Rhinolith
Reading File
Searching the Web
rhinolith nasal calculus clinical features management
Finding Sources
Searching PubMed
rhinolith nasal calculus
Reading File
Reading File
Reading Web Page
https://www.kbb-forum.net/journal/text.php?lang=en&id=550
Here is a comprehensive overview of rhinolith:
Rhinolith (Nasal Calculus)
Definition
A rhinolith is a calcareous (mineral salt) concretion that forms within the nasal cavity around a central nidus. The term comes from the Greek rhinos (nose) + lithos (stone).
- K.J. Lee's Essential Otolaryngology: "calcareous concretions around intranasal foreign bodies within the nasal cavity, usually in the anterior nasal cavity"
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Vol. 2: "Rhinoliths consist of salts of calcium, magnesium phosphate and carbonate"
Pathogenesis
Nidus (the seed around which calcification occurs) can be:
- Exogenous - an inhaled or inserted foreign body (most common - beads, seeds, food material, tooth fragments). Foreign body introduction is most common in children aged 2-4 years.
- Endogenous - dried blood clot, inspissated mucus, desquamated epithelium, a deviated nasal bone fragment, or a displaced tooth root
Once the nidus lodges in the nasal cavity, it triggers a foreign body granulation reaction. Mineral salts from nasal secretions (calcium phosphate, calcium carbonate, magnesium phosphate) gradually deposit in concentric layers over months to years, enlarging the stone. A rhinolith may be present for decades - cases of stones indwelling for over 80 years have been reported.
Clinical Features
Rhinoliths can affect any age and either sex (slight female predominance in case series).
Symptoms (in approximate order of frequency):
- Unilateral nasal obstruction (most common)
- Unilateral purulent, foul-smelling nasal discharge (characteristic - the combination of unilateral purulence + malodor is the classic presentation)
- Oral malodor (halitosis)
- Facial pain / pressure
- Epistaxis (less common)
- Long-standing cases can cause hypoplasia of the inferior turbinate
Location: Most commonly found between the inferior turbinate and nasal septum. Right nasal cavity is slightly more commonly affected than left (around 60% vs 40% in case series).
Important: Many rhinoliths are asymptomatic for years, presenting only when large enough to cause obstruction or secondary infection.
Differential Diagnosis
Rhinolith enters the differential for nasal masses and unilateral nasal symptoms. It falls under the "Anatomic/Structural" category alongside:
- Nasal/sinus foreign body
- Mucocele
- Encephalocele
- Osteoma
- Benign and malignant neoplasms (inverted papilloma, SCC)
- Nasal polyps
- Chronic rhinosinusitis
- Granulomatous disease (Wegener's/GPA, sarcoidosis, TB)
Diagnosis
| Investigation | Finding |
|---|---|
| Anterior rhinoscopy | May reveal a grey-white, irregular mass, but turbinate hypertrophy or septal deviation can obscure it |
| Rigid nasal endoscopy | Best for direct visualization and localization |
| Plain X-ray (Waters' view) | Radio-opaque mass in nasal cavity |
| CT scan (gold standard) | Shows a hyperdense calcified mass; best for defining extent, relationship to turbinates/septum, and evaluating associated sinusitis. Helps exclude malignancy. |
CT is particularly important when there are associated sinus pathologies (mucosal thickening, retention cysts) or when the diagnosis is in doubt. About 50% of patients with rhinolith have concurrent sinus pathology; septal deviation is also frequently associated (~38%).
Management
Treatment is surgical removal.
