Difference between different types of fungal sinusitis
Reading File
Finding Sources
Searching PubMed
"fungal sinusitis" classification invasive
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough, well-illustrated answer. Here it is:
Fungal Sinusitis: Classification and Comparison
Fungal sinusitis (fungal rhinosinusitis, FRS) encompasses a wide spectrum of disorders - from benign colonization and hypersensitivity reactions to life-threatening tissue invasion. The fundamental division is invasive vs. non-invasive, defined histologically by whether fungal hyphae penetrate the mucosal basement membrane into underlying tissue.
Overview Classification
Fungal Sinusitis
├── NON-INVASIVE
│ ├── Fungal Ball (Mycetoma / Aspergilloma)
│ └── Allergic Fungal Rhinosinusitis (AFRS)
│
└── INVASIVE
├── Acute Invasive Fungal Sinusitis (AIFS)
├── Chronic Invasive Fungal Sinusitis (CIFS)
└── Granulomatous Invasive Fungal Sinusitis (GIFS)
1. Fungal Ball (Mycetoma / Aspergilloma)
Definition: Dense amalgamation of fungal hyphae within a sinus cavity, without tissue invasion and without an allergic/immune reaction.
| Feature | Detail |
|---|---|
| Immune status | Immunocompetent |
| Pathogen | Aspergillus spp. (most common); Candida |
| Sinus involved | Maxillary (most common) > Sphenoid > Ethmoid > Frontal |
| Presentation | Often asymptomatic (incidental finding); may cause chronic rhinosinusitis symptoms - cheek pressure/fullness, purulent nasal drainage if secondarily infected |
| Endoscopy | Gritty, chalky, clay-like or cheesy debris filling the sinus; the underlying mucosa is edematous but not invaded |
| Histology | Dense matted hyphae; NO tissue invasion, NO eosinophilic mucin, NO granulomas |
| CT | Partial/complete opacification of a single sinus; hyperdense foci (calcification) within opacified sinus; sinus walls often thickened and hyperostotic (reactive sclerosis); bone erosion may occur with remodeling |
| MRI | T1/T2 variable low-signal due to dehydration and calcification of fungal content |
| Treatment | Surgical removal (FESS) and sinus ventilation; no antifungals needed postoperatively in most cases |
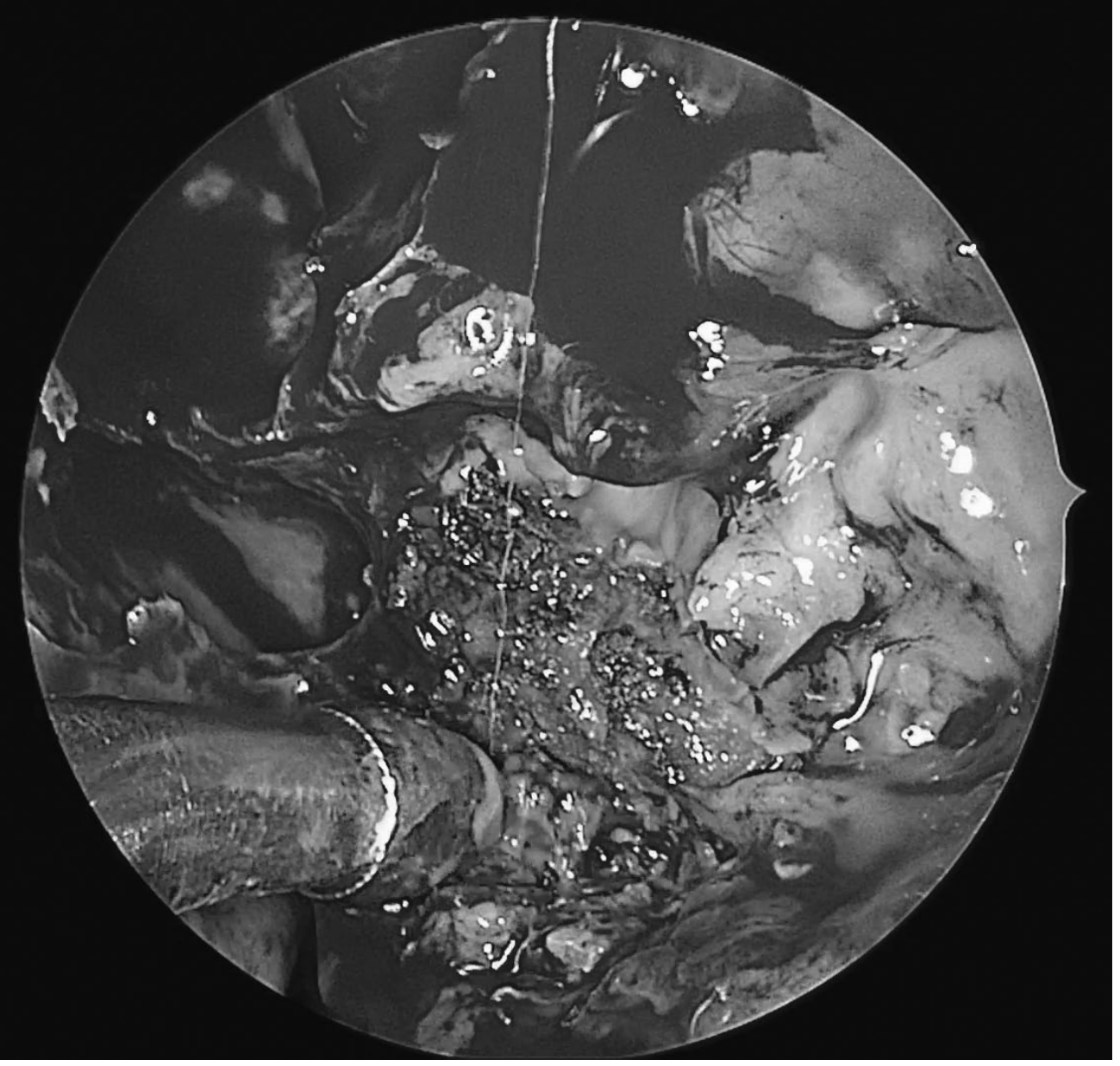
