Difference betweeen radiation , shifting, referred pain
Reading File
Finding Sources
Searching the Web
difference between radiation shifting referred pain clinical medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Now I have enough to give a comprehensive, well-sourced answer.
Radiation, Shifting, and Referred Pain
These three terms describe distinct patterns of pain spread or migration, and are often confused with each other.
1. Radiation of Pain
Pain that travels from its origin along a nerve pathway to a distant site, while remaining felt at both the source and along the course.
- The pain originates at a source and spreads outward along the anatomical path of a nerve or nerve root.
- The patient feels pain continuously from the origin to the distal point — it doesn't "jump" locations.
- Quality is typically sharp, shooting, or burning (neuropathic/radicular character).
- The source and the distal site are anatomically connected by the nerve.
Examples:
- Renal colic → pain radiates from loin to groin along the ureter/genitofemoral nerve distribution
- Cardiac ischemia → pain radiates from the chest to the left arm, jaw, or shoulder (along T1–T4 dermatomes)
- Lumbar disc herniation (L5/S1) → pain radiates down the posterior leg to the foot (sciatica)
- Subacreous diaphragmatic irritation → radiation to the shoulder tip (C3/4 phrenic nerve)
"Radicular pain differs from referred pain in its greater intensity, distal radiation along the course of the nerve containing the affected root, and factors that excite it — stretching, irritation, and compression of the root." — Adams and Victor's Principles of Neurology, 12th Ed.
2. Referred Pain
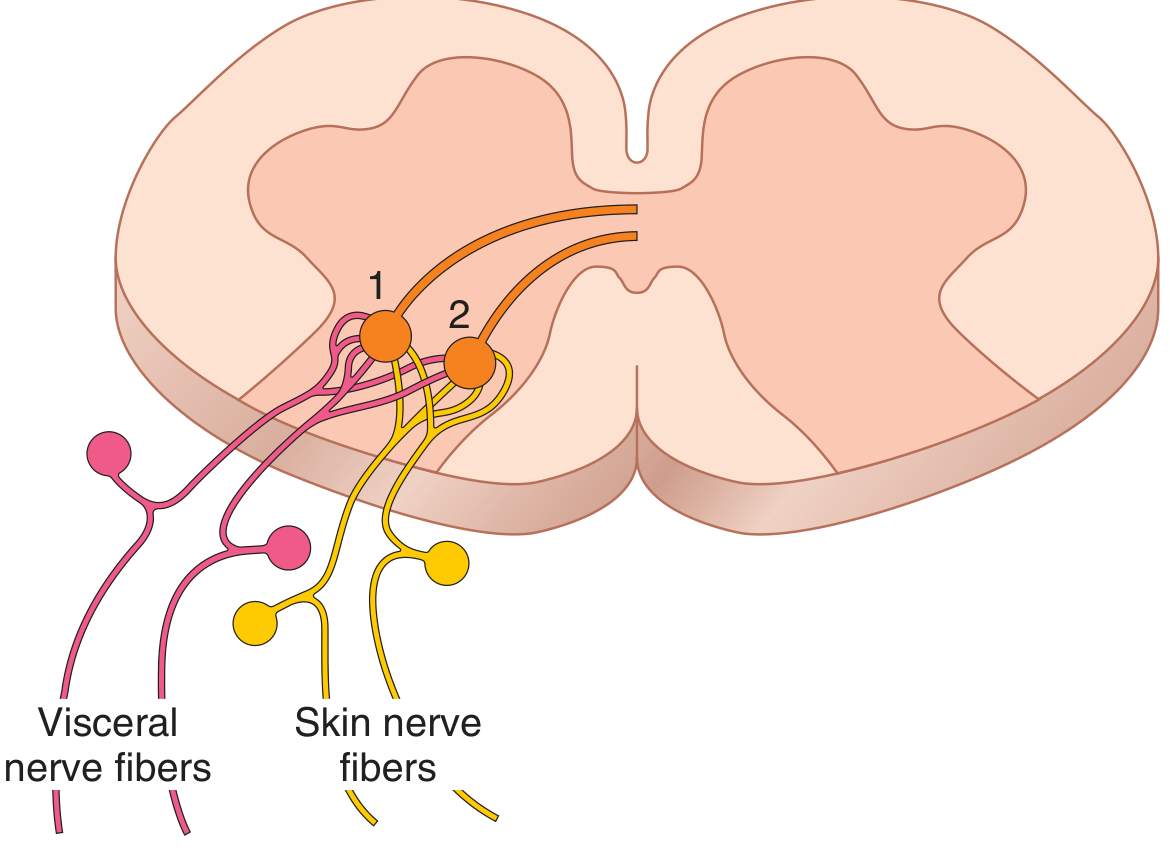
Pain perceived at a site distant from and not anatomically connected to its actual source — caused by convergence of visceral and somatic afferents on the same spinal cord neurons.