- For most cases: endoscopic removal (functional endoscopic nasal surgery) under local, sedation, or general anesthesia
- For very large or anteriorly-placed stones: piecemeal fragmentation and extraction
- For anterior, small rhinoliths: simple forceps extraction may suffice in an outpatient setting
- The mother's kiss technique (used for simple foreign bodies in children) is generally not applicable for calcified rhinoliths
- Post-removal: nasal irrigation and antibiotics if secondary sinusitis is present
- The removed specimen should be sent for pathological examination to confirm nature and identify any nidus
Key Points to Remember
- Classic presentation: unilateral foul-smelling nasal discharge + obstruction
- Radio-opaque on plain X-ray; CT is the best imaging modality
- Can be present for years before diagnosis - high index of suspicion needed
- Always consider in children with a history of nasal foreign body insertion
- Differential from sinonasal tumors (including malignancy) is important - CT and histopathology clarify the diagnosis
- Excellent prognosis after removal
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 430; K.J. Lee's Essential Otolaryngology; KBB-Forum clinical series of 42 patients (2020)
Tympanosclerosis
Finding Sources
Searching PubMed
tympanosclerosis middle ear
Searching the Web
tympanosclerosis pathogenesis clinical features hearing loss management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent - I now have comprehensive textbook material and clinical images. Here is the full synthesis:
Tympanosclerosis
Definition
Tympanosclerosis is a post-inflammatory condition of the middle ear characterized by hyaline degeneration and calcification of the fibrous layer of the tympanic membrane (TM) and/or the submucosal connective tissue of the middle ear cleft. When restricted to the TM alone, it is more precisely called myringosclerosis.
Otoscopic Appearance
Myringosclerosis - the classic finding on otoscopy: chalky white, horseshoe-shaped or crescent-shaped plaques within the TM, usually in the anterior-inferior or posterior-inferior quadrants.
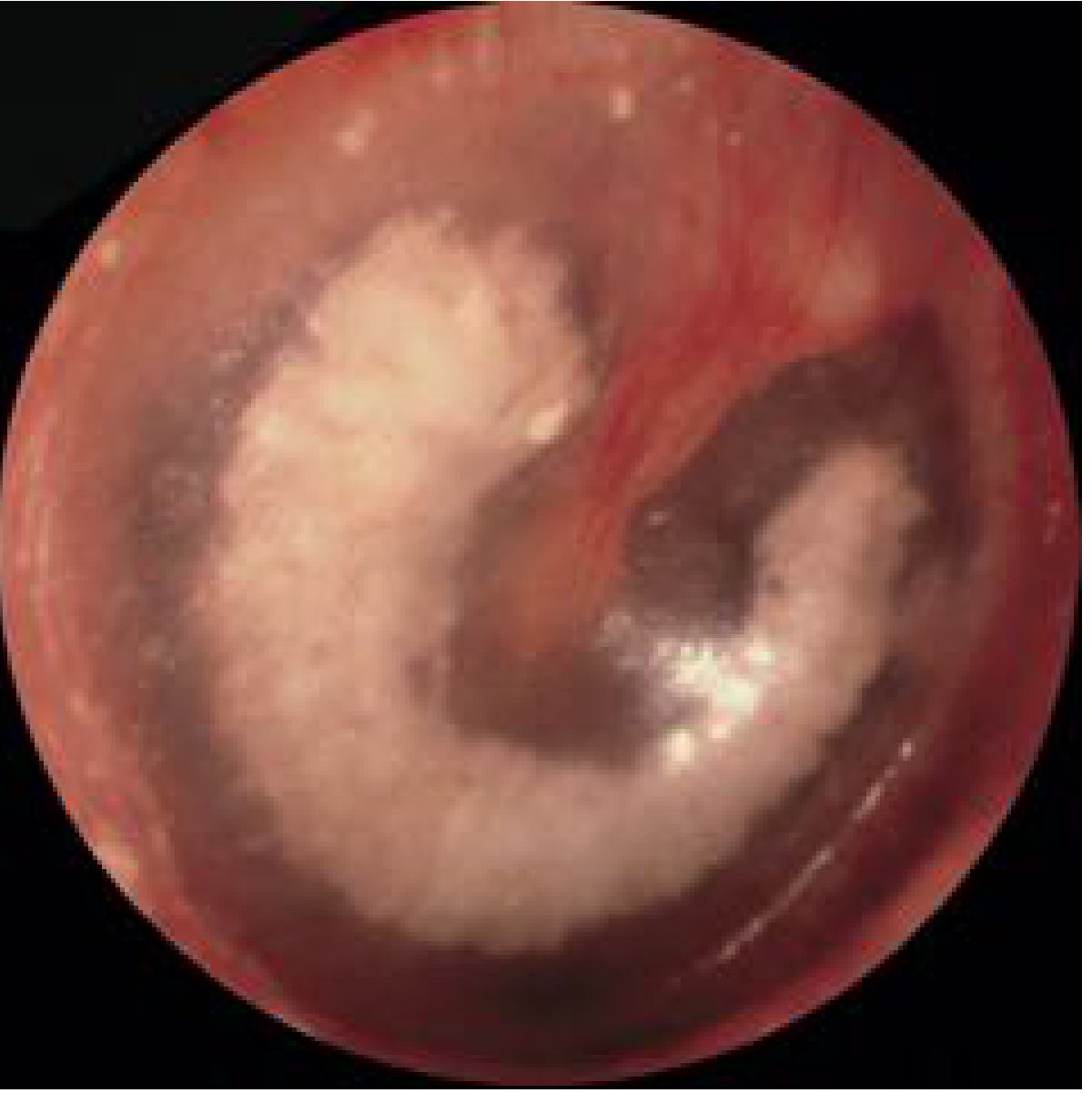
Fig. 140.18 - Myringosclerosis: semicircular crescent-shaped white plaque within the TM (Cummings Otolaryngology)
In advanced cases with middle ear involvement, white avascular chalky masses are seen attached to the promontory, malleus, and other middle ear structures:

Fig. 140.20 - Advanced tympanosclerosis with white avascular lesions on the promontory and malleus (Cummings Otolaryngology)
Epidemiology / Incidence
- Incidence in children with OME: ~10% (aged 4-15 years, average 4-year follow-up)
