Detail information about puerperal disorder for 10 mark and with good presentation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compile a detailed, well-structured 10-mark answer on puerperal disorders.
Puerperal Disorders — Comprehensive 10-Mark Answer
Definition
The puerperium is the period following delivery, lasting approximately 6 weeks, during which the maternal reproductive system returns to its pre-pregnant state. Puerperal disorders are a group of pathological conditions that arise during this period, encompassing infectious, hemorrhagic, thromboembolic, and psychiatric complications.
Classification of Puerperal Disorders
PUERPERAL DISORDERS
│
├── 1. Puerperal Pyrexia / Sepsis
├── 2. Puerperal Hemorrhage
│ ├── Primary (< 24 hours)
│ └── Secondary (24 hrs – 6 weeks)
├── 3. Puerperal Endometritis
├── 4. Wound & Perineal Infections
├── 5. Puerperal Mastitis & Breast Abscess
├── 6. Septic Pelvic Thrombophlebitis
└── 7. Puerperal Psychiatric Disorders
├── Baby Blues
├── Postpartum Depression
└── Postpartum Psychosis
1. Puerperal Pyrexia and Sepsis
Definition: Fever of 38°C (100.4°F) or higher occurring on any two of the first 10 days postpartum (excluding the first 24 hours), or any fever ≥38.5°C in the first 24 hours.
Causative Organism: Streptococcus pyogenes (Group A Streptococcus) is the classic agent of puerperal sepsis. Women typically present with fever, abdominal pain, and hypotension without tachycardia or leukocytosis — a deceptively mild early picture. Maternal mortality is highest when infection occurs within 4 days of delivery.
- Incidence: 6–80 cases per 100,000 live births
- Case-fatality rate: ~3.5%
- Transmission: may be nosocomial or from household contacts with streptococcal pharyngitis
(Goldman-Cecil Medicine)
2. Puerperal Endometritis
Epidemiology
| Mode of Delivery | Without Prophylaxis | With Prophylaxis |
|---|---|---|
| Scheduled C-section (no labor) | 5–15% | < 5% |
| C-section after prolonged labor + ruptured membranes | 30–35% | ~10% |
Pathogenesis
Endometritis is a polymicrobial infection caused by normal vaginal flora — aerobes and anaerobes — that ascend to the upper genital tract during labor, vaginal examinations, and surgery. Key pathogens include:
- GBS (Group B Streptococcus)
- Anaerobic gram-positive cocci (Peptostreptococcus spp.)
- Aerobic gram-negative bacilli (E. coli, K. pneumoniae, Proteus)
- Anaerobic gram-negative bacilli (Bacteroides, Prevotella)
- Chlamydia trachomatis (late-onset endometritis)
Risk Factors
Intraamniotic infection (chorioamnionitis), cesarean delivery (greatest single risk factor), young age, prolonged labor, prolonged ruptured membranes, multiple vaginal examinations, internal monitoring, pre-existing GBS/gonorrhea/BV.
Clinical Features
- Fever ≥38°C within 36 hours of delivery
- Malaise, tachycardia
- Uterine tenderness, lower abdominal pain
- Malodorous lochia
- ± Tender inflammatory mass (broad ligament, cul-de-sac)
Treatment
First-line: Clindamycin 900 mg IV q8h + Gentamicin 5 mg/kg IV q24h
- ~90–95% of patients defervesce within 48–72 hours
- IV antibiotics discontinued once afebrile and asymptomatic for ~24 hours
- Extended oral antibiotic course after discharge is not routinely necessary
Failure to respond → suspect: resistant organism (Enterococcus → add ampicillin), wound abscess, pelvic abscess, or septic pelvic thrombophlebitis.
(Creasy & Resnik's Maternal-Fetal Medicine)
3. Postpartum Hemorrhage (PPH)
Definition: Blood loss >500 mL after vaginal delivery, or >1000 mL after cesarean delivery.