Mechanism (convergence theory)
Visceral pain fibers and skin (somatic) pain fibers synapse on the same second-order neurons in the dorsal horn of the spinal cord. The brain, accustomed to pain signals from the skin at that level, misinterprets the visceral signal as coming from the skin/dermatome.
Key features:
- Pain is felt away from the diseased organ, not along a nerve
- There is no continuous path of pain from source to felt site
- The site of referred pain corresponds to the dermatome sharing the same spinal segment as the organ
- Palpating the area of referred pain often does not worsen or may even relieve the pain
- Associated muscle spasm in referred pain diminishes during inspiration (unlike true abdominal pain which persists through both phases)
Examples:
| Source | Referred to | Segment |
|---|---|---|
| Heart (ischemia) | Left arm, jaw | T1–T4 |
| Diaphragm | Shoulder tip | C3–C4 |
| Gallbladder | Right subscapular / tip of right shoulder | T6–T9 |
| Appendix (early) | Periumbilical region | T10 |
| Kidney | Groin/testis | T10–L1 |
Classic example — Appendicitis:
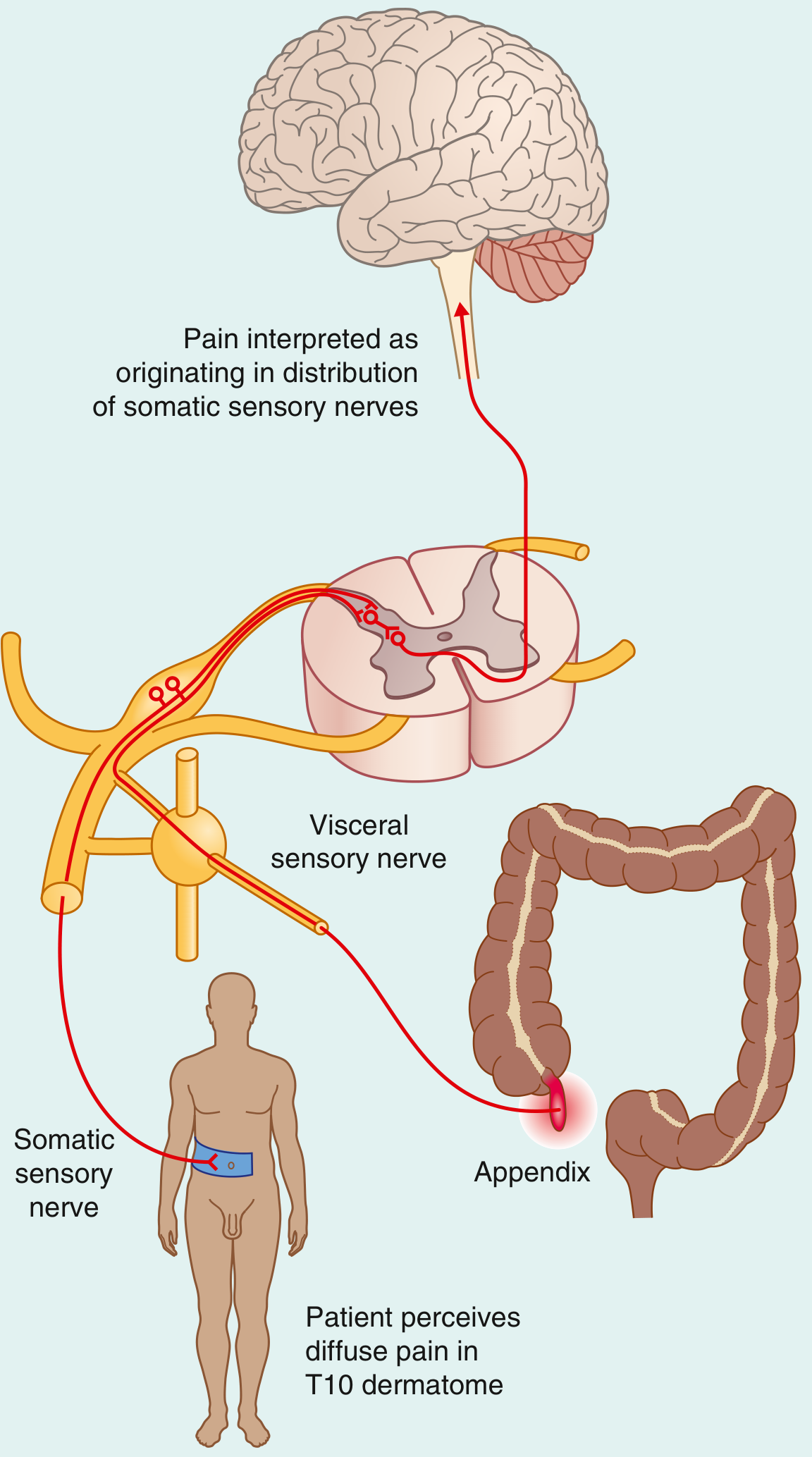
"When the appendix initially becomes inflamed, visceral sensory fibers are stimulated. These fibers enter the spinal cord with the sympathetic fibers at T10. The pain is referred to the T10 dermatome — the umbilical region. The pain is diffuse, not focal." — Gray's Anatomy for Students
3. Shifting (Migrating) Pain
Pain that moves from one location to another as the disease progresses — reflecting a change in the underlying pathophysiological process.