- In chronic otitis media generally: 9-43% across different series (~25% overall estimate)
- Strong association with tympanostomy (grommet) tube insertion: 59% of grommet ears developed tympanosclerosis vs. 13% of ears treated with myringotomy alone (Tos & Stangerup)
- Meta-analysis of 134 studies: 32% post-intubation tympanosclerosis vs. 10% in controls
Pathogenesis
Tympanosclerosis is a consequence of resolved otitis media (acute or with effusion) or middle ear trauma. The key steps are:
- Repeated middle ear inflammation triggers damage to the subepithelial connective tissue
- Collagen undergoes hyaline degeneration (acellular hyalinization of the lamina propria)
- Mineral salts (calcium phosphate, calcium carbonate) deposit in the degenerated tissue
- Osteoneogenesis can also occur within these lesions
- Microscopically: deposition occurs in concentric onion-ring layers, building up to several millimeters thick
Two proposed mechanisms (Hussl & Lim model):
- Direct collagen degeneration → calcified plaques
- Fibrous connective tissue degeneration → calcified plaques
Additional etiologic factors:
- Chlamydia pneumoniae has been identified as a possible infectious trigger
- Genetic predisposition - animal models (LP/J mouse; Enpp1asj mutant mice) support a genetic component
- Molecular pathways implicated in recent research: TNF-α, IL-6 (inflammatory cytokines), oxidative stress enzymes (CAT, iNOS), Wnt signaling, TGF-β1, osteopontin (bone remodeling)
Clinical Features
Distribution and Severity
| Location | Frequency | Clinical consequence |
|---|---|---|
| TM only (myringosclerosis) | Most common | Usually no significant hearing loss |
| Middle ear / attic | Less common | Ossicular fixation → conductive hearing loss |
| Stapes (oval window region) | Equal to attic in frequency | Significant CHL |
| Malleus/incus in attic | Equal to stapes fixation | Significant CHL |
| Both attic + stapes | Simultaneously in some cases | Severe CHL |
Hearing Loss
- Myringosclerosis alone - rarely causes significant hearing loss and usually requires no intervention
- Middle ear tympanosclerosis - can immobilize the malleus, incus, and/or stapes, causing moderate-to-severe conductive hearing loss
- Mixed hearing loss (conductive + sensorineural) can occur in long-standing middle ear disease
- Suspect ossicular fixation from tympanosclerosis when: history of chronic infections + CHL + tympanosclerosis visible on TM
Key Clinical Clue
Tympanosclerosis is typically irreversible. The TM form can occasionally resolve, but this is uncommon. The condition does not usually progress once the underlying inflammation has settled.
