for routine surgery)
4. Subarachnoid Hemorrhage (SAH)
SAH from aneurysm rupture carries high early mortality - the first priority is preventing rebleeding by securing the aneurysm.
Immediate Steps
- Transfer to high-volume center (> 35 SAH cases/year) - associated with lower mortality
- Ventriculostomy (EVD) if hydrocephalus present
- Control BP: target SBP < 160 mmHg pre-aneurysm securing (titratable IV nicardipine preferred)
Aneurysm Obliteration
- Endovascular coiling vs microsurgical clipping - decision by multidisciplinary team based on aneurysm location, patient grade, and institutional expertise
- The ISAT trial showed coiling was associated with better 1-year outcomes for aneurysms amenable to both approaches
- Early treatment (within 24-72 hours) is preferred to reduce rebleeding risk
Rebleeding Prevention (pre-treatment)
- Short-term tranexamic acid or aminocaproic acid (< 72 hours) reduces rebleeding when there is unavoidable delay to aneurysm treatment, but increases thromboembolic risk
Delayed Cerebral Ischemia (Vasospasm)
- Peaks at days 4-14 post-SAH
- Oral nimodipine (60 mg q4h x 21 days) is the standard treatment - reduces vasospasm-related neurological deficit
- Maintain euvolemia; avoid hypovolemia
- Induced hypertension (Triple-H therapy: Hypertension, Hypervolemia, Hemodilution) or endovascular angioplasty/intra-arterial vasodilators for refractory vasospasm
5. Secondary Prevention (Post-Stroke)
| Strategy | Indication / Drug | Evidence |
|---|---|---|
| Antiplatelets | Aspirin 75-325 mg OD; or clopidogrel 75 mg OD; or asp + extended-release dipyridamole | All ischemic stroke/TIA without AF |
| Anticoagulation | Warfarin (INR 2-3) or DOACs | Cardioembolic stroke - especially AF (superior to aspirin) |
| Statins | High-intensity (atorvastatin 80 mg) - target LDL < 70 mg/dL | SPARCL trial: 2% reduction in recurrence over 5 years |
| BP control | RAAS-based (ACE inhibitor or ARB + thiazide) | BP lowering reduces recurrence regardless of baseline |
| PFO closure | Transcatheter closure in selected young patients with cryptogenic stroke | ESO 2024 guidelines (PMID 38752755 - for AF-related) |
| Carotid endarterectomy/stenting | Symptomatic stenosis 50-99%; benefit greatest > 70% stenosis | CEA preferred for surgically accessible stenosis |
6. Rehabilitation
Rehabilitation begins as soon as life-threatening complications are stabilized. Early mobilization, speech therapy, physiotherapy, and occupational therapy are all components. Stroke unit care consistently reduces mortality and disability compared to general ward care.
Summary Diagram
ACUTE STROKE
|
|----> Non-contrast CT brain (immediate)
|
├── ISCHEMIC (~85%)
│ |
│ ├─ Within 4.5h + eligible → IV Alteplase 0.9 mg/kg
│ ├─ LVO detected → Mechanical Thrombectomy (up to 24h)
│ ├─ BP management (permissive unless >185/110 pre-tPA)
│ ├─ Aspirin 24h post-tPA (or immediately if no tPA)
│ └─ Stroke unit care + complication prevention
│
├── ICH (~10-15%)
│ ├─ BP → target SBP 140 mmHg
│ ├─ Reverse anticoagulation
│ ├─ Treat elevated ICP
│ └─ Neurosurgery if cerebellar hematoma > 3 cm
│
└── SAH (~5%)
├─ BP → SBP < 160 mmHg
├─ EVD if hydrocephalus
├─ Secure aneurysm (coiling or clipping)
└─ Nimodipine x 21 days for vasospasm
Sources:
- Bradley and Daroff's Neurology in Clinical Practice (General Management of Acute Ischemic Stroke, p.1405-1408)
- Rosen's Emergency Medicine (Reperfusion Therapy, p.1437-1439)
- Adams and Victor's Principles of Neurology, 12th ed. (Secondary Prevention, p.826)
- Frameworks for Internal Medicine (Intracerebral Hemorrhage, p.577)
- ESO 2024 PFO Guidelines [PMID 38752755]
Search for clinical images of stroke CT/MRI findings
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
All images retrieved. Here is a comprehensive illustrated guide to stroke CT/MRI findings from the medical textbooks.