Classification
| Type | Timing |
|---|---|
| Primary PPH | Within first 24 hours |
| Secondary PPH | 24 hours to 6 weeks postpartum |
Because of maternal plasma volume expansion during pregnancy, the patient may not show signs of shock until >1500 mL of blood is lost.
The "Four Ts" — Causes of Primary PPH
| Cause | Frequency |
|---|---|
| Tone — Uterine atony | 75–90% |
| Trauma — Genital tract lacerations | Up to 20% |
| Tissue — Retained placental fragments | ~10% |
| Thrombin — Coagulopathy | Uncommon |
Uterine Atony (Most Common)
- Uterus feels soft and boggy on examination
- Predisposing factors: multiple gestation, fetal macrosomia, polyhydramnios, prolonged labor, chorioamnionitis, tocolytic use, general anesthesia with halogenated agents
Management:
- Bimanual uterine massage
- Uterotonics: Oxytocin 10 units IM → IV infusion (up to 40 units total)
- Misoprostol, carboprost, ergometrine if oxytocin fails
- Balloon tamponade
- Surgical: B-Lynch suture, uterine artery ligation, emergency hysterectomy
(Rosen's Emergency Medicine; Tintinalli's Emergency Medicine)
4. Wound and Perineal Infections
Incidence: ~3–5% after cesarean delivery.
Organisms: S. aureus (including MRSA), aerobic streptococci, aerobic/anaerobic gram-negative bacilli.
Risk Factors: Prolonged labor, ruptured membranes, obesity, diabetes, immunosuppression, poor surgical technique.
Diagnosis: Erythema, induration, and tenderness at incision margins; purulent discharge. Culture wound exudate routinely to exclude MRSA.
Serious Complication — Necrotizing Fasciitis:
- Extensive, rapidly spreading necrosis of skin and deep fascia
- Skin progresses: red → purple → blue → blisters/bullae → frank gangrene
- "Pain out of proportion" to injury is a key clinical clue
- Management: Broad-spectrum IV antibiotics (clindamycin + vancomycin + gentamicin/aztreonam) plus aggressive surgical debridement — life-saving
5. Puerperal Mastitis and Breast Abscess
Puerperal mastitis typically presents in the second postpartum week due to milk stasis and retrograde infection.
Clinical Features:
- Severe pain, tenderness, swelling, redness of breast
- Fever, chills, myalgias
Causative Organisms:
- Staphylococcus aureus (40% of cases) — including community-acquired MRSA
- E. coli, Streptococcus spp.
Treatment:
- Frequent analgesia
- Continued breast emptying / breastfeeding (do not interrupt)
- Antibiotics: Antistaphylococcal penicillins or cephalosporins
- Do not give sulfamethoxazole-trimethoprim to lactating mothers with infants <2 months
Breast Abscess:
- Complicates mastitis in ~3% of cases
- Ultrasound-guided drainage is first-line
- Surgical drainage reserved as last resort (risk of milk fistula)
(Tintinalli's Emergency Medicine)
6. Septic Pelvic Thrombophlebitis
A complication occurring in <1% of patients with puerperal endometritis. Presents in two forms:
- Acute thrombosis of one ovarian vein — fever, flank pain, palpable tender mass
- Enigmatic fever — persistent fever despite adequate antibiotics, no localizing signs
Treatment: IV heparin anticoagulation + continued antibiotics; fever typically resolves within 24–48 hours.