Endoscopic view: dense, chalky, discrete balls of fungal elements in the left maxillary sinus - KJ Lee's Essential Otolaryngology
2. Allergic Fungal Rhinosinusitis (AFRS)
Definition: Non-invasive fungal disease driven by a Type I IgE-mediated hypersensitivity response to fungal antigens, producing eosinophilic "allergic mucin" packed with degenerating eosinophils and Charcot-Leyden crystals. Analogous to allergic bronchopulmonary aspergillosis (ABPA) in the lung.
| Feature | Detail |
|---|---|
| Immune status | Immunocompetent, atopic individuals |
| Age/demographics | Young adults (mean age 21-33 years); warm, humid climates; lower socioeconomic status |
| Pathogens | Dematiaceous (dark-pigmented) fungi: Alternaria, Bipolaris, Curvularia, Cladosporium, Drechslera - and Aspergillus spp. |
| Presentation | Nasal congestion, thick dark nasal discharge, nasal polyps; responds to oral steroids but not antibiotics; may present with proptosis or telecanthus from bony erosion |
| Endoscopy | Gross nasal polyposis with thick, highly viscous mucin - classically described as "peanut butter" consistency; green or black casts |
| Histology | Eosinophilic mucin with Charcot-Leyden crystals, sheets of eosinophils, fungal hyphae on special stains (not visible on H&E); NO tissue invasion |
| Diagnostic criteria (Bent & Kuhn - all 5 major must be met) | 1. Type I hypersensitivity (skin test/IgE); 2. Nasal polyposis; 3. Characteristic CT findings; 4. Eosinophilic mucin without fungal invasion; 5. Positive fungal stain/culture of mucin |
| CT | Multi-sinus opacification, often bilateral; "double density" sign (central hyperattenuation of thick mucin surrounded by lower-attenuation mucosa); sinus expansion and bony erosion of sinus walls from mass effect (can mimic malignancy) |
| Treatment | Surgery (FESS) to remove mucin and polyps + oral corticosteroids (perioperative and maintenance); adjunct oral antifungals (itraconazole) may reduce recurrence; allergen immunotherapy |
Note: Despite being classified as non-invasive histologically, advanced AFRS with sinus expansion and bony erosion can produce intracranial/intraorbital "invasion" by mass effect that mimics malignancy on imaging.