Stroke - Clinical CT/MRI Imaging Findings
1. Acute Ischemic Stroke - CT (Non-Contrast)
Ultra-Early Signs (within 3-6 hours)
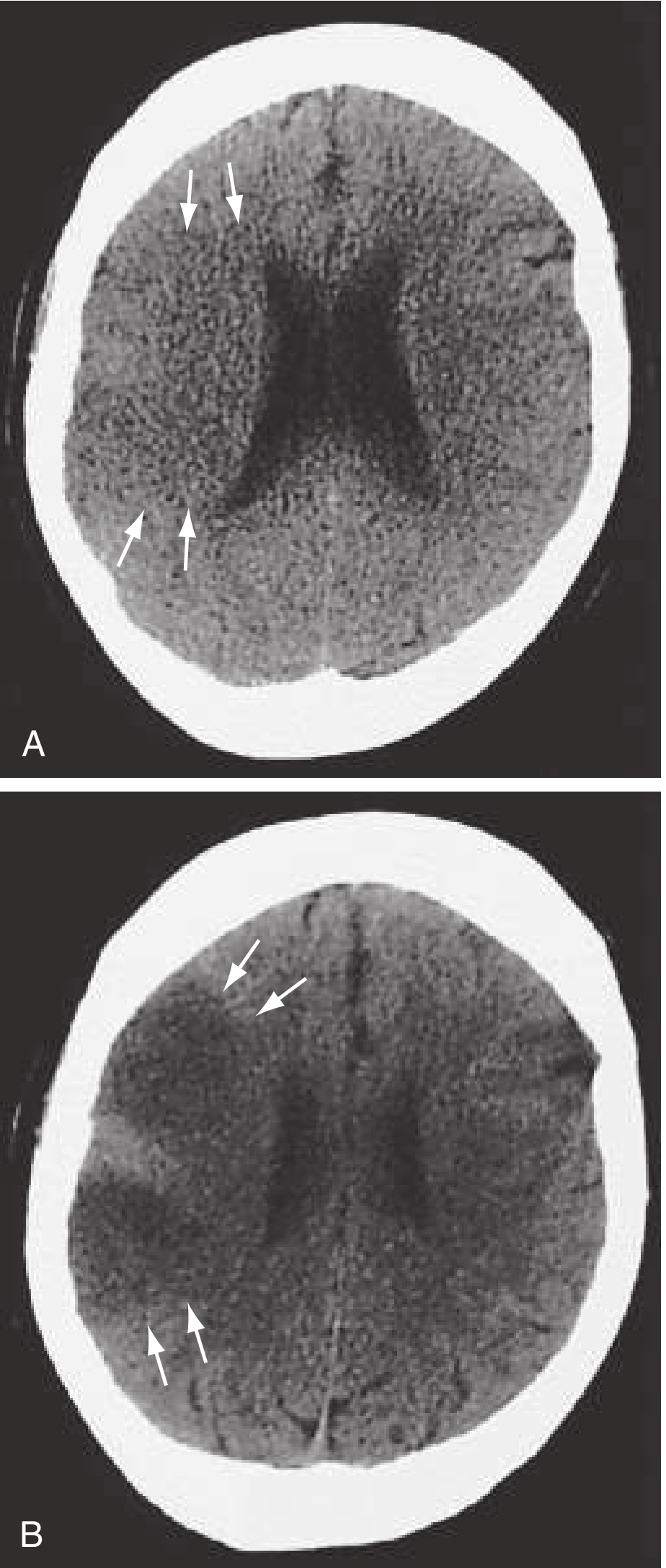
Image A (at 2h 50min): Subtle ultra-early ischemic changes in a large right MCA occlusion - the arrows indicate loss of the gray-white matter interface and early sulcal effacement. These are easy to miss and require careful scrutiny.
Image B (at ~8 hours): The same patient now shows clear acute hypodensity (darker area, arrows) and more prominent sulcal effacement - the classic CT appearance of established ischemic infarction.