- The original pain disappears or diminishes and a new pain appears elsewhere.
- This is not simultaneous in two locations — it migrates over time.
- It reflects a transition from visceral inflammation → parietal peritoneal involvement (or equivalent transition in other organs).
Classic example — Appendicitis (again, the best teaching case):
- Early phase: Diffuse, colicky, periumbilical pain (visceral/referred → T10 dermatome)
- Later phase: As the inflamed appendix contacts and irritates the parietal peritoneum of the right iliac fossa (somatic innervation), pain shifts to and localizes at McBurney's point (RIF)
"In the later stages of the disease, the appendix contacts and irritates the parietal peritoneum in the right iliac fossa, which is innervated by somatic sensory nerves. This produces a constant focal pain, which predominates over the colicky pain the patient felt some hours previously. The patient no longer interprets the referred pain from the T10 dermatome." — Gray's Anatomy for Students
The shift marks a clinically important transition: from vague visceral pain to localized somatic pain — and indicates peritoneal involvement, a surgical urgency signal.
Summary Comparison Table
| Feature | Radiation | Referred Pain | Shifting Pain |
|---|---|---|---|
| Definition | Pain spreads along a nerve from source | Pain felt far from source, mislocalized by CNS | Pain moves from one site to another over time |
| Simultaneous at source? | Yes | Source pain may be absent | No — earlier pain diminishes |
| Anatomical nerve path? | Yes (follows nerve/dermatome) | No (convergence in spinal cord) | No — reflects disease progression |
| Mechanism | Direct neural conduction along nerve root | Viscero-somatic convergence in dorsal horn | Transition from visceral to parietal involvement |
| Quality | Sharp, shooting, lancinating | Dull, aching, diffuse | Changes character (colicky → constant) |
| Palpation at distant site | Worsens pain | Does NOT usually worsen | Site-specific |
| Classic example | Sciatica, renal colic | Cardiac pain to left arm; early appendicitis at umbilicus | Appendicitis shifting from periumbilical → RIF |
Sources:
- Guyton and Hall Textbook of Medical Physiology — Referred Pain & Mechanism
- Gray's Anatomy for Students — Appendicitis as referred/shifting pain example
- Harrison's Principles of Internal Medicine 22E — Referred Pain in Abdominal Disease
- Adams and Victor's Principles of Neurology, 12th Ed. — Radicular vs. referred pain
Why signs of inflammation are absent in Cold abscess
Finding Sources
Searching the Web
cold abscess signs of inflammation absent mechanism tuberculosis pathophysiology
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading Web Page
why signs of inflammation absent cold abscess mechanism
Finding Sources
I now have comprehensive information to give a thorough answer. Let me compile it.
Why Are Signs of Inflammation Absent in a Cold Abscess?
What Is a Cold Abscess?
A cold abscess is a localized collection of pus (liquefied caseous material) that forms without the classical cardinal signs of acute inflammation — i.e., no calor (heat), rubor (redness), dolor (pain), or tumor (swelling beyond a fluctuant mass). The word "cold" reflects the absence of these acute inflammatory features despite active disease.
It is most classically seen in tuberculosis (TB), but also in atypical mycobacterial infections, actinomycosis, blastomycosis, and leprosy.
The Core Reason: Chronic Granulomatous Inflammation, NOT Acute Inflammation
The cardinal signs of inflammation are produced by acute inflammation — driven by vasodilation, increased vascular permeability, and neutrophil recruitment, triggered by prostaglandins, histamine, bradykinin, and cytokines like IL-1 and IL-8.
In TB, the immune response is fundamentally different — it is a chronic, cell-mediated (Type IV / delayed-type hypersensitivity) response, which generates granulomas rather than the acute inflammatory cascade. This is why each sign is absent.
