Hyperthyroidism management
Reading File
Finding Sources
Searching PubMed
"hyperthyroidism"[MeSH Terms] AND "management"[MeSH Terms]
Searching the Web
hyperthyroidism management guidelines 2025 ATA
Reading File
Reading File
Reading File
Searching PubMed
"hyperthyroidism" AND "antithyroid" AND "treatment"
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive, multi-textbook coverage. Let me compile the full answer.
Hyperthyroidism: Management
Diagnostic Workup - Algorithm
The flowchart below (from Current Surgical Therapy, 14e) shows the diagnostic pathway from suspected thyrotoxicosis to etiology:
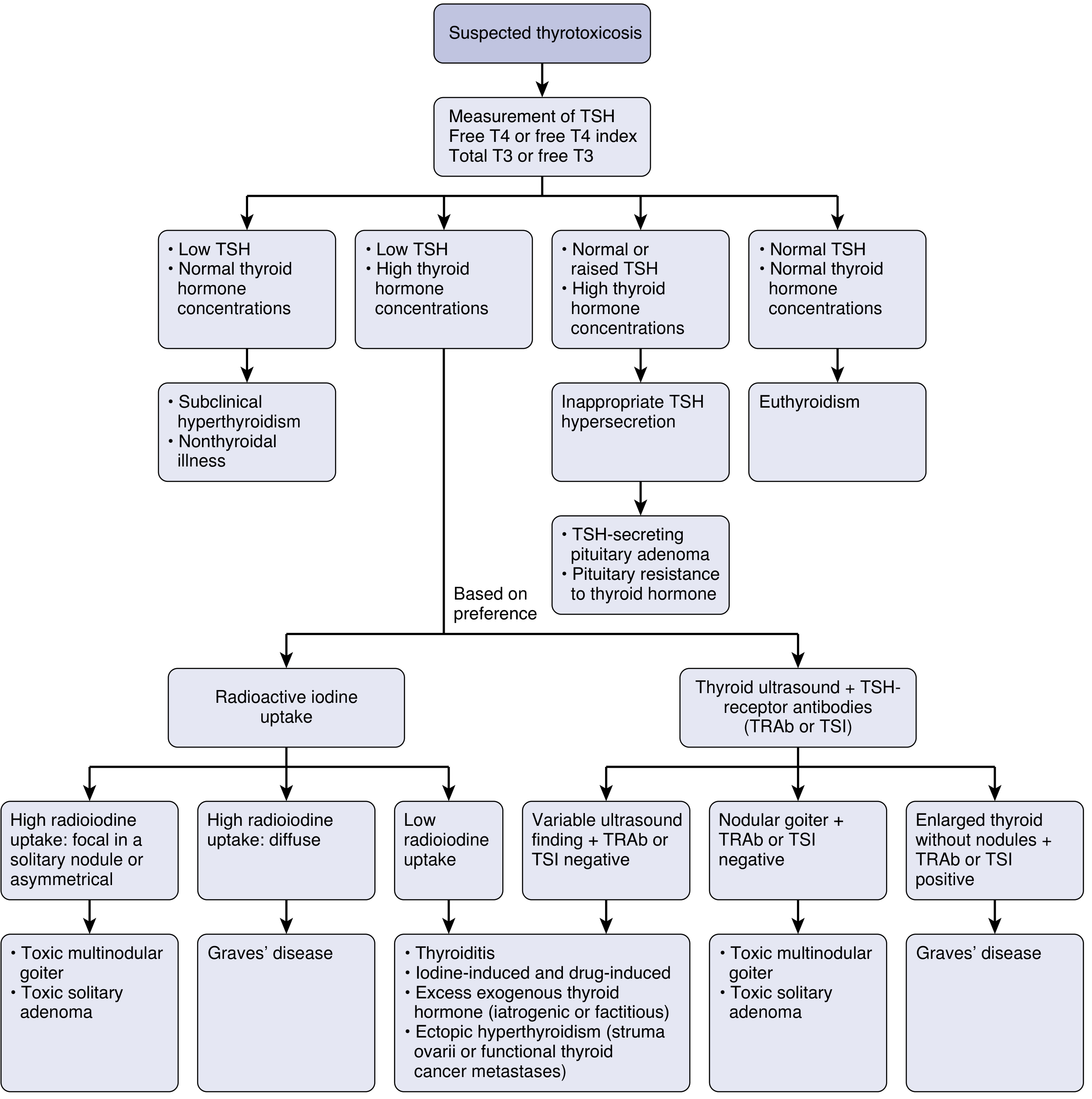
Start with: TSH + Free T4 (or FT4 index) + Total/Free T3
- Low TSH + elevated thyroid hormones → confirmed overt hyperthyroidism
- Low TSH + normal thyroid hormones → subclinical hyperthyroidism or non-thyroidal illness
- Normal/elevated TSH + elevated hormones → inappropriate TSH hypersecretion (TSH-secreting pituitary adenoma / pituitary resistance)
Then differentiate etiology with radioiodine uptake (RAIU) or thyroid ultrasound + TRAb/TSI antibodies.
