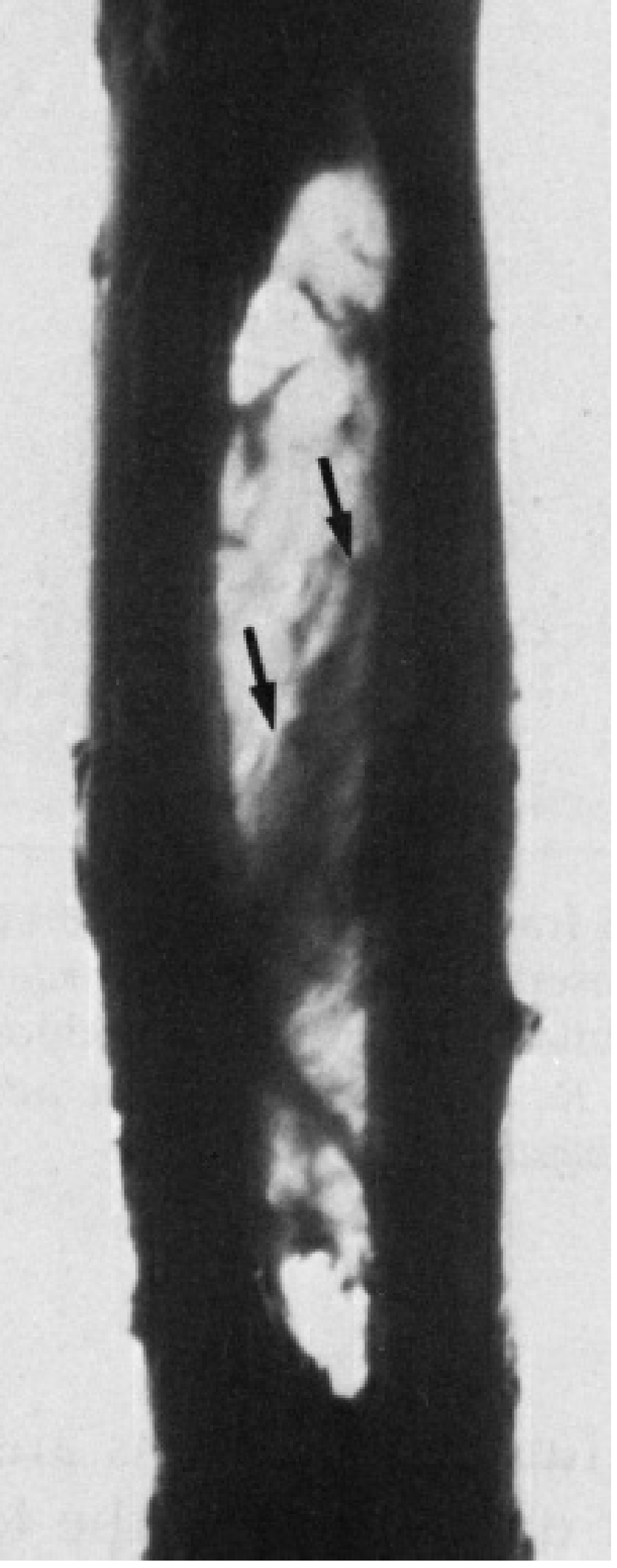
Posterior interosseuos membrane
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Posterior (Forearm) Interosseous Membrane
Note: Although "posterior interosseous membrane" can refer to the membrane of the forearm as seen from its posterior aspect, anatomically the forearm has one interosseous membrane spanning the interosseous borders of the radius and ulna. The term "posterior interosseous membrane" is sometimes used loosely to describe this structure, or specifically to contrast it with the oblique cord (anterior cord). The following covers the forearm interosseous membrane comprehensively, including its posterior relations.
