greenish sputum n nasal discharge thick
Reading File
Finding Sources
Finding Sources
Searching PubMed
purulent sputum acute rhinosinusitis bacterial diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have strong textbook content. Let me compile a thorough answer.
Greenish/Thick Sputum and Nasal Discharge
What does it mean?
Green or yellow-green sputum and thick nasal discharge signal purulent secretions - dominated by neutrophils. The green color comes from myeloperoxidase (an enzyme released by neutrophils), not from bacteria themselves. This means purulent secretions can occur in both viral AND bacterial infections, so the color alone does not confirm a bacterial cause.
Most Likely Diagnosis: Acute Rhinosinusitis (ARS)
The combination of thick/purulent nasal discharge + facial symptoms is the hallmark of acute rhinosinusitis.
Defining symptoms (per American Academy of Otolaryngology guidelines):
- Cardinal signs: Purulent (non-clear) nasal drainage + nasal obstruction AND/OR facial pain/pressure/fullness
- Additional: reduced sense of smell, tooth pain, halitosis, headache, sinus pressure on bending forward, fever
- Duration: 7 days to 4 weeks (acute); beyond 12 weeks = chronic
Viral vs. Bacterial - Key Distinction
Most ARS is viral (rhinovirus, influenza, coronavirus). The diagnosis of acute bacterial rhinosinusitis (ABRS) requires at least ONE of three criteria:
| Criterion | Detail |
|---|---|
| Persistent symptoms | ≥10 days without improvement |
| Severe onset | Fever >39°C with nasal discharge or facial pain for 3-4 days without improvement |
| Double worsening | Initial improvement followed by new worsening of symptoms |
- Textbook of Family Medicine 9e, p. 422
- Rosen's Emergency Medicine, p. 969
Note: 80% of patients on placebo still improve within 2 weeks, so most cases are self-limiting regardless of purulence.
Common Bacteria in Acute Sinusitis
When bacterial, the usual pathogens are:
- Streptococcus pneumoniae (most common)
- Haemophilus influenzae
- Moraxella catarrhalis (~20% of cases)
Beta-lactamase production is common among all three. Chronic sinusitis also involves anaerobes, Pseudomonas, and staphylococci.
Treatment
Supportive (first-line for most patients):
- Nasal saline irrigation - reduces symptom severity
- Intranasal corticosteroid spray - may shorten illness duration
- Topical decongestants (e.g. oxymetazoline) - max 3 days only, to avoid rhinitis medicamentosa
- Avoid routine antibiotics unless bacterial criteria are met
Antibiotics (only if ABRS criteria met):
- First-line: Amoxicillin 500 mg PO three times/day x 5-7 days
- Penicillin allergy: Macrolides, cephalosporins, or fluoroquinolones
- Recent antibiotics (last 4-6 weeks) or treatment failure: High-dose amoxicillin-clavulanate OR a fluoroquinolone
- Plain sinus X-rays and CT are NOT needed for uncomplicated ARS
When to Worry - Complications of Sinusitis
The paranasal sinuses are adjacent to the orbits and brain. Red-flag signs requiring urgent evaluation:
- Periorbital swelling/redness or proptosis (orbital cellulitis/abscess)
- Vision changes
- Severe or worsening headache
- High fever
- Altered mental status (intracranial extension - meningitis, brain abscess, cavernous sinus thrombosis)
CT with contrast is the imaging of choice if complications are suspected. Orbital and intracranial complications require IV antibiotics and specialist (ENT, ophthalmology, infectious disease) input.
- Textbook of Family Medicine 9e, p. 422
- Tintinalli's Emergency Medicine, p. 1620
Other Causes to Consider
If symptoms also include a productive cough with greenish sputum (not just nasal), consider:
- Acute bronchitis - usually viral; antibiotics rarely needed
- Community-acquired pneumonia - if fever, pleuritic chest pain, crackles on auscultation
- Acute exacerbation of COPD/chronic bronchitis - purulent sputum is one criterion (Anthonisen criteria)
- Cystic fibrosis - in younger patients with recurrent episodes
Bottom line: Greenish thick nasal discharge alone most commonly represents a viral upper respiratory infection or early ARS - watchful waiting with supportive care is appropriate for the first 7-10 days. Antibiotics are indicated only if symptoms persist beyond 10 days, are severe, or follow a double-worsening pattern.