Key CT signs of ischemic stroke to recognise:
| Sign | Description | Significance |
|---|---|---|
| Loss of gray-white interface | Insular ribbon sign; basal ganglia obscuration | Ultra-early ischemia (< 6h) |
| Hypodensity | Dark area corresponding to territory | Established infarct |
| Sulcal effacement | Cytotoxic edema compressing sulci | Evolving infarct |
| Hyperdense MCA sign | Dense clot visible in M1 segment | LVO - thrombectomy candidate |
| ASPECTS score | Scoring system for extent of changes | Guides thrombectomy eligibility (≥6 favorable) |
"Patients with a hyperdense artery sign and acute hypodensity of one-third of the MCA distribution tend to have a poorer prognosis. Their outcomes are still better with tPA treatment than without." - Rosen's Emergency Medicine
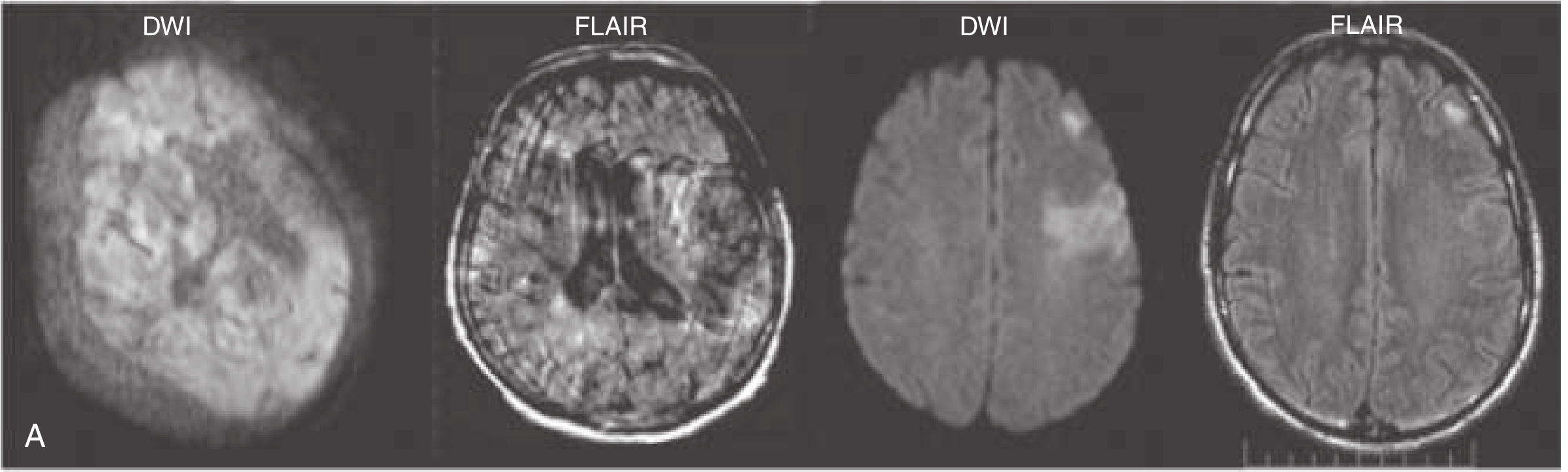
2. MRI - DWI/FLAIR for Ischemic Stroke
DWI-FLAIR Mismatch (Unknown Onset / "Wake-Up Stroke")
Interpretation:
- Left pair (DWI bright, FLAIR dark = mismatch): The DWI shows restricted diffusion (acute infarct) but FLAIR is still negative - this indicates the infarct is likely < 4.5 hours old, making the patient potentially eligible for thrombolysis even with unknown time of onset.
- Right pair (DWI bright, FLAIR also bright = no mismatch): Both sequences positive - the infarct is older (> 4.5h), and thrombolysis carries higher hemorrhagic risk.
This is the basis of the PRE-FLAIR and WAKE-UP trial protocols for extending thrombolysis to patients with unknown onset.