7. Puerperal Psychiatric Disorders
A. Postpartum Blues ("Baby Blues")
- Affects up to 65% of mothers
- Onset: day 2–5 postpartum
- Features: tearfulness, mood lability, anxiety
- Self-limiting within 2 weeks
- Management: reassurance and support
B. Postpartum Depression (PPD)
- Affects 3–6% of women (DSM-5)
- Onset: during pregnancy or within 4 weeks of delivery (DSM-5 specifier: "with peripartum onset")
- Features: sustained depressed mood, anhedonia, guilt, sleep disturbance, cognitive impairment
- Risk factors: prior depressive episodes, bipolar disorder, family history, poor social support
- Management: psychotherapy, SSRIs, social support
C. Postpartum Psychosis
- Most severe form; rare (~1–2 per 1000 deliveries)
- Onset: within first 2 weeks postpartum
- Features: confusion, disorganized behavior, hallucinations (command hallucinations to harm infant), delusions
- Infanticide risk — psychiatric emergency requiring urgent hospitalization
- Strongly associated with bipolar disorder
- Management: antipsychotics, mood stabilizers, psychiatric hospitalization
| Feature | Baby Blues | PPD | Postpartum Psychosis |
|---|---|---|---|
| Onset | Days 2–5 | Within 4 weeks | Days 1–14 |
| Prevalence | ~65% | 3–6% | ~0.1–0.2% |
| Duration | <2 weeks | Weeks–months | Variable |
| Psychosis | No | No | Yes |
| Treatment | Reassurance | SSRIs/therapy | Hospitalization, antipsychotics |
(Rosen's Emergency Medicine; Adams & Victor's Neurology)
Summary Table — Puerperal Disorders at a Glance
| Disorder | Key Feature | Key Organism/Cause | Treatment |
|---|---|---|---|
| Puerperal Sepsis | Fever + hypotension + abdominal pain | S. pyogenes | Penicillin/IV antibiotics |
| Endometritis | Uterine tenderness + malodorous lochia | Polymicrobial | Clindamycin + Gentamicin |
| Primary PPH | Soft boggy uterus, shock | Uterine atony (75–90%) | Massage + Oxytocin |
| Wound Infection | Erythema/pus at incision | S. aureus, MRSA | Open, drain, antibiotics |
| Necrotizing Fasciitis | Gangrene, "pain out of proportion" | Mixed anaerobes | Debridement + broad antibiotics |
| Puerperal Mastitis | Tender red breast, 2nd week | S. aureus | Antistaphylococcal antibiotics |
| Septic Thrombophlebitis | Fever unresponsive to antibiotics | Venous thrombosis | Heparin + antibiotics |
| PPD | Sustained low mood, >2 weeks | Hormonal/psychosocial | SSRIs, psychotherapy |
| Postpartum Psychosis | Hallucinations, delusions | Bipolar predisposition | Hospitalization, antipsychotics |
Prevention Highlights
- Antibiotic prophylaxis at cesarean delivery significantly reduces endometritis and wound infections
- Intrapartum GBS prophylaxis reduces chorioamnionitis and neonatal sepsis
- Chlorhexidine skin preparation preferred over povidone-iodine
- Skilled birth attendance and proper obstetric technique reduce birth trauma
- Early psychiatric screening in the postpartum period for PPD
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine, Blocks 11 & 18
- Rosen's Emergency Medicine, Block 32
- Tintinalli's Emergency Medicine, Block 8
- Goldman-Cecil Medicine, Block 44
- Adams & Victor's Principles of Neurology, Block 18
Will you present the all disorder including its cause clinical features and management in tabular format
Here is a comprehensive tabular presentation of all puerperal disorders with causes, clinical features, and management:
Puerperal Disorders — Complete Tabular Reference
Table 1: Infectious Puerperal Disorders
| Disorder | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|
| Puerperal Sepsis | Streptococcus pyogenes (GAS); nosocomial or household transmission | Fever, abdominal pain, hypotension; ± absence of expected tachycardia or leukocytosis; onset within 4 days of delivery | IV Penicillin G or ampicillin; supportive care; ICU if septic shock; source control |