3. Acute Invasive Fungal Sinusitis (AIFS)
Definition: Rapidly progressive, potentially fatal fungal infection with angioinvasion and/or perineural invasion by hyphae into tissue, occurring over days to weeks. The hallmark on histology is angioinvasion causing tissue necrosis.
| Feature | Detail |
|---|---|
| Immune status | Severely immunocompromised - neutropenia (<500/µL) or neutrophil dysfunction is the key risk |
| Risk groups | Hematologic malignancies (leukemia, BMT), chemotherapy-induced neutropenia, solid organ transplant, diabetic ketoacidosis (DKA), advanced HIV/AIDS, dialysis patients on deferoxamine |
| Pathogens | Zygomycetes (Mucorales) - Rhizopus (most common), Mucor, Rhizomucor, Absidia, Cunninghamella - irregular non-septate/pauci-septate hyphae branching at wide angles (90°); Aspergillus spp. - regular septate hyphae branching at acute angles (45°) |
| Pathomechanism (DKA) | Acidic environment activates Mucorales ketone reductase; abnormal transferrin binding frees iron; deferoxamine acts as siderophore for Rhizopus - all promote angioinvasion |
| Presentation | Fever, nasal obstruction, mucous drainage; rapidly progressing to facial/palatal eschar (black necrotic tissue), periorbital swelling, proptosis, cranial neuropathies, altered mental status |
| Endoscopy | Pale, gray, or black necrotic mucosa; loss of normal mucosal bleeding on instrumentation |
| Histology | Angioinvasion with vessel thrombosis, tissue necrosis, hyphae invading vessel walls; silver stain essential (H&E and Gram have high false-negative rates) |
| CT | Often subtle early; unilateral severe mucosal thickening; bony erosion is a late finding; soft tissue emphysema; periantral fat stranding; extrasinus extension |
| MRI | "Black turbinate sign" - absence of mucosal enhancement on post-contrast T1 (non-enhancing devitalized tissue due to angioinvasion); MRI superior for detecting soft-tissue extension, orbital/intracranial involvement |
