Central neurocytoma imaging features
Reading File
Finding Sources
Finding Sources
Searching PubMed
central neurocytoma MRI imaging features
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive imaging data from two authoritative radiology/neurology textbooks plus an MRI image. Here is the full answer:
Central Neurocytoma - Imaging Features
Overview
Central neurocytoma is a rare, slow-growing WHO Grade II tumor of neuronal lineage, accounting for less than 1% of all primary brain tumors. It most commonly affects patients in the second to fourth decade of life.
Location (Key Imaging Clue)
- Intraventricular: almost exclusively within the lateral ventricles, anteriorly near the foramen of Monro
- Arises from or is closely related to the septum pellucidum and columns of the fornix
- Can extend into the third ventricle through the foramen of Monro
- Rarely, extraventricular neurocytomas arise in cerebral hemispheres, cerebellum, or spinal cord
CT Features
- Well-demarcated, lobulated intraventricular mass
- Calcification is common (frequently visible on CT)
- Small cysts are frequently present
- May be iso- to slightly hyperdense relative to brain parenchyma
- Obstructive hydrocephalus is a common associated finding due to CSF obstruction at the foramen of Monro
MRI Features
| Sequence | Appearance |
|---|---|
| T1 | Isointense to cortical gray matter |
| T2 | Iso- to hyperintense relative to gray matter |
| Post-gadolinium | Variable enhancement - moderate and heterogeneous; sometimes intense and inhomogeneous |
| SWI/GRE | Susceptibility artifact from calcification |
| FLAIR | Heterogeneous signal |
Characteristic Morphology on MRI
- "Bubbly" or "soap-bubble" appearance: multiple septated cysts within the mass
- Heterogeneous signal due to mixture of solid nodules (isointense to gray matter), cysts, calcifications, and flow voids
- Gray-matter-isointense nodules interspersed within the cystic components
- Sharply demarcated margins, non-infiltrative
- No significant surrounding edema (unlike high-grade tumors)
Below is an MRI of a central neurocytoma - axial proton density (A) and coronal T1 post-gadolinium (B) - showing a partly cystic, multi-septated, enhancing mass related to the septum pellucidum filling both lateral ventricles with resultant hydrocephalus:
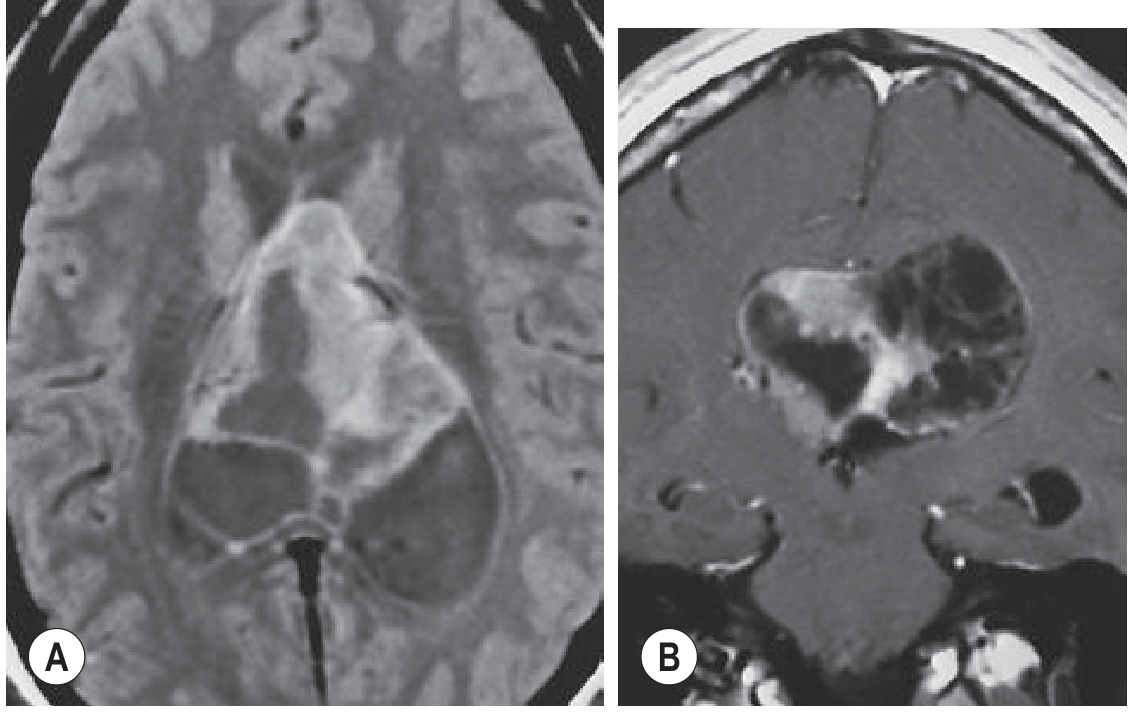
Axial proton density (A) and coronal T1 post-gadolinium (B). A partly cystic, multi-septated, enhancing mass fills the bodies of both lateral ventricles, causing hydrocephalus with dilatation of the left temporal horn. - Grainger & Allison's Diagnostic Radiology
Advanced MRI / Functional Imaging
- MR Spectroscopy: Elevated glycine peak at 3.55 ppm (relatively specific for central neurocytoma); elevated choline, reduced NAA
- DWI: Variable; usually not restricted diffusion (unlike high-grade tumors)
- Perfusion MRI: May show elevated rCBV in solid components
Key Differential Diagnoses
| Diagnosis | Distinguishing Features |
|---|---|
| Subependymoma | Older patients (5th-6th decade); minimal/no enhancement; 4th ventricle more common; no calcification typical |