3 year old small frequent loose stools more orange yellowish in color with liquid
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Searching PubMed
toddler diarrhea functional chronic loose stool children
I have enough information to provide a comprehensive answer. Let me compile it now.
Small, Frequent, Loose Orange-Yellow Watery Stools in a 3-Year-Old
Most Likely Cause: Toddler's Diarrhea (Functional Diarrhea of Childhood)
The classic description of toddler's diarrhea - also called "irritable colon of infancy" or functional diarrhea of childhood - is:
- Age: 1-4 years
- Multiple (3-6+) small, loose/watery stools per day
- Orange or yellow color, often containing undigested food particles
- Child is well-appearing, gaining weight normally, no blood/mucus
- No pain, no fever, no failure to thrive
This is a benign, self-limiting functional disorder related to rapid intestinal transit. Excess fruit juice, fructose, and sorbitol (poorly absorbed sugars) are common triggers. It typically resolves spontaneously by age 4-5 when the gut matures.
Why Orange-Yellow Color?
| Reason | Explanation |
|---|---|
| Rapid transit | Bile is normally broken down from yellow/green (biliverdin/bilirubin) to brown by gut bacteria. Fast transit means bile doesn't fully convert - stool stays yellow/orange |
| Diet | Orange or yellow foods (carrots, sweet potato, mango, certain formulas) can tint stool |
| Osmotic/carbohydrate malabsorption | Unabsorbed sugars draw water in - watery yellow stool |
| Viral gastroenteritis | Rotavirus and norovirus cause osmotic diarrhea with yellow watery stool |
Differential Diagnosis
1. Acute Infectious Gastroenteritis (most common overall cause of diarrhea at this age)
- Viral (rotavirus, norovirus, adenovirus): watery, yellow-green stools, often with vomiting, low-grade fever; self-limiting
- Bacterial (Salmonella, Shigella, Campylobacter, E. coli): more likely if stool has blood/mucus, high fever, or child appears ill
- Parasitic (Giardia): chronic/recurrent greasy, foul-smelling, pale/yellow stools; bloating; weight loss
2. Toddler's Diarrhea / Functional Diarrhea
- Chronic (>4 weeks), no weight loss, well child, often yellow-orange with food particles
3. Carbohydrate/Lactose Intolerance
- After viral GI illness (secondary lactase deficiency)
- Explosive, frothy, acidic, yellow stools; diaper rash common
- Improves after removing lactose/dairy
4. Food Allergy / Intolerance
- Cow's milk protein allergy; can cause chronic loose stools
- Often with skin (eczema) or respiratory symptoms
5. Celiac Disease
- Chronic, pale/yellow, bulky, fatty stools (steatorrhea); failure to thrive; abdominal distension
- Usually presents after gluten introduction
6. Cystic Fibrosis
- Greasy, bulky, foul stools (steatorrhea); recurrent respiratory infections; failure to thrive