| Prognosis | 50% overall mortality; worse with intracranial extension, facial/palatal involvement, severe neutropenia, CRP ≥5.50 mg/dL, renal/liver failure |
| Treatment | Three pillars: (1) Reverse immunosuppression (control DKA, reduce steroids/immunosuppressants); (2) Wide surgical debridement to bleeding margins; (3) IV antifungals - Liposomal amphotericin B (drug of choice, especially for mucormycosis); IV voriconazole for Aspergillus; isavuconazole is an alternative |
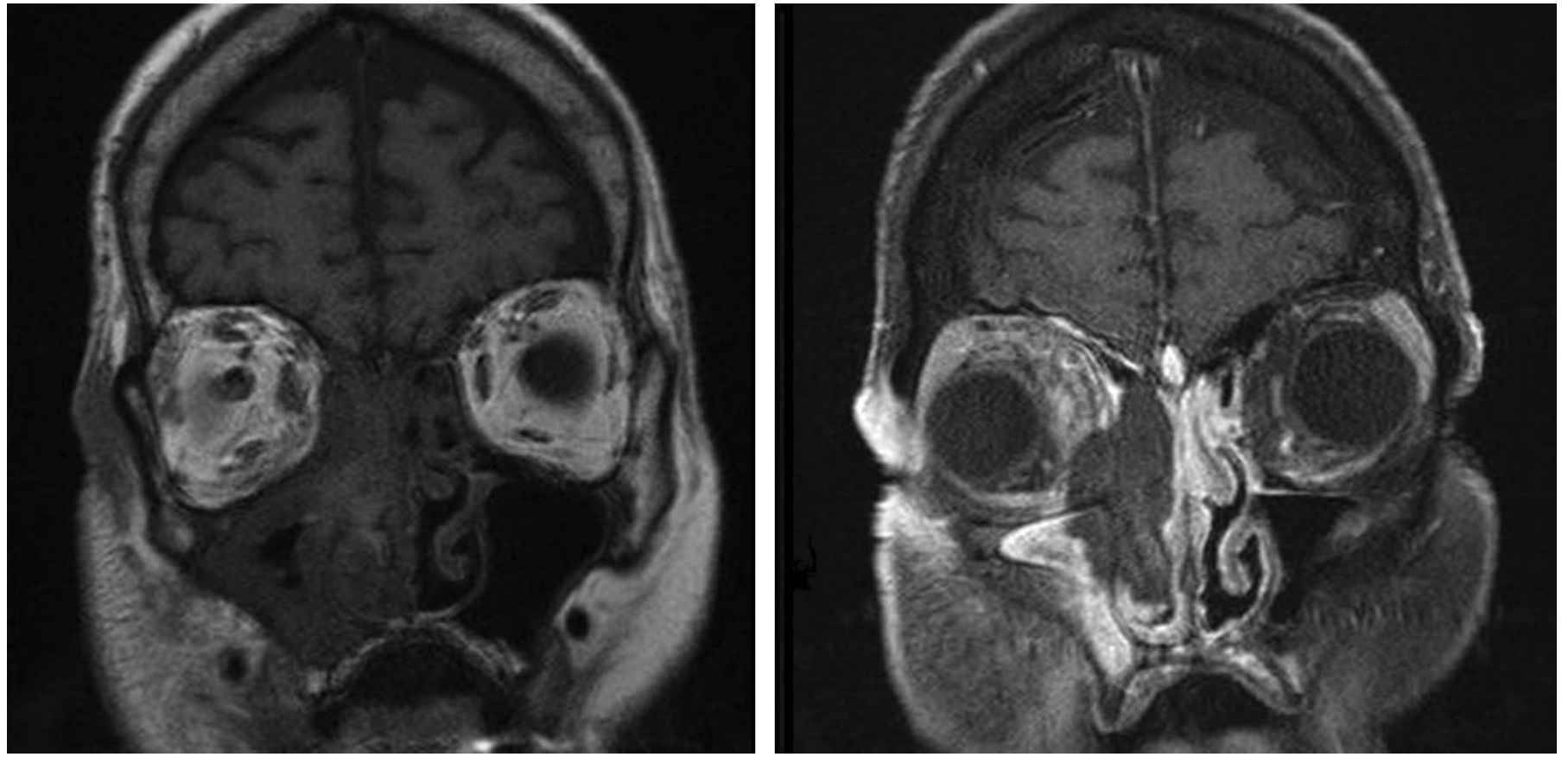
"Black turbinate sign" on post-contrast T1 MRI (right panel): the middle turbinate mucosa fails to enhance due to fungal angioinvasion - KJ Lee's Essential Otolaryngology
4. Chronic Invasive Fungal Sinusitis (CIFS)
Definition: An indolent form of invasive fungal sinusitis lasting >4 weeks, considered a less fulminant variant of AIFS.
| Feature | Detail |
|---|---|
| Immune status | Immunocompetent or mildly immunocompromised (diabetes mellitus, low-dose glucocorticoids) |
| Age | Older patients than AFRS |
| Pathogens | Aspergillus spp. (hyaline molds) and dematiaceous molds more common than Mucorales |
| Presentation | Months of non-specific CRS symptoms (maxillary pressure, nasal drainage) before a complication appears: proptosis/visual changes (orbital invasion), cranial neuropathies, pre-antral cellulitis |
| Histology | Dense hyphae (similar to fungal ball) plus tissue invasion with necrosis; distinguished from AIFS by time course and immune status |
| CT/MRI | Affected sinus with mass lesion and mucosal thickening; bony erosion and extrasinus involvement common; T1/T2 iso- or hypointense signals relative to muscle |
| Treatment | Same three pillars as AIFS: reverse immunosuppression + surgical debridement + prolonged antifungal therapy; long-term surveillance required |
5. Granulomatous Invasive Fungal Sinusitis (GIFS)
Definition: A rare, distinct form of chronic invasive FRS defined by non-caseating granuloma formation with Langhans-type giant cells, dense background fibrosis, and vasculitis.