Anatomy
The interosseous membrane (IOM) is a thin but tough fibrous sheet connecting the interosseous (medial) border of the radius to the interosseous (lateral) border of the ulna along most of their lengths. - Gray's Anatomy for Students
Attachments:
- Proximally: begins just inferior to the radial tuberosity (free upper margin)
- Distally: ends at the distal radio-ulnar joint; a small circular aperture exists in its distal third
Fiber Orientation:
- Collagen fibers run predominantly obliquely downward and medially - from the radius (proximally) to the ulna (distally), at approximately 20 degrees to the long axis of the forearm
- This obliquity is mechanically significant: it allows load transfer from the radius to the ulna
Key Structural Component - The Central Band (Interosseous Ligament):
- The IOM has a marked central thickening called the central band (also called the interosseous ligament)
- It is approximately 3.5 cm wide
- Fibers run obliquely from proximal-radial to distal-ulnar
- The central band contributes ~71% of the longitudinal stiffness of the IOM after radial head resection (Hotchkiss et al., 1989) - Rockwood & Green's Fractures in Adults, 10th ed.
Related Structure: The Oblique Cord
Superior to the IOM, a separate ligamentous band called the oblique cord runs in the opposite direction (from ulna to radius, proximally). It is distinct from the IOM proper.
Functions
1. Load / Force Transfer
The IOM engages especially during supination, distributing axial loads from the radius to the ulna. This is essential because the humeroradial articulation is smaller than the humeroulnar and cannot tolerate the same compressive forces. During a fall on an outstretched pronated hand, axial force is transmitted through the radius - without the IOM, this overwhelms the radial head. - Imaging Anatomy, Vol. 3
Force flow: Hand → radius → IOM → ulna → humerus
2. Syndesmotic Joint
The IOM connects the radius and ulna as a syndesmosis - it holds the two bones together without preventing pronation and supination. The interosseous space is greatest in full supination. - Rockwood & Green's
3. Muscle Attachment
Numerous forearm muscles originate from the IOM on both its anterior (volar) and posterior (dorsal) surfaces:
- Posterior/dorsal side: Extensor pollicis longus, extensor pollicis brevis, abductor pollicis longus, extensor indicis (origin from dorsal surfaces of radius, ulna, and IOM)
- Anterior/volar side: Flexor digitorum profundus, flexor pollicis longus
4. Compartment Separator
The IOM forms the posterior limit of the anterior (volar) compartment of the forearm and the anterior limit of the posterior (dorsal) compartment. - Rockwood & Green's
Vascular Apertures
- Proximal free margin (superior): The posterior interosseous artery passes over/dorsal to the proximal margin of the IOM from the anterior compartment into the posterior compartment
- Distal aperture: The anterior interosseous artery passes through this aperture distally to contribute to the dorsal carpal arch
- Anterior interosseous artery: Runs along the anterior surface of the IOM throughout its course, supplying the anterior compartment muscles
Clinical Significance
Essex-Lopresti Injury
The most clinically important IOM injury. A high-energy fall on an outstretched hand causes:
- Fracture/dislocation of the radial head (the primary longitudinal stabilizer)
- Rupture of the IOM (especially the central band)
- Disruption of the distal radio-ulnar joint (DRUJ)
This triad results in longitudinal radioulnar dissociation - the radius migrates proximally, and the ulna head subluxes at the wrist. - Rosen's Emergency Medicine
Clinical features: Elbow pain + wrist pain + grip weakness + pronation weakness
Diagnosis:
- Plain X-ray often shows only an isolated radial head fracture (easily missed)
- Look for positive ulnar variance and widened DRUJ
- MRI is the study of choice for IOM integrity
- Ultrasound is increasingly used Management: Urgent orthopedic referral (within 7-10 days). Options include radial head replacement, IOM central band reconstruction, ulnar shortening.
Forearm Compartment Syndrome
The IOM forms a boundary of the relatively closed compartments of the forearm; increased intracompartmental pressure can be transmitted between compartments via the IOM apertures.