Investigations
| Test | Finding |
|---|---|
| Otoscopy / microscopy | Chalky white plaques on TM; malleus may fail to move on pneumatic otoscopy |
| Pure tone audiometry | Conductive hearing loss (air-bone gap), or normal if only TM involved |
| Tympanometry | Flat (type B) or reduced compliance (type As) curve |
| High-resolution CT temporal bone | Shows extent of ossicular fixation, attic involvement; helps surgical planning |
Management
Myringosclerosis (TM only)
- Observation - most cases require no treatment
- Hearing aid if mild CHL is present and surgery is declined or high-risk
Middle Ear Tympanosclerosis (Ossicular Fixation)
Surgical treatment is indicated for significant conductive hearing loss:
Principles (Tos technique):
- Wide atticotomy when disease is restricted to the attic
- Tympanosclerotic plaques are progressively removed from lateral, anterior, superior, and medial surfaces of malleus/incus
- Preserve the intact ossicular chain whenever possible
- Laser (otologic CO2 or KTP) is preferred to reduce mechanical trauma to the ossicles - thin shell of plaque is vaporized rather than dissected
For stapes fixation:
- Remove plaques without opening the vestibule; dissect posterior-to-anterior using the stapedius tendon for stability
- Stapedotomy - air-bone gap <20 dB achieved in ~70% in one series
- Stapedectomy - reserved for total stapes fixation; do not combine with TM repair (risk of labyrinthitis and profound SNHL)
- Attic disease addressed first, then stapes, in combined cases
For malleus/incus fixation:
- Option 1: Remove the bony fixation directly, preserve intact chain; Silastic sheet interposed between malleus head and attic wall
- Option 2: Remove incus and malleus head, interpose autograft/allograft between manubrium and stapes (TORP/PORP)
Outcomes:
- Excellent hearing results (ABG <20 dB) in ~79% with ossicular reconstruction in two-stage procedures (Smyth)
- Recurrence of tympanosclerosis post-surgery is reported but not universal
- Risk of cochlear damage is higher than in other middle ear surgery due to extensive dissection required
Key Points Summary
- Tympanosclerosis = hyaline degeneration + calcification of TM and/or middle ear, a sequela of otitis media or trauma
- Grommet insertion doubles the risk compared to myringotomy alone
- TM plaques alone rarely affect hearing - middle ear involvement causes CHL via ossicular fixation
- Stapes and malleus/incus in the attic are equally commonly affected
- Surgery is technically demanding; laser use reduces mechanical cochlear trauma
- Hearing aids are a valid alternative when surgery is high-risk or declined
Sources: Cummings Otolaryngology Head and Neck Surgery (§140, Figs. 140.18, 140.19, 140.20); Shambaugh Surgery of the Ear, p. 419; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 1045
Tracheoesophageal fistula
Finding Sources
Searching PubMed
tracheoesophageal fistula esophageal atresia
Searching the Web
tracheoesophageal fistula classification pathophysiology diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive material from multiple authoritative sources. Here is the full synthesis:
Tracheoesophageal Fistula (TEF)
Definition
A tracheoesophageal fistula is an abnormal communication between the trachea and the esophagus. It may be congenital (by far the most common, typically presenting in neonates) or acquired (from malignancy, trauma, or prolonged intubation).
Embryology (Congenital TEF)
TEF arises from a failure of separation of the primitive foregut into trachea and esophagus during weeks 4-6 of gestation. The most widely accepted hypothesis involves a defect in lateral septation of the foregut. The result may be esophageal atresia (EA) alone, TEF alone, or EA combined with TEF in various anatomic configurations.