| Feature | Detail |
|---|---|
| Immune status | Immunocompetent (predominantly) - may occur in immunodeficient patients |
| Geography | Almost exclusively North Africa (Sudan), Middle East, South Asia (India, Pakistan, Saudi Arabia); rare in the West |
| Pathogens | Aspergillus flavus (most common), A. fumigatus |
| Presentation | Unilateral proptosis is the classic presentation (rather than CRS symptoms); indolent course means disease is often advanced at diagnosis; frequently mistaken for a tumor |
| Histology | Non-caseating granulomas with Langhans-type multinucleated giant cells; dense background fibrosis; vasculitis; fungal hyphae within granulomas |
| CT | Large, expansive hyperdense mass with homogenous contrast enhancement; lacks the dual-density secretions seen in fungal balls; bony erosion and extrasinus involvement common |
| MRI | T1/T2 hypointensity; foci of parenchymal enhancement (cerebritis) adjacent to the solid lesion |
| Treatment | Surgical resection (conservative, orbit-sparing where possible given responsiveness to therapy) + prolonged antifungal: oral itraconazole or voriconazole for limited disease; oral voriconazole for advanced/intracranial disease; amphotericin B is not recommended first-line (caused by Aspergillus, not Mucorales) |
Side-by-Side Comparison Table
| Feature | Fungal Ball | AFRS | AIFS | CIFS | GIFS |
|---|---|---|---|---|---|
| Invasiveness | No | No | Yes | Yes | Yes |
| Immune status | Intact | Atopic, intact | Severely immunocompromised | Intact/mildly compromised | Intact |
| Course | Chronic/indolent | Chronic | Acute (<4 wks) | Chronic (>4 wks) | Chronic/indolent |
| Key pathogen | Aspergillus | Dematiaceous fungi | Rhizopus/Mucor; Aspergillus | Aspergillus; dematiaceous | A. flavus |
| Histology hallmark | Dense hyphae, no invasion | Eosinophilic mucin, Charcot-Leyden crystals, no invasion | Angioinvasion + necrosis | Hyphae + tissue necrosis | Non-caseating granulomas, Langhans giant cells |
| Allergic mucin | No | Yes | No | No | No |
| CT hallmark | Hyperdense foci, hyperostosis, single sinus | Double density, multi-sinus expansion | Subtle mucosal thickening → bone erosion | Mass lesion, bony erosion | Expansile hyperdense mass, homogenous enhancement |
| MRI hallmark | Low T1/T2 | Double density | Black turbinate sign | Iso/hypointense | T1/T2 hypointense, cerebritis foci |
| Mortality | Nil | Nil | ~50% | High if undiagnosed | Significant |
| Surgery | FESS (curative) | FESS + debridement | Wide aggressive debridement | Debridement | Conservative resection |
| Antifungals | Usually NOT needed | Adjunct (oral itraconazole) | IV Lip-AmB (mucor) / Voriconazole (Aspergillus) | Prolonged IV/oral | Voriconazole (NOT AmB) |
| Steroids | No | Yes (systemic) | No (harmful) | No | No |
Key Distinguishing Points
-
Immune status is the single most important differentiator: AIFS demands severe immunocompromise; fungal ball and AFRS occur in fully intact hosts; GIFS is almost exclusively in immunocompetent patients in specific geographies.
-
Time course: "Acute" (days-weeks) = AIFS. "Chronic" (months) = CIFS or GIFS. Non-invasive forms are always chronic.
-
The black turbinate sign on MRI is pathognomonic for AIFS - absence of enhancement indicates angioinvasion and mucosal devascularization.
-
AFRS vs. fungal ball: Both non-invasive in intact hosts, but AFRS is an allergic/immune-driven response (needs atopy, eosinophilic mucin, IgE) while fungal ball is a simple saprophytic colonization without immune activation.
-
GIFS vs. CIFS: GIFS is differentiated by geography (Africa/Asia), A. flavus as pathogen, and the non-caseating granulomas on histology. Both are chronic and invasive.
-
Antifungal choice matters: Liposomal amphotericin B for Mucorales (AIFS in DKA); voriconazole for Aspergillus (AIFS, CIFS); voriconazole/itraconazole for GIFS (amphotericin is NOT recommended for Aspergillus flavus-driven GIFS).
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1; KJ Lee's Essential Otolaryngology, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.