MRI modality summary for stroke:
| Sequence | Finding | Use |
|---|---|---|
| DWI | Bright signal = restricted diffusion | Detects acute ischemia within minutes |
| ADC map | Dark (low ADC) confirms true restriction | Distinguishes from T2 shine-through |
| FLAIR | Bright signal = subacute infarct | Timing (if DWI+ but FLAIR- = < 4.5h) |
| T2* / GRE | Susceptibility (blooming) = blood | Detects hemorrhage, microbleeds |
| MRA | Flow void = vessel occlusion | Non-invasive LVO detection |
| Perfusion (PWI) | Perfusion-diffusion mismatch = penumbra | Guides thrombectomy in extended windows |
3. Intracerebral Hemorrhage (ICH) - CT
Deep and Lobar Hemorrhages
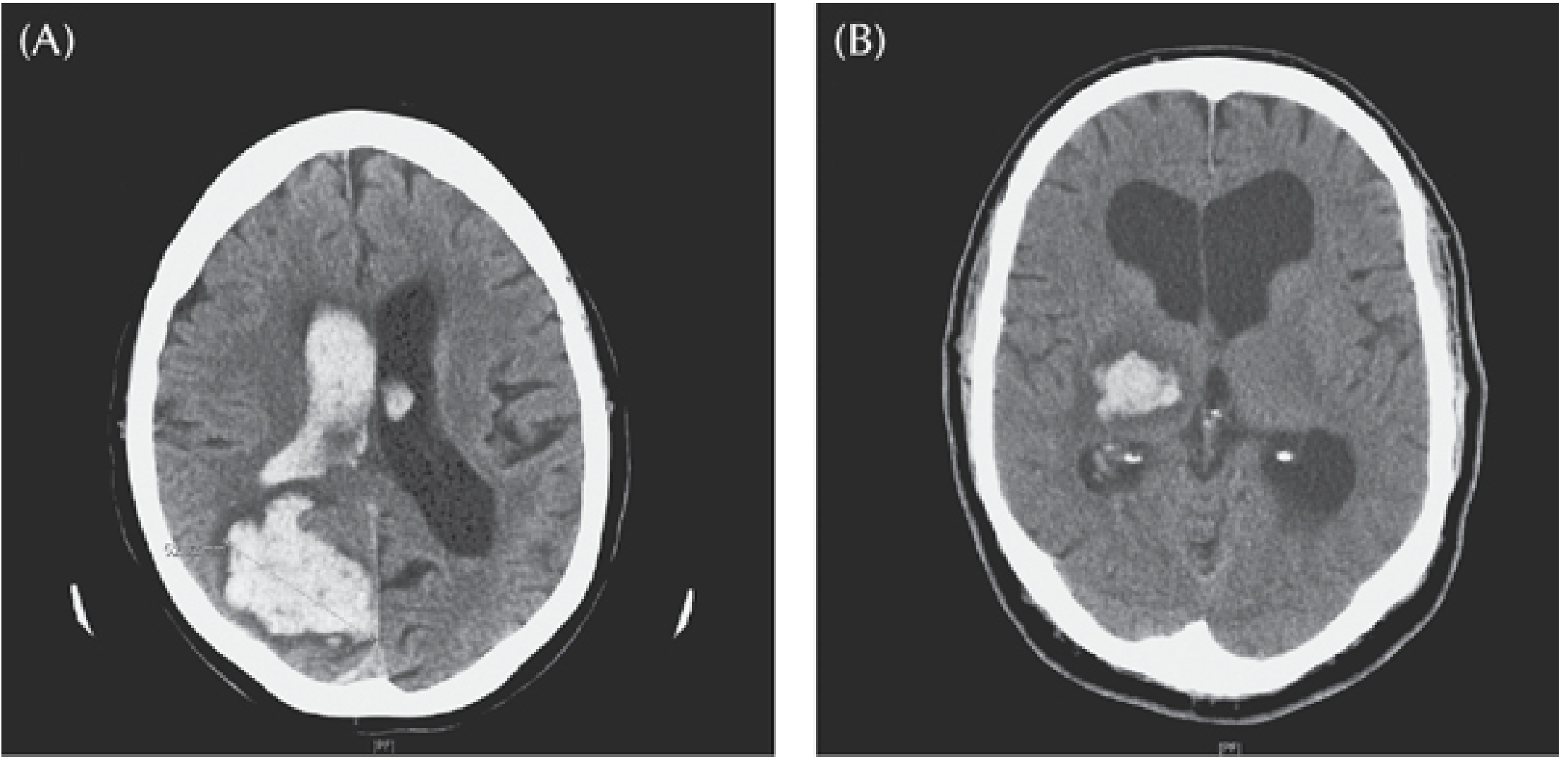
(A) Large hemorrhage into the right parieto-occipital lobe in a 77-year-old woman on aspirin, presenting with left-sided neglect. The hematoma has ruptured into the lateral ventricle (intraventricular extension - a poor prognostic sign).
(B) Right thalamocapsular hemorrhage in a 60-year-old hypertensive man presenting with headache, left-sided weakness, and sensory loss. Note the bright white (hyperdense) lesion in the posterior thalamic/internal capsule region - classic hypertensive deep hemorrhage location.