Classification (Gross Classification)
Five types are described. Incidence figures come from Tintinalli's Emergency Medicine:
| Type | Description | Incidence |
|---|---|---|
| A | Isolated esophageal atresia (EA without TEF) - blind proximal pouch, no fistula | 7% |
| B | EA + proximal TEF - blind pouch communicates with trachea | 1% |
| C | EA + distal TEF - blind proximal pouch; distal esophagus communicates with trachea | 88% (most common) |
| D | EA + both proximal and distal TEFs | 1% |
| E | H-type TEF - fistula without EA, esophagus is intact | 3% |
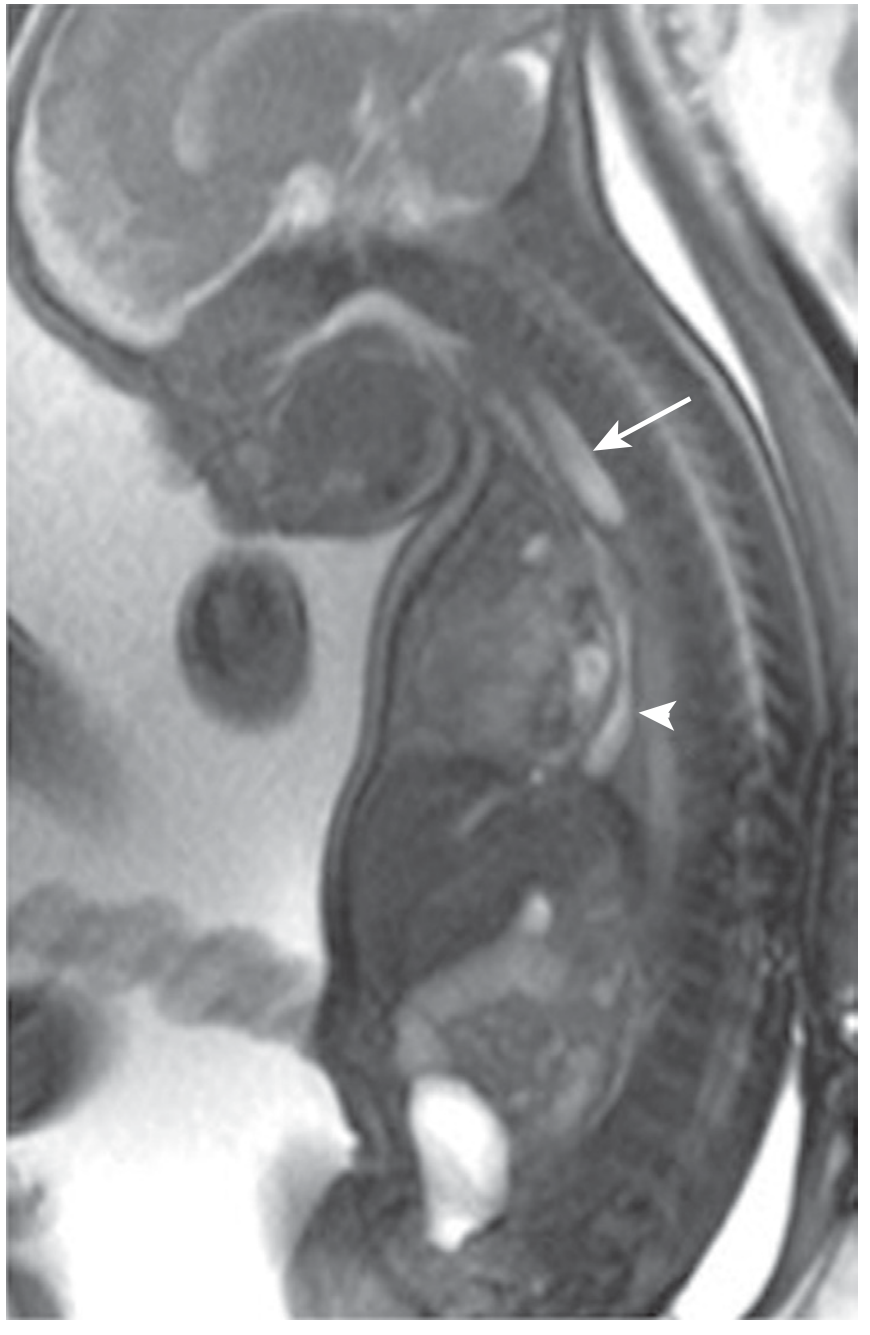
Fig. 43.9 - Sagittal T2-weighted fetal MRI showing proximal esophageal blind pouch (arrow) and long distal esophagus (arrowhead) in esophageal atresia (Sleisenger & Fordtran's)
Associated Anomalies - VACTERL
TEF is closely associated with the VACTERL association (~50-70% of EA-TEF patients have at least one associated anomaly):
- V - Vertebral anomalies (assessed by plain X-ray)
- A - Anal atresia (anorectal defects, ~8%)
- C - Cardiac defects (~38% - the most important predictor of survival; assess with echocardiography)
- TE - Tracheoesophageal fistula
- R - Renal anomalies (~15%)
- L - Limb anomalies / radial limb hypoplasia (~19% skeletal defects)
The aortic arch side (left vs. right) shown on echo also influences the surgical approach.