Red Flags - Needs Urgent Evaluation
Any of the following in this 3-year-old requires medical evaluation:
-
Blood or mucus in stool
-
Fever ≥39°C
-
Signs of dehydration: sunken eyes, dry mouth, no tears, decreased urine output, lethargy
-
Failure to thrive / weight loss
-
Bilious (green) vomiting
-
Abdominal distension or pain
-
Diarrhea lasting >2 weeks without improvement
-
Tintinalli's Emergency Medicine, p. 884-888
-
Rosen's Emergency Medicine, p. 3389-3409
Management
For acute gastroenteritis / mild diarrhea (no red flags):
- Continue feeding - do NOT starve the child; resume normal diet early
- Oral rehydration therapy (ORT) - small frequent sips of oral rehydration solution (ORS like Pedialyte); NOT plain water, NOT sugary juices (worsen diarrhea)
- Continue breastfeeding if applicable
- Avoid fruit juice, high-fructose drinks - worsens diarrhea
- Zinc supplementation (in developing country settings) - reduces duration and severity
- Probiotics (Lactobacillus rhamnosus GG, Saccharomyces boulardii) - modest evidence for shortening acute gastroenteritis by ~1 day
- Antibiotics are NOT routinely needed for watery diarrhea
For toddler's diarrhea:
- Reduce fruit juice and high-fructose corn syrup intake
- Increase dietary fat (fat slows transit)
- Normalize fiber intake
- Reassure parents - the child is well, growing, and will outgrow it
Dehydration Warning Signs to Teach Parents:
- Dry lips and mouth
- Sunken eyes
- Not urinating as often / dark urine
- Reduced tears when crying
- Decreased activity or lethargy
Bottom line: In a well-appearing 3-year-old with no fever, blood, or signs of dehydration, frequent small loose orange-yellow stools most likely represent toddler's diarrhea or a resolving viral gastroenteritis. If the child is thriving and there are no red flags, supportive care and dietary adjustment are appropriate. Persistent diarrhea beyond 2 weeks, weight loss, or any red flag should prompt medical evaluation including stool studies.
for gastroenteritis what is treatment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Treatment of Gastroenteritis
Core Principle
Gastroenteritis is usually self-limited - the goal is to prevent and treat dehydration, not to kill a bug. The vast majority of cases need NO antibiotics.
Step 1 - Assess Dehydration (the most important step)
| Degree | Signs |
|---|---|
| None/Minimal | Normal activity, moist mucous membranes, normal urine output, normal tears |
| Some (mild-moderate) | Decreased activity, dry mouth, sunken eyes, reduced tears, decreased urine output |
| Severe | Very decreased activity/lethargic, sunken eyes, no tears, markedly reduced urine, prolonged capillary refill, cold/mottled skin |
Step 2 - Rehydration (Treatment Backbone)