Congenital Radioulnar Synostosis
A narrow interosseous membrane is one of the anatomical encumbrances that complicates surgical correction of radioulnar synostosis. - Campbell's Operative Orthopaedics, 15th ed. 2026
Surgical Importance: Posterior Interosseous Nerve (PIN)
The posterior interosseous nerve (deep branch of the radial nerve) is closely related to the IOM region - it passes between the superficial and deep heads of the supinator and runs in the posterior compartment of the forearm. During radial head surgery, the forearm is kept pronated to protect the PIN. - Rockwood & Green's
Summary Table
| Feature | Detail |
|---|---|
| Type | Fibrous syndesmosis / interosseous membrane |
| Connects | Radius (medial border) to ulna (lateral border) |
| Fiber direction | Oblique: proximal-radial → distal-ulnar (~20° to forearm axis) |
| Key structure | Central band (interosseous ligament) - 3.5 cm wide, 71% longitudinal stiffness |
| Proximal margin | Free; just below radial tuberosity |
| Distal aperture | For anterior interosseous artery |
| Main functions | Load transfer, syndesmosis, muscle origin, compartment separation |
| Key injury | Essex-Lopresti (IOM rupture + radial head fracture + DRUJ dislocation) |
| Imaging | MRI = gold standard for IOM integrity |
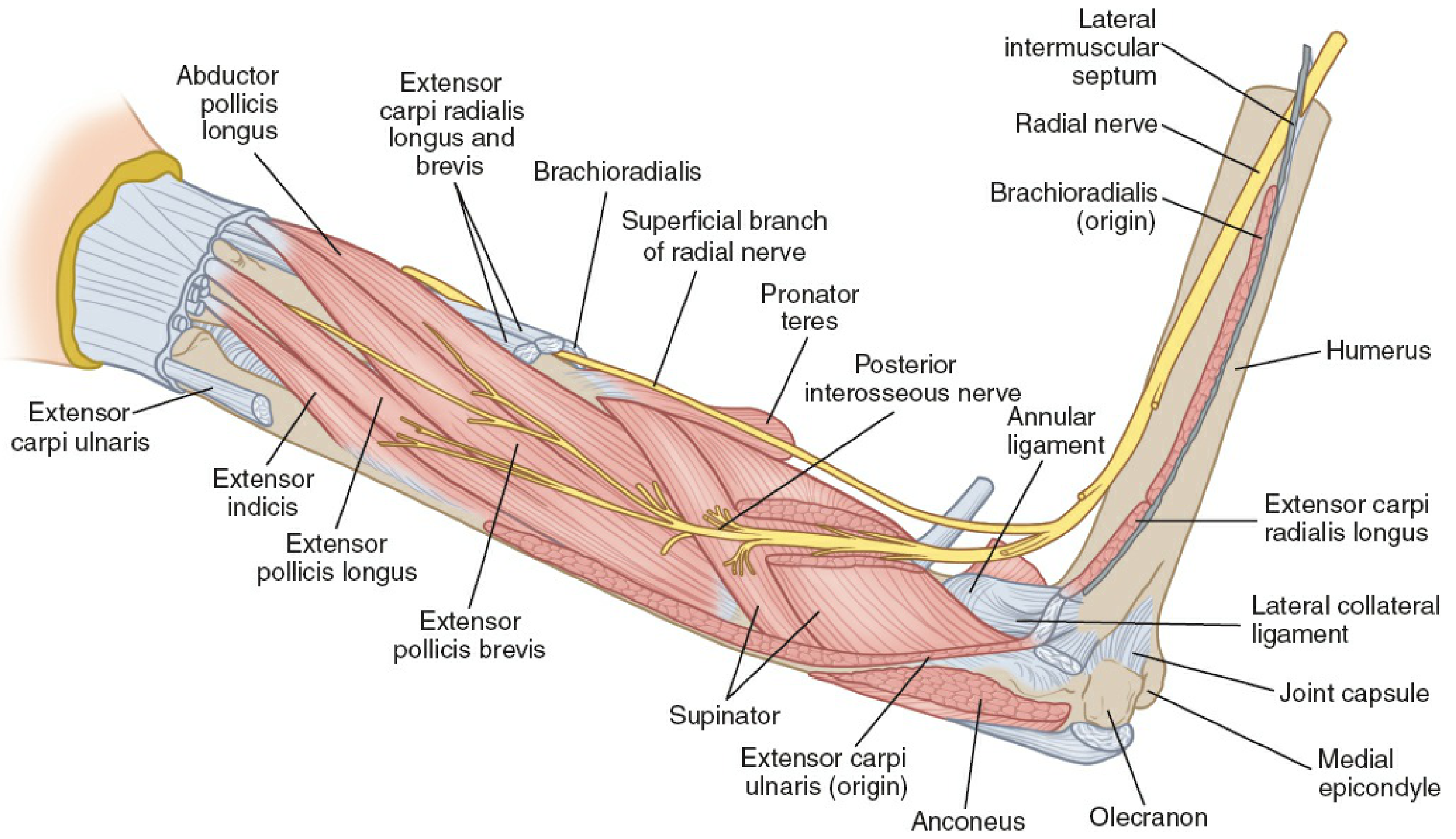
Posterior interosseous nerve
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Excellent - I have all the material I need for a thorough answer. Here it is:
Posterior Interosseous Nerve (PIN)
Origin and Root Value
The PIN is the deep terminal branch of the radial nerve, carrying motor fibers from C7 and C8 (via the posterior cord of the brachial plexus). The radial nerve divides into its superficial (sensory) and deep (motor) branches at the level of the lateral epicondyle / cubital fossa. - Gray's Anatomy for Students
The deep branch is called the posterior interosseous nerve only after it emerges from the distal border of the supinator muscle. Before that, it is simply the "deep branch of the radial nerve."
Course
The PIN's course can be divided into four segments:
1. Cubital Fossa / Lateral Epicondyle Region
- The radial nerve enters the forearm between the brachioradialis and brachialis muscles
- It gives off branches here to: brachioradialis, ECRL (and sometimes ECRB) - before dividing