Clinical Presentation
Type C (EA + Distal TEF) - the typical neonate
- Excessive oral secretions / drooling from birth - the nursing staff often make the diagnosis at first feeding attempt
- Choking, coughing, and cyanosis at first feed
- Abdominal distension - air passes through the fistula into the stomach with each breath or cry
- Chemical pneumonitis - regurgitated gastric juice enters the trachea via the distal fistula
- Unable to pass NG tube into stomach - tube coils in the proximal blind pouch
- On CXR: gas-filled abdomen (confirms a distal TEF is present)
Type A (Isolated EA, no fistula)
- Regurgitation + scaphoid (gasless) abdomen - no pathway for air to enter bowel
- Saliva pools in the pouch
H-type TEF (Type E)
- Diagnosis often delayed to childhood or even adulthood
- Presents with recurrent aspiration pneumonia, chronic cough, bronchiectasis
- Symptoms relate to aspiration (not obstruction) since the esophagus is patent
- Diagnosed by esophagography ± bronchoscopy; methylene blue ingestion with bronchoscopic visualization of blue-stained fistula is a useful diagnostic trick for small, elusive H-type fistulas
Prenatal Diagnosis
- Polyhydramnios (impaired fetal swallowing - fetus cannot swallow amniotic fluid into the bowel)
- Absent stomach bubble on ultrasound (no fluid reaching the stomach)
- Fetal MRI (as shown above) can clearly demonstrate the proximal blind pouch
Postnatal Diagnosis
| Investigation | Finding |
|---|---|
| Clinical: NG tube insertion | Tube coils in upper pouch; cannot reach stomach |
| Chest X-ray | Coiled tube in pouch; gas in abdomen (if distal TEF present); gasless abdomen (if isolated EA) |
| Water-soluble contrast esophagogram | Confirms atresia, delineates proximal fistula, documents gap length |
| Bronchoscopy | Identifies fistula orifice in trachea; essential for H-type |
| Echocardiography | Mandatory - excludes cardiac defects; establishes aortic arch sidedness |
| Plain X-rays of spine, limbs | Assess vertebral and radial anomalies |
| Renal ultrasound | Renal anomalies |
Initial (Pre-operative) Management
- Position neonate with head elevated ≥30° to minimize aspiration
- Sump catheter in upper pouch on continuous suction - prevents aspiration of pooled saliva
- IV antibiotics + warmed electrolyte solution
- Avoid right upper limb IV if possible - it may interfere with surgical positioning
- Definitive repair is not a surgical emergency in the stable infant - repair can be planned 1-2 days after birth allowing thorough investigation
Special case: Premature neonate on ventilator
High ventilatory pressures can force air through the fistula into the stomach → abdominal distension → impaired lung expansion → worsened respiratory failure. Options include:
- Position endotracheal tube distal to the fistula
- Emergency gastrostomy to decompress the stomach
- Early surgical fistula ligation
Surgical Repair (Congenital EA-TEF)
Approach: Right posterolateral thoracotomy (extrapleural approach preferred) - the aortic arch on echocardiography determines approach side; a right-sided arch mandates a left thoracotomy.