| Puerperal Endometritis | Polymicrobial — GBS, E. coli, Bacteroides, Peptostreptococcus, Prevotella, C. trachomatis (late onset) | Fever ≥38°C within 36 hrs of delivery; uterine tenderness; malodorous lochia; lower abdominal pain; tachycardia; malaise | Clindamycin 900 mg IV q8h + Gentamicin 5 mg/kg IV q24h; add Ampicillin if Enterococcus suspected; IV until afebrile ×24 hrs |
| Puerperal Mastitis | S. aureus (40%), E. coli, Streptococcus spp.; community-acquired MRSA possible | Onset 2nd postpartum week; severe breast pain, tenderness, swelling, redness; fever, chills, myalgias | Continue breastfeeding; antistaphylococcal penicillin or cephalosporin; analgesia; if MRSA — clindamycin or vancomycin |
| Breast Abscess | S. aureus (including MRSA); complicates mastitis in ~3% | Discrete tender fluctuant mass; pus on ultrasound (hypoechoic collection, no vascular signal) | Ultrasound-guided aspiration/drainage (first-line); antibiotics (cephalosporin/clindamycin/IV vancomycin); surgical drainage only as last resort |
| Wound Infection (C-section) | S. aureus, MRSA, aerobic streptococci, aerobic/anaerobic gram-negative bacilli | Erythema, induration, tenderness at incision; purulent discharge; onset 3–8 days postpartum | Open and drain wound; wound irrigation + repacking; antibiotics; vancomycin if MRSA culture-positive |
| Necrotizing Fasciitis | Mixed anaerobes + S. pyogenes; complicates wound/episiotomy infection | Pain out of proportion to wound; rapid spread; skin: red → purple → blue → blistering → gangrene; systemic shock; fever | Surgical emergency — aggressive wide debridement of all necrotic tissue; Clindamycin + Vancomycin + Gentamicin/Aztreonam IV; ICU care |
| Urinary Tract Infection | E. coli (most common), Klebsiella, Proteus | Dysuria, frequency, urgency; fever if pyelonephritis; flank pain; urinalysis: pyuria, bacteriuria | Urine culture and sensitivity; oral antibiotics for uncomplicated UTI; IV antibiotics for pyelonephritis |
| Perineal / Episiotomy Infection | S. aureus, E. coli, mixed anaerobes; inadequate wound healing | Pain, swelling, discharge from perineum; wound dehiscence; fever | Wound debridement; antibiotics; perineal hygiene; delayed secondary repair after infection resolves |
Table 2: Hemorrhagic Puerperal Disorders
| Disorder | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|
| Primary PPH (within 24 hrs) | Four Ts: Tone (uterine atony — 75–90%); Trauma (lacerations — 20%); Tissue (retained placenta — 10%); Thrombin (coagulopathy — rare) | Excessive vaginal bleeding; soft boggy uterus (atony); visible tears; signs of haemorrhagic shock (may not appear until >1500 mL lost) | Bimanual uterine massage; Oxytocin 10 units IM then IV infusion; Misoprostol; Ergometrine; balloon tamponade; B-Lynch suture; uterine artery ligation; emergency hysterectomy |
| Secondary PPH (24 hrs – 6 wks) | Retained placental fragments; subinvolution of placental site; endometritis; coagulopathy | Abnormal uterine bleeding after initial normal recovery; uterine tenderness if infected; ultrasound may show echogenic material in uterus | Oxytocics (oxytocin/ergometrine); antibiotics if infection present; surgical uterine evacuation if retained products confirmed on ultrasound |
| Uterine Atony | Multiple gestation; fetal macrosomia; polyhydramnios; prolonged labour; chorioamnionitis; tocolytic use; halogenated anaesthetic agents | Uterus feels soft, enlarged, and boggy on palpation; heavy continuous bleeding; ± haemorrhagic shock | Uterine massage; Oxytocin → Carboprost → Misoprostol → Ergometrine; intrauterine balloon; surgical/radiological intervention |
| Uterine Inversion | Mismanaged third stage; fundal pressure; short cord; adherent placenta | Sudden severe pain; haemorrhage; failure to palpate fundus abdominally; visible/palpable mass at cervix or vagina | Do NOT remove placenta if attached; manual replacement (Johnson manoeuvre); tocolytics to relax uterus; IV fluids and blood transfusion |