Oral Rehydration Therapy (ORT) - FIRST LINE for most patients
Use proper Oral Rehydration Solution (ORS) - NOT sports drinks, NOT plain water, NOT juices (too much sugar, worsen diarrhea)
| Solution | Sodium (mmol/L) | Osmolarity |
|---|---|---|
| WHO reduced-osmolarity ORS | 75 | 245 mOsm/L |
| Pedialyte | 45 | 250 mOsm/L |
| Apple juice | 0.4 | 730 mOsm/L ❌ |
| Gatorade | 20 | 350 mOsm/L (not ideal for infants) |
How to give ORT:
- If vomiting: start with 5 mL every 5 minutes, increase gradually as tolerated
- For mild-moderate dehydration: 25-50 mL/kg over 1-2 hours
- A Cochrane review shows ORT = IV rehydration in outcomes, with shorter hospital stays
IV Rehydration - reserved for:
- Severe dehydration / hemodynamic compromise
- Altered mental status preventing safe oral intake
- Persistent vomiting despite ondansetron
- Failure of ORT
Management Algorithm (pediatric):
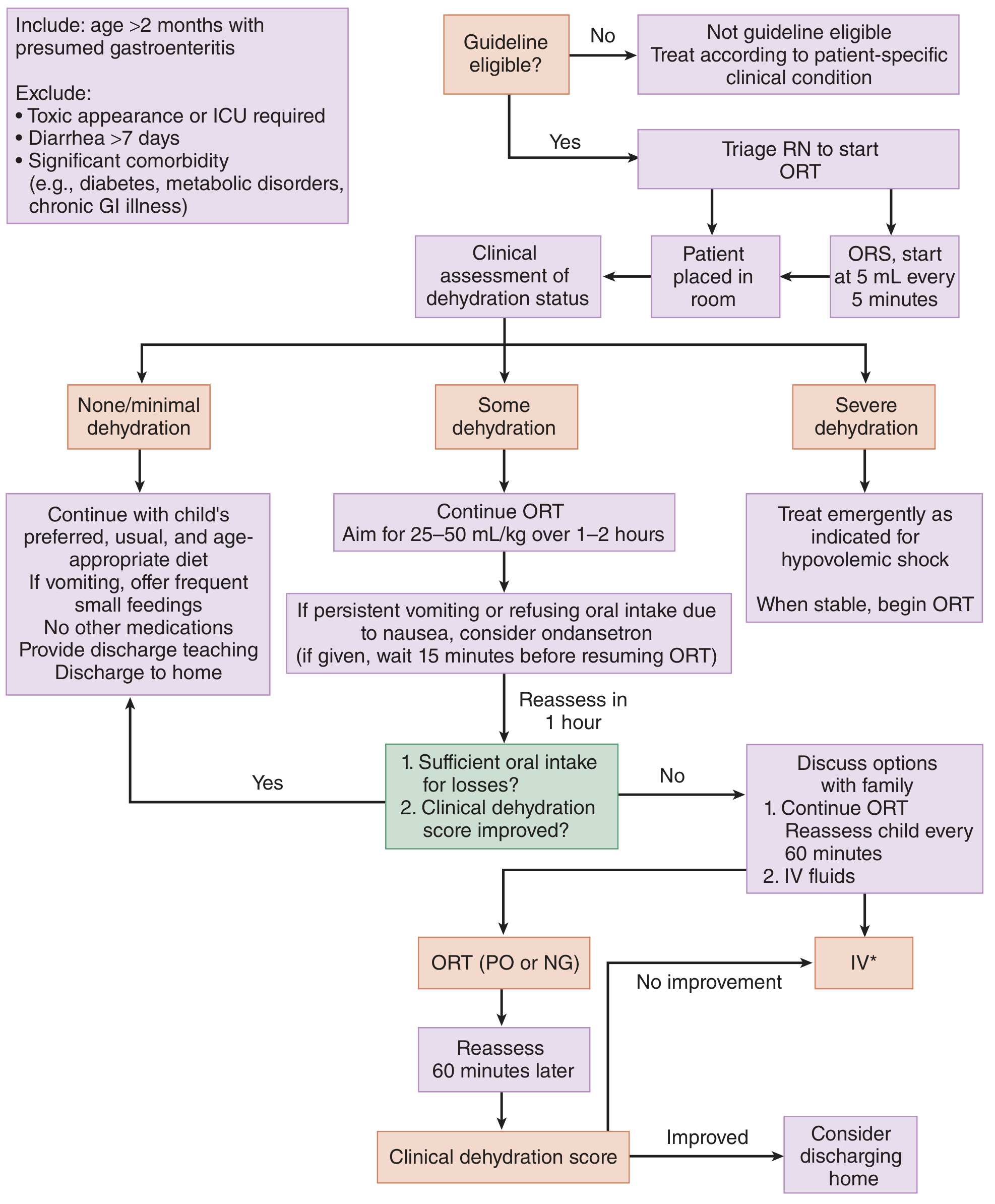
Tintinalli's Emergency Medicine, p. 889
Step 3 - Symptom Management
Vomiting - Antiemetics
- Ondansetron (first choice): 0.15 mg/kg up to 8 mg PO or IV - safe, effective, helps facilitate ORT
- Wait 15 minutes after giving before resuming ORT
- Reduces vomiting, avoids IV hydration in many patients
Diarrhea - Antimotility agents
- Loperamide (adults only, NOT children): reduces stool frequency; use cautiously
- Avoid in bloody diarrhea or suspected invasive/toxin-producing infection (e.g., E. coli O157:H7, C. difficile) - antimotility agents can increase toxin contact time and risk of HUS/TTP
- Bismuth subsalicylate (Pepto-Bismol): modest benefit in adults
Probiotics
- Lactobacillus rhamnosus GG and Saccharomyces boulardii - modest evidence, may shorten acute gastroenteritis by ~1 day
Zinc
- Recommended in children in developing countries (reduces duration and severity)
- WHO recommends 10-20 mg/day x 10-14 days in children with diarrhea
Step 4 - Diet / Feeding
- Do NOT fast the patient - early refeeding is recommended
- Return to normal diet as soon as tolerated - including dairy (no need to stop milk)
- Breastfeeding mothers: continue breastfeeding
- Avoid high-sugar foods/drinks and raw foods during illness
Step 5 - Antibiotics (only for specific situations)
NOT routinely indicated - even for most bacterial gastroenteritis (most is self-limiting)
| Pathogen | Antibiotic? | Drug of Choice |
|---|---|---|
| Viral (norovirus, rotavirus) | No | Supportive only |
| Salmonella (non-typhi) | Usually no (antibiotics prolong shedding) | Fluoroquinolone/azithromycin only in severe/immunocompromised |
| Campylobacter | Mild: No; Severe/early: Yes | Azithromycin 500 mg/day x 3 days |
| Shigella | Yes (shortens course, clears pathogen) | Ciprofloxacin 500 mg BD x 3 days OR azithromycin 500 mg/day x 3 days |