Procedure:
- Fistula identified, ligated, and divided
- Esophageal ends mobilized
- End-to-end esophageal anastomosis performed (primary anastomosis)
- Short-gap (< 3 vertebral bodies): direct primary anastomosis
- Long-gap EA: options include:
- Bougienage (Foker procedure) or circular myotomy to lengthen upper pouch
- Magnetic compression anastomosis (magnamosis)
- Esophageal replacement using stomach (gastric pull-up), colon interposition, or jejunal graft if approximation impossible
Minimally invasive: Thoracoscopic repair is increasingly performed at specialized centers.
Long-term Complications (Post-repair)
| Complication | Frequency |
|---|---|
| Gastroesophageal reflux (GERD) without esophagitis | 57% |
| GERD with esophagitis | 40% |
| Barrett esophagus | 6.4% |
| Anastomotic stricture | 30-56% (requires dilatation) |
| Dysphagia in survivors to adulthood | ~50% |
| Fundoplication needed for GERD | 20-35% |
| Recurrent TEF | Uncommon but reported |
GERD is almost universal after EA-TEF repair due to abnormal esophageal motility and impaired acid clearance. Lifelong surveillance is recommended.
Acquired TEF
Causes
- Post-intubation (most common acquired cause) - ETT cuff pressure causes pressure necrosis of the posterior membranous trachea and anterior esophageal wall, forming a "party wall" fistula
- Malignancy - esophageal or lung cancer eroding between structures (poor prognosis: median survival ~10 weeks)
- Trauma - blunt or penetrating neck/chest trauma
- Iatrogenic - post-tracheotomy, post-esophageal surgery
- Infection - tuberculosis, actinomycosis (rare)
Surgical Repair (Benign Acquired TEF - Grillo Principles)
- Preoperative: Barium swallow to define anatomy; treat pulmonary sepsis; optimize nutrition; wean ventilator if possible
- Approach:
- Proximal TEF: anterior collar incision (may extend to sternotomy)
- Distal TEF: right posterolateral thoracotomy (4th/5th interspace)
- Technique:
- Segmental tracheal resection often required (especially for post-intubation TEF with circumferential cuff damage)
- Esophagus closed in two layers over an NG tube (inner layer - mucosa; outer layer - musculature) with interrupted non-absorbable sutures
- Trachea reanastomosed with interrupted absorbable sutures
- Pedicled muscle flap (infrahyoid strap muscle / sternohyoid) interposed between tracheal and esophageal suture lines - this is mandatory to prevent recurrence
- "Guardian suture" (chin-to-sternum) maintains 30° neck flexion post-op to reduce anastomotic tension
- Outcomes (benign TEF): 95% successful closure; 83% resume oral feeding; 72% tracheostomy-free
Malignant TEF - Palliation
- Surgery rarely appropriate (poor condition, poor prognosis)
- Self-expanding covered metal/plastic stents across the fistula (esophageal ± tracheal) - 80-100% success for sealing fistula
- Tracheal stent placed first (under bronchoscopy) before esophageal stent to prevent airway compression
- Stenting contraindicated at or above cricopharyngeus (pharyngeal foreign body sensation; unable to swallow)
- Peripheral bronchoesophageal fistulas: esophageal stent ± tracheobronchial stent
Summary Table
| Feature | Type C EA-TEF | H-type TEF | Acquired TEF |
|---|---|---|---|
| Age at diagnosis | Newborn | Infancy - adulthood | Any age |
| Key symptom | Drooling, choking at 1st feed | Recurrent aspiration pneumonia | Coughing on swallowing, aspiration |
| Abdomen on X-ray | Gas-filled | Normal | Normal |
| Best diagnostic test | CXR + NG tube | Esophagogram + bronchoscopy | Barium swallow + bronch/endoscopy |
| Treatment | Surgical repair | Surgical repair | Surgery (benign) / Stent (malignant) |
Sources: Schwartz's Principles of Surgery 11e (§39); Sleisenger & Fordtran's Gastrointestinal and Liver Disease (§43, Table 43.2); Tintinalli's Emergency Medicine; Current Surgical Therapy 14e (§ Operative Management, pp. 1026-1028)
This is a shared conversation. Sign in to Orris to start your own chat.