Step 1 - Symptomatic Control (All Patients)
Beta-adrenergic blockade is the first step in any symptomatic patient, especially the elderly or those with HR >90 bpm or cardiovascular disease.
| Drug | Dose | Notes |
|---|---|---|
| Propranolol (non-selective) | 10-40 mg 3-4x/day | Also blocks peripheral T4→T3 conversion |
| Atenolol (beta-1 selective) | 25-100 mg 1-2x/day | Preferred in mild asthma (use cautiously) |
| Metoprolol (beta-1 selective) | 25-50 mg 2-3x/day | Alternative |
-
Contraindications: asthma (relative), congestive heart failure, bradyarrhythmias, Raynaud's disease
-
Alternative: calcium channel blockers (rate control) when beta-blockers are not tolerated
-
Current Surgical Therapy, 14e, p. 890; Lippincott Illustrated Reviews: Pharmacology, p. 785
Step 2 - Definitive Treatment: Three Modalities
All three modalities (antithyroid drugs, radioiodine, surgery) are similarly effective at reducing thyroid hormone levels and improving quality of life. Choice depends on etiology, patient factors, and clinician preference.
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Vol 1, p. 772
2A. Antithyroid Drugs (Thionamides)
Mechanism: Inhibit thyroid peroxidase-mediated iodination of tyrosyl groups and coupling of iodotyrosines to form T3/T4. PTU additionally blocks peripheral T4→T3 conversion. Note: no effect on pre-formed thyroglobulin stores - clinical effect is delayed until those stores are depleted.
| Drug | Preferred Use | Key Points |
|---|---|---|
| Methimazole (MMI) | First-line for most adults | Once-daily dosing (longer half-life), lower side-effect burden |
| Propylthiouracil (PTU) | First trimester of pregnancy; thyroid storm | Black box warning for hepatotoxicity (fulminant hepatic failure); FDA warning added 2010 |
| Carbimazole | Available outside USA | Prodrug - completely converted to MMI |
Duration: 12-18 months for Graves' disease (remission rates do NOT improve beyond 18 months)
Remission rate: ~50-80% while on therapy; relapse 20-30% over 3-5 years after stopping
Tapering/discontinuation: Only if TRAb levels have normalized
Major adverse effects:
- Agranulocytosis - stop drug immediately if fever/sore throat, check CBC; diagnose if ANC <500/uL
- Hepatotoxicity - cholestatic (MMI) vs. hepatocellular/fulminant liver failure (PTU)
- Vasculitis, rash, pruritus, arthralgia
European vs. US practice: Europe favors antithyroid medications (especially <40 years), reserving surgery for relapse. In the USA, RAI is widely used as first-line.
- Current Surgical Therapy, 14e, p. 890; Lippincott Illustrated Reviews: Pharmacology, p. 784
2B. Radioactive Iodine (RAI, ¹³¹I)
- ¹³¹I is selectively taken up by thyroid follicular cells, destroying thyroid tissue
- Used for Graves' disease and toxic multinodular goiter
- Most patients develop hypothyroidism post-RAI and require long-term levothyroxine replacement
- Contraindicated before achieving a sustained euthyroid state (may precipitate thyroid storm)
- Preoperative use of iodides: Lugol's solution or potassium iodide is used before surgery but not routinely before RAI in all patients
Considerations:
-
Associated with increased cardiovascular mortality risk - though this is likely from underlying thyrotoxicosis, not RAI itself; RAI-induced hypothyroidism may be protective
-
Concerns about secondary malignancy make it less preferred in children and young adults
-
Contraindicated in: active Graves' orbitopathy (worsens eye disease), pregnancy, breastfeeding
-
Scott-Brown's, Vol 1, p. 772; Current Surgical Therapy, 14e, p. 893
2C. Surgery (Thyroidectomy)
Indications for thyroidectomy in Graves' disease:
- Women planning pregnancy within 6 months
- Large thyroid nodules (>4 cm), compressive goiter symptoms, suspected/known malignancy
- Concurrent primary hyperparathyroidism needing parathyroidectomy
- Moderate-to-severe Graves' orbitopathy
- Persistent disease after prior antithyroid drug or RAI failure
- Children/young adults (avoid RAI malignancy risk)
Type of surgery: Total or near-total thyroidectomy for Graves' disease and toxic multinodular goiter; thyroid lobectomy for toxic adenoma.
Outcomes: Total thyroidectomy has lowest persistent/recurrent hyperthyroidism rate:
- Total thyroidectomy: 0.3% recurrence
- Single-dose RAI: 21% recurrence
- Subtotal thyroidectomy: 10% recurrence
Preoperative preparation (to minimize anesthetic risk and thyroid storm):
- Render patient euthyroid with thionamides + beta-blockade
- Add potassium iodide (50 mg/drop, 1-2 drops TID) or Lugol's solution (2-3 drops TID) 7-10 days before surgery - reduces thyroid vascularity and hormone release (Wolff-Chaikoff effect)
- High-volume, experienced surgeon essential (Graves' disease carries highest risk of hypoparathyroidism and recurrent laryngeal nerve injury of all thyroid operations)
Relative contraindications: Severe cardiopulmonary disease, advanced cancer, shortened life expectancy.