| Uterine Rupture | Prior uterine scar (C-section); obstructed labour; oxytocin misuse; grand multiparity | Sudden severe abdominal pain; cessation of contractions; fetal parts palpable outside uterus; fetal distress; maternal shock | Emergency laparotomy — uterine repair or hysterectomy; blood transfusion; ICU support |
Table 3: Thromboembolic Puerperal Disorders
| Disorder | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|
| Deep Vein Thrombosis (DVT) | Virchow's triad: stasis (bedrest, C-section), hypercoagulability (pregnancy), vessel injury | Unilateral leg pain, swelling, warmth, erythema; Homans sign (unreliable); Doppler USS confirms | LMWH (enoxaparin); compression stockings; mobilization; monitor for PE |
| Pulmonary Embolism (PE) | Dislodged DVT; venous thromboembolism in puerperium | Sudden dyspnoea, pleuritic chest pain, haemoptysis, tachycardia, hypoxia; ± collapse | LMWH or unfractionated heparin; thrombolysis if massive PE with haemodynamic instability |
| Septic Pelvic Thrombophlebitis | Complication of endometritis; thrombosis of ovarian/pelvic veins with superimposed infection | Fever persisting despite adequate antibiotics; flank/lower abdominal pain; ± palpable tender mass; no other localizing source | IV heparin anticoagulation + continued broad-spectrum antibiotics; fever resolves within 24–48 hrs |
| Cerebral Venous Thrombosis | Hypercoagulable state of puerperium | Puerperal headache worsening over days; behavioural change; seizures; focal neurological deficits | Anticoagulation (LMWH/heparin); antiepileptics if seizures; MRI/MRV for diagnosis |
Table 4: Puerperal Psychiatric Disorders
| Disorder | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|
| Postpartum Blues ("Baby Blues") | Rapid postpartum fall in oestrogen and progesterone; psychological adjustment | Onset day 2–5; tearfulness, mood lability, anxiety, irritability, mild insomnia; self-limiting | Reassurance and emotional support; no pharmacotherapy needed; resolves within 2 weeks |
| Postpartum Depression (PPD) | Hormonal shifts; psychosocial stressors; prior depressive history; sleep deprivation; poor social support | Onset within 4 weeks (DSM-5) to 1 year postpartum; persistent low mood, anhedonia, guilt, fatigue, cognitive impairment, anxiety, poor bonding with infant | Edinburgh Postnatal Depression Scale (EPDS) for screening; SSRIs (sertraline first-line); cognitive-behavioural therapy; social support; refer to psychiatry if severe |
| Postpartum Psychosis | Strong association with bipolar disorder; prior postpartum psychotic episode; family history | Onset within first 2 weeks; confusion, disorientation, command hallucinations (to harm infant), delusions, rapid mood swings, bizarre behaviour | Psychiatric emergency — urgent hospitalisation; antipsychotics; mood stabilisers (lithium); ECT if refractory; safeguard infant; do not leave mother alone with baby |
Table 5: Other Puerperal Complications
| Disorder | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|
| Postpartum Urinary Retention | Perineal oedema; pain inhibiting micturition; epidural anaesthesia; bladder overdistension during labour | Inability to void within 6 hrs of delivery; suprapubic fullness; bladder palpable abdominally; ± overflow incontinence | Catheterisation (intermittent or indwelling); adequate analgesia; trial of voiding after 24–48 hrs |
| Breast Engorgement | Inadequate milk removal; infant separation; poor latch; milk stasis | Onset day 3–5; painful, hard, enlarged bilateral breasts; low-grade fever; nausea | Frequent breastfeeding/pumping; correct latch technique; warm compresses; manual massage; analgesics |