- It then divides into the superficial radial nerve (sensory) and the deep branch (future PIN)
2. Radial Tunnel
- The deep branch dips beneath the origin of ECRB, entering the radial tunnel - a potential space approximately 5 cm long
- Boundaries of the radial tunnel:
- Posterior: capitulum and radiocapitellar joint
- Medial: brachialis
- Anterolateral: brachioradialis, ECRL, ECRB
- It innervates ECRB and supinator here
3. Through the Supinator (Arcade of Frohse)
- The deep branch pierces the supinator muscle through its fibrous proximal edge - the Arcade of Frohse (first described by Fritz Frohse in 1908)
- It courses between the superficial and deep layers of the supinator, winding laterally and posteriorly around the proximal radius
- It emerges from the distal border of supinator as the posterior interosseous nerve
4. Posterior Compartment of Forearm
- The PIN travels between the superficial and deep extensor muscle layers, running on the posterior surface of the interosseous membrane
- It gives off 6 branches (from proximal to distal) to: ECU, EDM, EDC, EPB+EPL, APL, and EIP
- It terminates as articular branches to the dorsal wrist capsule, located on the floor of the 4th extensor compartment
Muscles Innervated
| Muscle | Note |
|---|---|
| Extensor carpi radialis brevis (ECRB) | Innervated before entering supinator |
| Supinator | Innervated within the supinator |
| Extensor digitorum communis (EDC) | After exiting supinator |
| Extensor digiti minimi (EDM) | After exiting supinator |
| Extensor carpi ulnaris (ECU) | After exiting supinator |
| Abductor pollicis longus (APL) | After exiting supinator |
| Extensor pollicis brevis (EPB) | After exiting supinator |
| Extensor pollicis longus (EPL) | After exiting supinator |
| Extensor indicis proprius (EIP) | Last muscle innervated; last to recover |
ECRL is innervated by the radial nerve proper (before division), so it is always spared in PIN palsy.
Brachioradialis is also innervated before the division and is spared.
Mnemonic for first vs last innervated: First = Brachioradialis; Last = EIP
Sensory Function
The PIN is purely motor in the forearm. It carries no cutaneous sensation.
However, it provides articular/proprioceptive branches to the dorsal wrist capsule - patients with PIN syndrome may describe dorsal wrist pain from this terminal sensory contribution. - Miller's Review of Orthopaedics, 9th ed.