| Oligodendroglioma | Parenchymal (not purely intraventricular); 1p/19q co-deletion on genetics |
| Intraventricular meningioma | Trigone of lateral ventricle; homogeneous intense enhancement; dural tail (rare intraventricularly) |
| Ependymoma | Fourth ventricle more common; "plastic" extension through foramina |
| Subependymal giant cell astrocytoma (SEGA) | Near foramen of Monro in tuberous sclerosis; intensely enhancing |
Clinical Correlation
- Contrast-enhanced MRI is the modality of choice
- The diagnosis should be considered in any young adult presenting with an anterior intraventricular mass near the foramen of Monro showing cysts, calcification, and heterogeneous enhancement
- Key histological confirmation: synaptophysin-positive immunostaining distinguishes it from oligodendroglioma (which lacks this marker)
- Atypical neurocytomas (MIB-1/Ki-67 >2-3%) have higher recurrence rates
Sources: Bradley and Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology
Co angle mass lesion dd
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have a thorough set of data. Here is the comprehensive answer:
Cerebellopontine (CP) Angle Mass Lesion - Differential Diagnosis
Boundaries of the CP Angle
- Anterior: CN VI and lateral clivus
- Lateral: medial surface of the petrous bone
- Medial: pons, middle cerebellar peduncle, ventral cerebellum
- Superior: CN V (trigeminal)
- Inferior: CN IX, X, XI
- Contained within the space: CN V, VII, VIII, IX, X, XI and the AICA
Relative Frequency
| Lesion | Frequency |
|---|---|
| Vestibular schwannoma (acoustic neuroma) | ~80-90% |
| Meningioma | ~3-10% |
| Epidermoid cyst (primary cholesteatoma) | ~2.5-5% |
| Facial nerve schwannoma | ~1% |
| Paraganglioma | Up to 10% when secondary tumors included |
| Others | Rare |
Common Lesions
1. Vestibular Schwannoma (Acoustic Neuroma) - MOST COMMON
- Benign schwannoma of the vestibular division of CN VIII
- Arises within the internal auditory canal (IAC), expands into the CPA
- Unilateral in 95%; bilateral = NF2 (chromosome 22 mutation)
- CT: Enlargement of IAC (>2 mm asymmetry), no calcification
- MRI: T1 isointense, T2 slightly hyperintense, enhances with gadolinium (moderate-intense, homogeneous or heterogeneous for large lesions)
- Characteristic "ice cream cone" shape with IAC component + CPA component
- No dural tail
2. Meningioma (~10%)
- Second most common CPA lesion
- Eccentric to the IAC (broad dural base; does NOT enter the IAC)
- CT: Iso- to hyperdense; may show calcification; adjacent hyperostosis
- MRI: T1 isointense; T2 signal varies with calcium content (hypo- or hyperintense); intensely and homogeneously enhances
- Dural "tail" sign - enhancing dural extension pathognomonic
- IAC involvement absent or shallow; no IAC erosion/widening typical of schwannoma
3. Epidermoid Cyst (Primary Cholesteatoma)
- Derived from ectodermal remnants; filled with keratin debris
- Has a characteristic "insinuating" growth pattern - wraps around structures rather than displacing them
- CT: Hypodense, no enhancement