CT appearance of ICH:
- Acute (0-72h): Hyperdense (bright white), 40-80 Hounsfield Units, round or oval
- Subacute (days-weeks): Progressively isodense as clot retracts, rim enhancement possible
- Chronic: Hypodense (dark), slit-like defect
Right Temporal ICH (Arrow Sign)
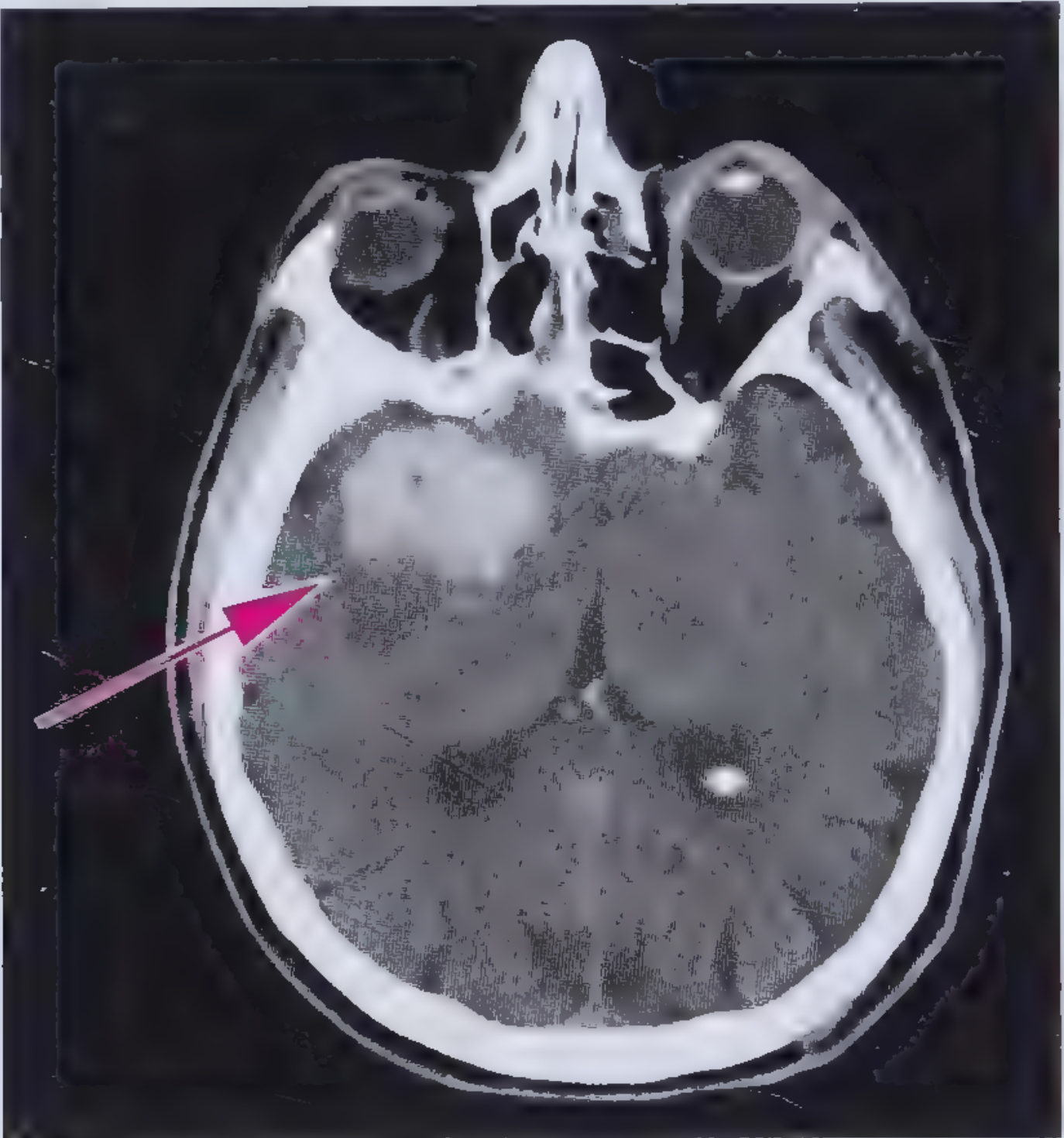
Classic non-contrast CT showing a hyperdense (bright) area in the right temporal lobe corresponding to acute ICH. The pink arrow points to the hematoma, measuring 40-80 HU in attenuation. This appearance is pathognomonic for acute blood on CT.