There is no reflex loss with PIN injury (brachioradialis reflex is mediated by the radial nerve before PIN division).
Sites of Compression / Entrapment (Radial Tunnel)
The PIN can be compressed at 4 sites along the radial tunnel. Mnemonic: LEAFS (©Kakar): - Miller's Review of Orthopaedics
| # | Structure | Notes |
|---|---|---|
| 1 | Leash of Henry (radial recurrent artery fan) | Tethers the nerve |
| 2 | Edge of ECRB (medial fibrous edge) | Fibrous origin compresses the nerve |
| 3 | Arcade of Frohse | Most common site - proximal fibrous edge of supinator |
| 4 | Fascial band at the radial head | Fibrous bands over the radiocapitellar joint |
| 5 | Supinator distal edge | Occasionally compresses as nerve exits |
Additional causes: fracture-dislocations of the elbow, Monteggia fracture-dislocation, Volkmann ischemic contracture, chronic radial head dislocation, RA synovitis, lipoma, aneurysm, or enlarged bursa. - Campbell's Operative Orthopaedics, 15th ed. 2026
Clinical Syndromes
PIN Palsy (Posterior Interosseous Nerve Syndrome)
Pure motor deficit - no sensory loss, no reflex change.
Features:
- Weakness/paralysis of finger and thumb extensors at the MCP joints
- ECU paralysis → wrist deviates radially on attempted extension (because ECRL and ECRB are spared)
- Cannot extend fingers at MCP joints (distinguish from extensor tendon rupture by normal wrist tenodesis test)
- No wrist drop (ECRL and ECRB are intact)
- No sensory loss
Two types (Spinner's classification): - Campbell's Operative Orthopaedics
- Complete - all muscles supplied by PIN are paralyzed
- Incomplete - only one or a few muscles are affected
Causes: Trauma, RA synovitis (most common inflammatory cause), space-occupying lesions
Investigations:
- EMG/NCS confirms diagnosis
- MRI identifies space-occupying lesions
Treatment:
- Non-operative: activity modification, splinting, NSAIDs (first line)
- Surgical decompression if no recovery by 3 months - good/excellent results in ~85% - Miller's Review of Orthopaedics
Radial Tunnel Syndrome
A distinct entity from PIN palsy:
- Pain only in the lateral proximal forearm - no motor or sensory deficit
- Point of maximal tenderness is 3-4 cm distal to the lateral epicondyle (vs. lateral epicondylitis at the epicondyle itself)
- Provoked by: resisted long finger extension (reproduces pain) and resisted supination
- EMG is typically inconclusive/normal
- Can coexist with lateral epicondylitis in a small % of cases
- Treatment: prolonged non-operative (up to 1 year); surgical decompression gives good-excellent results in only 50-80% - less predictable than for PIN palsy - Miller's Review of Orthopaedics
Surgical Relevance
- During radial head surgery, the forearm is kept in pronation to move the PIN away from the operative field and reduce compression risk - Rockwood & Green's
- Retractors should not be placed around the anterior radial neck (risk of PIN compression)
- During posterolateral approach to the elbow, the interval between EDC and ECRL/B is developed down to the level of the PIN entering the supinator at the arcade of Frohse - Campbell's Operative Orthopaedics
Summary
| Feature | Detail |
|---|---|
| Origin | Deep branch of radial nerve (C7, C8) |
| Becomes PIN | After exiting distal border of supinator |
| Course | Between superficial and deep extensors on posterior IOM surface |
| Motor supply | All posterior forearm extensors except ECRL and brachioradialis |
| Sensory supply | None cutaneous; articular branches to dorsal wrist capsule |
| Compression site | Arcade of Frohse (most common) |
| PIN palsy sign | Radial wrist deviation on extension; finger drop at MCP |
| Distinguishing feature | No sensory loss, no reflex change, no true wrist drop |
| Surgery threshold | Decompression if no recovery by 3 months |
This is a shared conversation. Sign in to Orris to start your own chat.