| E. coli O157:H7 (STEC) | NO - increases risk of HUS | Supportive only |
| C. difficile | Yes | Vancomycin 125 mg PO q6h x 10 days (first line) |
| Giardia | Yes | Metronidazole 250 mg TDS x 5-7 days |
| Typhoid (Salmonella typhi) | Yes | Fluoroquinolone or azithromycin x 7-14 days |
| Traveler's diarrhea (ETEC) | Yes if severe | Azithromycin or rifaximin |
Important: Antibiotics for E. coli O157:H7 are contraindicated - they increase Shiga toxin release and the risk of Hemolytic Uremic Syndrome (HUS).
- Rosen's Emergency Medicine, p. 1301-1307
When to Refer / Admit
- Severe dehydration or hemodynamic instability
- Unable to keep oral fluids down after ondansetron
- Bloody diarrhea with systemic signs (fever, prostration)
- Suspected C. difficile (recent antibiotics/hospitalization)
- Immunocompromised patient
- Extremes of age (very young infants, elderly)
- Diarrhea >2 weeks (consider parasites, IBD, other chronic causes)
Prevention / Infection Control
- Thorough handwashing with soap and water (most important - hand sanitizer alone is inadequate for norovirus and C. difficile)
- Rotavirus vaccine (2 oral doses in infants) - reduces rotavirus hospitalization by ~80%
- Food safety: avoid raw/undercooked poultry, unpasteurized milk, contaminated water
3 year old baby has 1 episode of vomiting followed by small frequent watery diarrhea ... fever 99.3
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I have all the information needed for a focused, practical clinical response. Let me compile it now.
Clinical Assessment: 3-Year-Old with Vomiting + Watery Diarrhea + Fever 99.3°F
Diagnosis: Viral Gastroenteritis (most likely)
99.3°F (37.4°C) = low-grade fever. Combined with:
- Single episode of vomiting (not bilious, not persistent)
- Small, frequent, watery diarrhea (no blood, no mucus described)
- Age 3 years
This is the textbook presentation of norovirus (now the #1 cause of acute gastroenteritis in children since rotavirus vaccine introduction) or rotavirus.
"Symptoms of norovirus include low-grade fever, anorexia, nausea, vomiting, diarrhea, and abdominal cramps. The disease typically runs its course in 1 to 5 days." - Swanson's Family Medicine Review
Step 1 - Assess Dehydration RIGHT NOW
This is the most critical assessment:
| Sign | Check in this Child |
|---|---|
| Activity level | Alert and playful? Or lethargic/irritable? |
| Mouth/lips | Moist or dry/sticky? |
| Eyes | Normal or sunken? |
| Tears | Present when crying? |
| Urine output | Last wet diaper/urination - when? Normal color? |
| Skin turgor | Normal or reduced? |
| Capillary refill | < 2 seconds = good |
With only 1 vomiting episode + early diarrhea + low-grade fever = likely MINIMAL or NO dehydration at this stage. This child can almost certainly be managed at home with ORT.