- Current Surgical Therapy, 14e, p. 892-893
Step 3 - Special Situations
Graves' Orbitopathy
- RAI is relatively contraindicated (worsens eye disease)
- Surgery is preferred for moderate-severe orbitopathy
- Teprotumumab (IGF-1R inhibitor) is now approved for active thyroid eye disease, with demonstrated efficacy and durability
Pregnancy
- First trimester: PTU preferred (MMI is teratogenic - risk of aplasia cutis, choanal/esophageal atresia)
- Second/third trimester: Switch to MMI (PTU's higher hepatotoxicity risk outweighs teratogenic risk by then)
- Thyroid storm in pregnancy: beta-blockers, thioamides, iodine, iodinated contrast, corticosteroids; avoid aspirin (displaces thyroid hormone from binding proteins)
Subclinical Hyperthyroidism
- TSH low + normal FT4/FT3
- Treatment is debated; consider treating if TSH persistently <0.1 mU/L, patient >65 years, or with cardiac risk factors/osteoporosis
Drug-Induced Hyperthyroidism
- Amiodarone-Induced Thyrotoxicosis Type 1 (AIT-1) - increased thyroid hormone synthesis: stop amiodarone + thionamides
- AIT-2 - destructive thyroiditis: corticosteroids; amiodarone stopping is case-by-case
- Immune checkpoint inhibitors: dose depends on type of immune reaction
- Subacute thyroiditis: NSAIDs first-line; corticosteroids for refractory; beta-blockers for symptoms
Thyroid Storm (Thyrotoxic Crisis)
A life-threatening emergency requiring ICU admission. Same drugs as for hyperthyroidism but at higher doses and more frequently.
Treatment sequence (order matters):
- PTU - first (also blocks T4→T3 conversion)
- Iodide (Lugol's or SSKI) - 1 hour AFTER PTU (giving iodide before thionamide provides substrate for more hormone synthesis)
- Beta-blockers (propranolol/metoprolol/atenolol) - blunt sympathetic surges
- Corticosteroids (hydrocortisone or dexamethasone) - reduce T4→T3 conversion, treat possible adrenal insufficiency
- Fluid resuscitation + antipyretics (acetaminophen preferred; avoid aspirin)
- Treat the precipitating cause (infection, MI, PE, stroke)
- Cholestyramine - for severe/refractory cases (interrupts enterohepatic recirculation of thyroid hormone)
- Plasmapheresis - last resort to remove circulating thyroid hormone
- ECMO - for severe storm with rapid cardiovascular deterioration
- Rosen's Emergency Medicine, p. 211; Lippincott Illustrated Reviews: Pharmacology, p. 785; Berek & Novak's Gynecology, p. 3201
Iodide Mechanism: Wolff-Chaikoff Effect
A pharmacological dose of iodide transiently inhibits iodination of tyrosines (lasts only days), but more importantly inhibits hormone release from thyroglobulin - hence its utility preoperatively and in thyroid storm. Iodide also decreases thyroid vascularity (useful before surgery). Not suitable for long-term therapy due to escape from Wolff-Chaikoff effect.
Treatment Summary by Etiology
| Etiology | First-Line | Notes |
|---|---|---|
| Graves' disease (USA) | RAI or MMI | RAI preferred in older adults; MMI preferred if planning pregnancy soon |
| Graves' disease (Europe) | MMI (if <40y) | Surgery if relapse |
| Graves' orbitopathy (moderate-severe) | Surgery + teprotumumab | RAI contraindicated |
| Toxic multinodular goiter | RAI or surgery | Thionamides used to achieve euthyroid pre-RAI/surgery |
| Toxic adenoma | RAI or lobectomy | Thionamides for temporizing |
| Subacute thyroiditis | NSAIDs ± beta-blockers | Self-limiting; no thionamides needed |
| Thyroid storm | PTU → iodide → beta-blockers → steroids | ICU; treat precipitant |
| Pregnancy (1st trimester) | PTU | Switch to MMI in 2nd-3rd trimester |
Recent Evidence (PubMed 2025)
A 2025 network meta-analysis (PMID: 40891035, Thyroid) examined mortality risks across all three treatment modalities (antithyroid drugs, RAI, surgery) - this represents the most current comparative evidence and may inform treatment selection. Watch for updates to formal ATA hyperthyroidism guidelines (the 2025 ATA publication was specific to differentiated thyroid cancer, not hyperthyroidism per se; the 2016 ATA Hyperthyroidism Guidelines remain the operative reference for Graves' disease and hyperthyroid management).
This is a shared conversation. Sign in to Orris to start your own chat.