Mechanism in Detail
1. M. tuberculosis Resists and Suppresses Acute Immune Activation
M. tuberculosis has evolved powerful immune evasion strategies:
- Blocks phagolysosome fusion by recruiting coronin → activating calcineurin → inhibiting phagosome-lysosome fusion. The bacterium survives inside macrophage phagosomes, replicating slowly without triggering massive cell death or cytokine storms.
- Suppresses IL-1α and IL-1β production: Type I interferons induced by MTB suppress IL-1, which is a key mediator of acute inflammation and fever.
- Slow replication rate: MTB replicates every ~24 hours (vs. hours for pyogenic bacteria like Staphylococcus), producing a low-grade, sustained antigenic stimulation rather than an acute overwhelming infection that triggers rapid neutrophil recruitment.
"Innate and adaptive interferons suppress IL-1α and IL-1β production by distinct pulmonary myeloid subsets during Mycobacterium tuberculosis infection." — Murray & Nadel's Textbook of Respiratory Medicine
2. The Immune Response Is Th1 / Cell-Mediated, Not Neutrophilic
After ~3 weeks of infection, the host mounts a Th1 T-cell response:
- Th1 cells produce IFN-γ, which activates macrophages
- Activated macrophages differentiate into epithelioid histiocytes and fuse into Langhans giant cells
- These form the granuloma — a walled-off structure designed to contain the organism
This is a lymphocyte–macrophage interaction, not a neutrophil-mediated acute response. Without neutrophil degranulation and the release of prostaglandins/vasoactive amines at the lesion site, there is no vasodilation, no heat, no redness.
"Macrophages activated by IFN-γ differentiate into 'epithelioid histiocytes' that aggregate to form granulomas; some fuse to form giant cells." — Robbins, Cotran & Kumar Pathologic Basis of Disease
3. Caseous Necrosis Replaces Pus Formation
In pyogenic (acute) abscesses, pus = viable + dead neutrophils + proteolytic enzymes → generates heat, redness, and pain.
In TB:
- The center of the granuloma undergoes caseous necrosis — a cheese-like, avascular, acellular material
- This results from the combined effect of ischemia + delayed hypersensitivity-mediated tissue destruction
- The caseous material liquefies slowly over time, accumulating to form the cold abscess
- No neutrophilic exudate → no pyrogens, no prostaglandins released locally → no heat or redness
4. The Abscess Develops Slowly, Spread Along Fascial Planes
Because the process is chronic and granulomatous:
- No rapid tissue distension (no acute edema) → minimal pain
- The abscess progressively dissects along fascial planes and ligaments following the path of least resistance — tracking to distant sites (e.g., psoas abscess tracking to groin/thigh from a lumbar TB focus)
- There is no acute perilesional edema or vasodilation
"This process occurs with minimal release of acute inflammatory mediators. As a result, classical signs of inflammation — pain, warmth, erythema, and tenderness — are conspicuously absent." — BoneAndSpine.com (citing TB surgical literature)
Summary Table
| Feature | Pyogenic (Hot) Abscess | Cold Abscess (TB) |
|---|---|---|
| Organism | Staph aureus, pyogenic bacteria | M. tuberculosis, atypical mycobacteria |
| Type of inflammation | Acute (neutrophilic) | Chronic granulomatous (cell-mediated) |
| Dominant immune cell | Neutrophils | Macrophages / T lymphocytes |
| Pus contents | Neutrophils, bacteria, proteases | Caseous (cheesy) necrotic material |
| Onset | Rapid (days) | Slow (weeks to months) |
| Heat (Calor) | Present (vasodilation) | Absent — no acute vasodilation |
| Redness (Rubor) | Present | Absent |
| Pain (Dolor) | Present | Absent (minimally tender) |
| Tenderness | Marked | Absent or minimal |
| Fluctuation | Tense, tender | Soft, non-tender fluctuant swelling |
| Fever | Often high | Low-grade or absent |
When Does a Cold Abscess Show Signs of Inflammation?
Only in two circumstances:
- When it is about to burst through the skin — secondary somatic tissue involvement triggers acute reactivity
- Secondary (mixed) infection with pyogenic organisms — superimposed acute inflammation develops on top of the chronic process
Common Sites of Cold Abscess (TB)
- Spinal TB (Pott's disease) → Psoas abscess → tracks to groin, Scarpa's triangle, or thigh
- Cervical TB lymphadenitis (Scrofula) → Neck swelling with violaceous overlying skin
- Rib/chest wall TB → Chest wall fluctuant swelling
- Epididymal TB → Scrotal cold abscess
Sources: Robbins Pathologic Basis of Disease; Murray & Nadel's Respiratory Medicine; Gray's Anatomy for Students; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.