Treatment Plan
1. Oral Rehydration Therapy (ORT) - Start Immediately
Since there was only 1 episode of vomiting, start ORT now:
- Give Pedialyte / ORS (not plain water, not juice, not sports drinks, not soda)
- How to give:
- Start small - 5 mL (1 teaspoon) every 5 minutes
- If no vomiting after 30 minutes, increase to 10-15 mL every 5 minutes
- Target: ~1 oz (30 mL) per kg body weight per hour
- Replace ongoing losses: ~10 mL/kg per loose stool episode
- For a ~14 kg 3-year-old: aim for ~400-500 mL ORS over 4 hours if mildly dehydrated
"The mainstay of treatment is ORT. Fruit juices, carbonated beverages, and sports drinks are inappropriate - high osmolarity worsens stool losses." - Swanson's Family Medicine Review
2. Antiemetic - If Vomiting Continues
If child vomits again and is struggling to keep ORS down:
- Ondansetron (Zofran): 0.15 mg/kg as a single oral dose
- For ~14 kg child: approximately 2 mg PO (available as 4 mg ODT - can give half)
- Wait 15 minutes after giving before restarting ORS
- Do NOT use promethazine, metoclopramide, or prochlorperazine in children - risk of respiratory depression and extrapyramidal reactions
3. Fever Management
- 99.3°F (37.4°C) is LOW-GRADE - does not necessarily require medication
- If uncomfortable or fever rises:
- Paracetamol (acetaminophen): 15 mg/kg/dose every 4-6 hours as needed
- OR Ibuprofen: 10 mg/kg/dose every 6-8 hours (only if child is not dehydrated and tolerating fluids)
- Do NOT give aspirin in children
4. Feeding - Resume Early
- Do NOT starve the child - this prolongs diarrhea
- Resume normal age-appropriate diet as soon as tolerated
- Continue milk/formula - no need to stop dairy
- The old BRAT diet (banana, rice, applesauce, toast) is no longer recommended - too restrictive, not enough calories or fat
- Avoid high-sugar foods and juices during illness
5. Antidiarrheal Medications
- NOT recommended in children (loperamide, etc.) - safety concerns
- No antibiotics needed - this is viral
Monitoring at Home - Watch for These Red Flags
Return to doctor/emergency immediately if:
| Red Flag | Why Concerning |
|---|---|
| Vomiting turns bilious (green) | Possible bowel obstruction |
| Blood or mucus in stool | Invasive bacterial infection |
| Fever rises to >39°C (102.2°F) | Raises concern for bacterial cause |
| Child becomes lethargic/limp, not responding normally | Severe dehydration / sepsis |
| No urination for 6-8 hours / no tears when crying | Significant dehydration |
| Sunken eyes, dry mouth, not drinking | Moderate-severe dehydration |
| Vomiting becomes persistent (can't keep anything down) | Risk for rapid dehydration |
| Diarrhea >2 weeks | Consider parasites, other diagnosis |
| Severe abdominal pain | Rule out surgical cause |
- Tintinalli's Emergency Medicine, p. 889-890
Expected Course
- Viral gastroenteritis in a 3-year-old typically resolves in 1-5 days
- Vomiting usually stops within 24-48 hours
- Diarrhea may persist for 3-7 days even as child improves
- Appetite will be poor for a few days - this is normal
- Gradual return to normal stool frequency over 1 week
Bottom line for this child: Low-grade fever + 1 vomiting + watery diarrhea = very likely viral. Start ORS in small frequent sips now, watch for dehydration signs, resume normal diet early, give paracetamol only if uncomfortable. No antibiotics, no antidiarrheals. If child remains active, has tears when crying, and is urinating - they are adequately hydrated and can be managed safely at home.
This is a shared conversation. Sign in to Orris to start your own chat.