4. Subarachnoid Hemorrhage (SAH) - CT + CT Angiography
SAH from Ruptured Anterior Communicating Artery Aneurysm
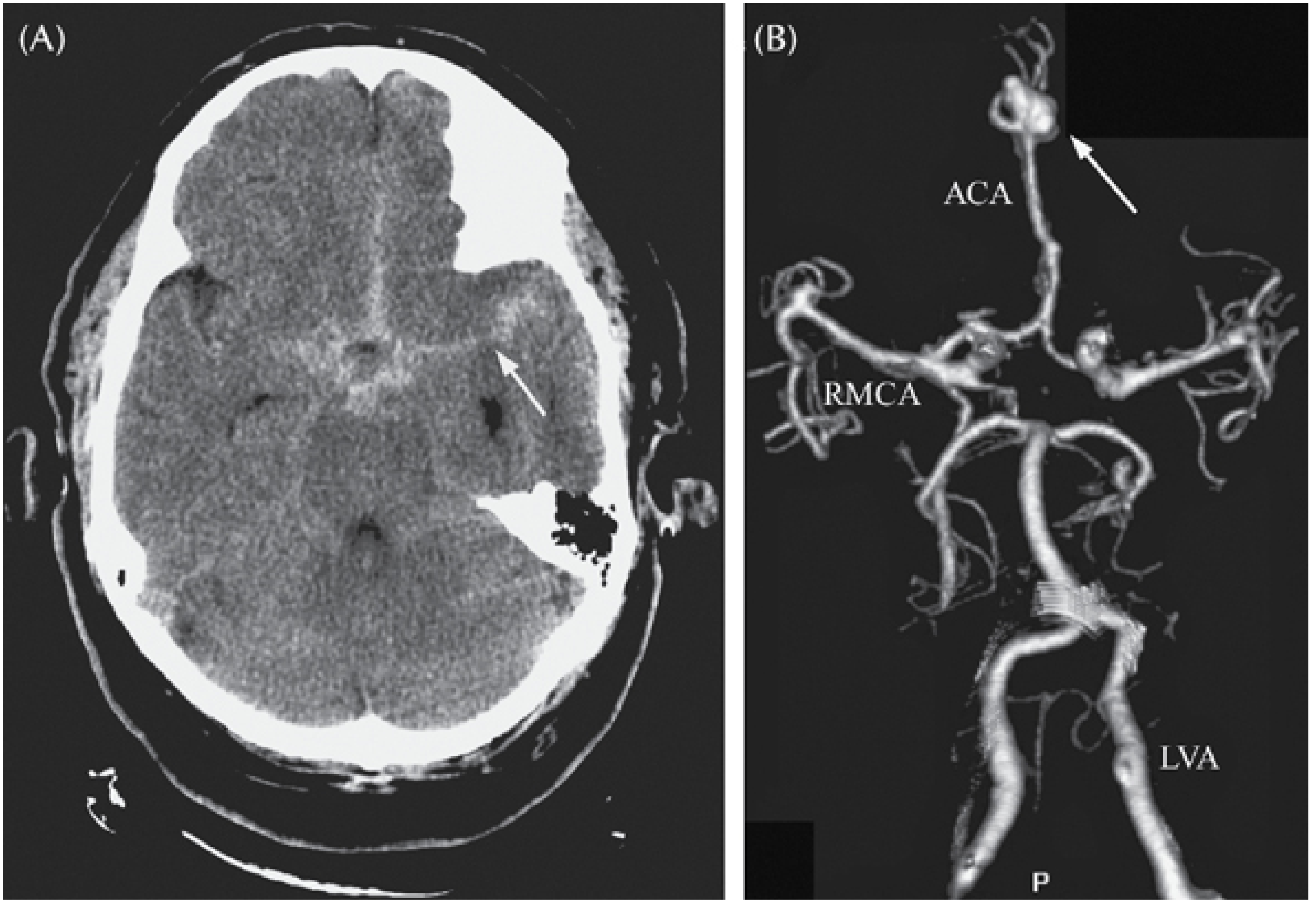
(A) Non-contrast CT: Blood (hyperdense/white) filling the cisterns surrounding the Circle of Willis at the skull base, extending into the interhemispheric fissure and the right Sylvian fissure (arrow). This is the classic "star sign" pattern of aneurysmal SAH.
(B) CT Angiogram (3D reconstruction): Shows the cerebrovascular tree. The arrow points to a large saccular aneurysm at the anterior communicating artery (ACoA) junction - the most common site for aneurysmal SAH. ACA = anterior cerebral artery; RMCA = right MCA; LVA = left vertebral artery.