- MRI: T1 hypointense, T2 hyperintense (similar to CSF at first glance)
- Key distinguishing feature: DWI - restricted diffusion (bright signal), unlike arachnoid cyst which follows CSF
- No enhancement with gadolinium
- FLAIR: higher signal than CSF (unlike arachnoid cyst)
- MR spectroscopy: elevated aniline, glutamine/glutamate, choline; absent/reduced NAA and creatinine
4. Arachnoid Cyst
- Follows CSF signal on ALL sequences (T1 hypo, T2 hyper, FLAIR suppressed like CSF)
- No enhancement, No DWI restriction - key distinction from epidermoid
- Smooth, well-defined, displaces structures (does not insinuate)
5. Facial Nerve Schwannoma (~1%)
- Imaging nearly identical to vestibular schwannoma
- Clue: may involve the geniculate ganglion or extend along the facial nerve canal
- Presents with facial palsy (unusual for acoustic schwannoma except in late/large disease)
Less Common Lesions
| Lesion | Key Features |
|---|---|
| Paraganglioma (glomus jugulare/tympanicum) | "Salt-and-pepper" on MRI (flow voids + hemorrhage); destructive on CT; pulsatile tinnitus |
| Lipoma | T1 hyperintense, T2 hyperintense; signal disappears with fat suppression; no enhancement |
| Metastasis | Rapid symptom progression; multiple cranial neuropathies; lytic petrous apex lesion; history of primary malignancy (lung, breast, prostate, melanoma) |
| Cholesterol granuloma | T1 hyperintense, T2 hyperintense on ALL sequences (due to cholesterol crystals + blood products); hypointense rim |
| Chordoma | Arises from clivus; midline bone destruction on CT; T2 very hyperintense; lobulated |
| Trigeminal schwannoma | Extends through Meckel's cave to middle fossa ("dumbbell" shape); CN V symptoms |
| Superficial siderosis | T1 and T2 hypointense hemosiderin coating; no enhancement; "blooming" on GRE/SWI |
MRI Imaging Characteristics Summary Table
| Lesion | T1 | T2 | Post-Gad | DWI | Key Clue |
|---|---|---|---|---|---|
| Vestibular schwannoma | Iso | Slightly hyper | Enhances | No restriction | IAC widening; "ice cream cone" |
| Meningioma | Iso | Hypo/hyper | Enhances | No restriction | Dural tail; eccentric to IAC |
| Epidermoid | Hypo | Hyper | No enhancement | Bright (restricted) | Insinuates; FLAIR > CSF |
| Arachnoid cyst | Hypo | Hyper | No enhancement | No restriction | Follows CSF all sequences |
| Lipoma | Hyper | Hyper | No enhancement | - | Fat sat suppression |
| Cholesterol granuloma | Hyper | Hyper | No enhancement | - | Petrous apex; all sequences bright |
| Superficial siderosis | Hypo | Hypo | No enhancement | - | Hemosiderin; blooming on GRE |
Clinical Approach
The most important discriminating question on MRI is:
- Does it involve/expand the IAC? - Yes → schwannoma
- Is there a dural tail? - Yes → meningioma
- Does it restrict on DWI? - Yes → epidermoid
- Does it follow CSF on all sequences? - Yes → arachnoid cyst
- Is it T1 bright? - Fat = lipoma; cholesterol crystal + blood = cholesterol granuloma
Sources: Cummings Otolaryngology Head and Neck Surgery; Bradley and Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.