SAH on CT:
- Sensitivity: ~98% within 12 hours of onset
- Falls to ~85-90% by 24 hours (blood becomes isodense)
- If CT negative but high clinical suspicion: LP for xanthochromia (CSF yellow discoloration from bilirubin)
- Grading: Fisher grade correlates blood burden with vasospasm risk
5. Bilateral Temporal Lobe Infarcts - CT
Cortical Deafness from Bilateral MCA Territory Strokes
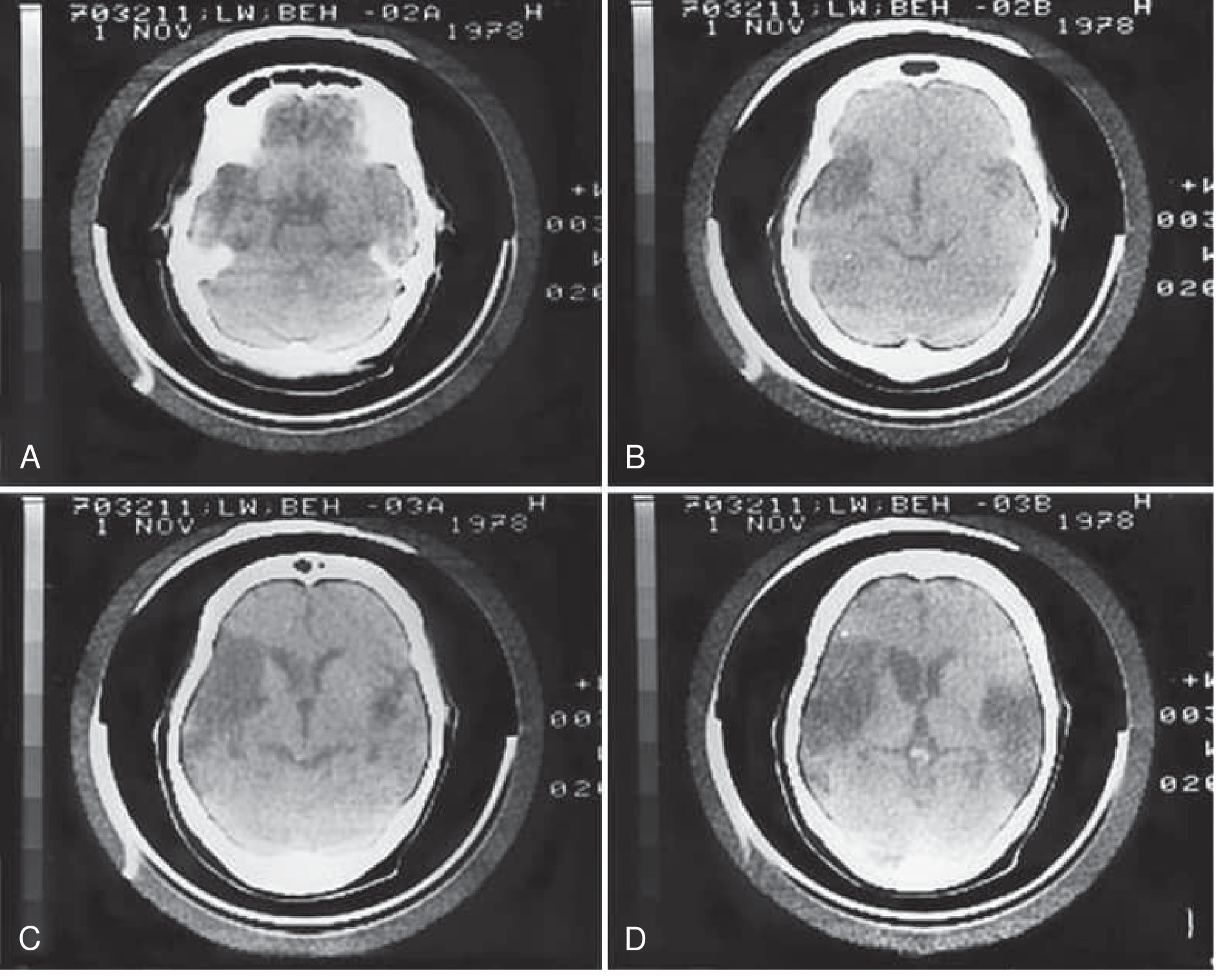
Four sequential axial CT slices showing old (chronic) infarcts affecting the temporal lobes bilaterally - presenting as hypodense (dark) areas. This patient developed cortical deafness - she could hear pure tones but could not comprehend speech, due to destruction of the primary auditory cortex bilaterally.
6. Intracranial Angiography - MCA Stenting
Pre- and Post-Wingspan Stent for M1 MCA Stenosis
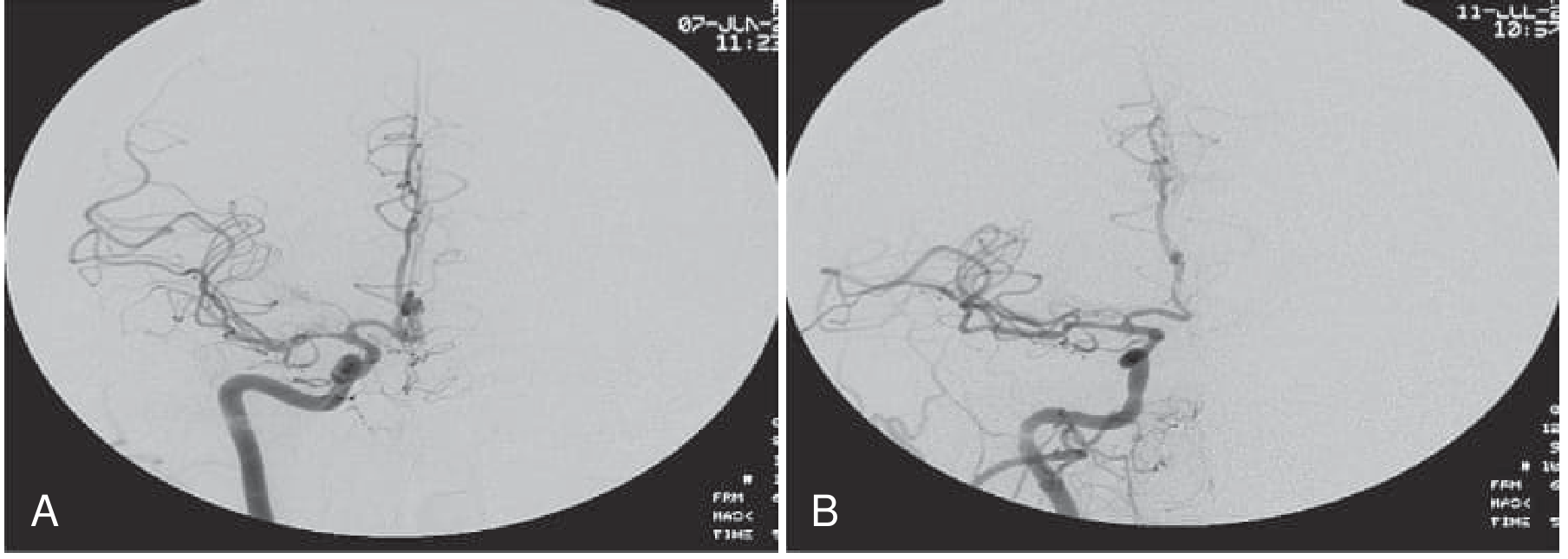
Digital subtraction angiography (DSA) in a 56-year-old man who had recurrent strokes despite optimal medical therapy, with a 65-70% focal stenosis of the M1 segment of the right MCA:
(A) Pre-stent: The proximal MCA shows critical focal stenosis, with reduced distal filling.
(B) Post-stent (Wingspan intracranial stent): The stent wire is in place following deployment; the MCA lumen is restored with improved distal flow.
Summary: What to Look for on Imaging
| Stroke Type | Modality | Key Finding |
|---|---|---|
| Ischemic - hyperacute | CT (plain) | Loss of insular ribbon, MCA hyperdense sign, sulcal effacement |
| Ischemic - established | CT (plain) | Wedge-shaped hypodensity in arterial territory |
| Ischemic | DWI MRI | Bright signal (restricted diffusion) - earliest sensitive marker |
| Ischemic - timing | DWI + FLAIR | DWI+/FLAIR- mismatch = likely < 4.5h (thrombolysis window) |
| LVO | CTA | Vessel cutoff; absence of filling in ICA/MCA/basilar |
| Penumbra | CT/MR perfusion | Mismatch between infarcted core and at-risk tissue |
| ICH | CT (plain) | Hyperdense round/oval lesion, +/- IVH, mass effect |
| SAH | CT (plain) | Hyperdensity in basal cisterns, Sylvian fissures, sulci |
| SAH source | CTA/DSA | Saccular aneurysm (ACoA, PCoA, MCA bifurcation most common) |
Sources: Rosen's Emergency Medicine (p. 1432-1439); Bradley and Daroff's Neurology in Clinical Practice (p. 1405); Plum and Posner's Diagnosis and Treatment of Stupor and Coma (p. 261-273); Frameworks for Internal Medicine (p. 577)
This is a shared conversation. Sign in to Orris to start your own chat.