| Subinvolution of Uterus | Retained placental fragments; endometritis; uterine fibroids | Uterus larger and softer than expected for postpartum day; prolonged/heavy lochia; ± fever if infected | Oxytocics (ergometrine/oxytocin); antibiotics if infection present; ultrasound-guided surgical evacuation if products retained |
| Postpartum Thyroiditis | Autoimmune (anti-TPO antibodies); Hashimoto's predisposition | Transient hyperthyroid phase (1–4 months) → hypothyroid phase (4–8 months) → often recovery; fatigue, palpitations, weight changes | Symptomatic: beta-blockers for hyperthyroid phase; levothyroxine for hypothyroid phase; majority recover within 12–18 months; monitor TFTs annually |
| Puerperal Eclampsia | Persistent hypertension postpartum; failure to resolve pre-eclampsia; de novo onset (rare) | Seizures; severe headache; visual disturbances; hypertension; proteinuria; onset within 48 hrs (usually) up to 4 weeks postpartum | IV Magnesium sulphate (anti-seizure); antihypertensives (labetalol, nifedipine, hydralazine); close monitoring; ICU if severe |
Quick-Reference Summary Card
| Disorder | Key Diagnostic Clue | First-Line Treatment |
|---|---|---|
| Puerperal Sepsis | Fever + hypotension + abdominal pain within 4 days | IV Penicillin |
| Endometritis | Uterine tenderness + malodorous lochia + fever | Clindamycin + Gentamicin |
| Primary PPH | Soft boggy uterus + heavy bleeding | Oxytocin + Uterine massage |
| Secondary PPH | Heavy bleeding 24 hrs – 6 weeks | Oxytocics ± evacuation |
| Wound Infection | Pus/erythema at incision | Open, drain, antibiotics |
| Necrotizing Fasciitis | Pain out of proportion + gangrene | Surgical debridement (emergency) |
| Mastitis | Tender red breast, 2nd postpartum week | Antistaphylococcal antibiotics |
| Breast Abscess | Discrete fluctuant mass on USS | USS-guided drainage |
| Septic Thrombophlebitis | Fever persisting despite antibiotics | Heparin + antibiotics |
| Baby Blues | Mild mood changes day 2–5 | Reassurance only |
| PPD | Sustained low mood >2 weeks | SSRI + psychotherapy |
| Postpartum Psychosis | Hallucinations/delusions, harm to infant risk | Emergency psychiatric admission |
| Postpartum Thyroiditis | Hyper then hypothyroid phases | Beta-blockers / Levothyroxine |
| Puerperal Eclampsia | Seizures + hypertension postpartum | Magnesium sulphate |
Sources: Creasy & Resnik's Maternal-Fetal Medicine • Rosen's Emergency Medicine • Tintinalli's Emergency Medicine • Goldman-Cecil Medicine • Adams & Victor's Principles of Neurology • Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Will you present the all disorder including its defination ,cause ,clinical features and management in tabular format
Puerperal Disorders — Complete Reference Table (Definition · Causes · Clinical Features · Management)
Table 1: Infectious Puerperal Disorders
| Disorder | Definition | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|---|
| Puerperal Pyrexia / Sepsis | Temperature ≥38°C (100.4°F) on any 2 of the first 10 days postpartum (excluding first 24 hrs), caused by S. pyogenes bacteraemia | Streptococcus pyogenes (GAS); nosocomial or household transmission from carriers of streptococcal pharyngitis | Fever, severe abdominal pain, hypotension; deceptively absent tachycardia/leukocytosis early; onset within 4 days of delivery; incidence 6–80/100,000 live births; CFR ~3.5% | IV Penicillin G or ampicillin; supportive IV fluids; ICU admission if septic shock; source control; blood cultures before antibiotics |
| Puerperal Endometritis | Infection of the uterine endometrium (and often myometrium) arising within the first 10 days postpartum, characterised by polymicrobial ascending infection from vaginal flora | GBS, E. coli, K. pneumoniae, Bacteroides, Prevotella, Peptostreptococcus; C. trachomatis in late-onset cases; ascends via vaginal examinations/surgery | Fever ≥38°C within 36 hrs of delivery; uterine tenderness; malodorous lochia; lower abdominal pain; tachycardia; malaise; ± broad ligament mass | Clindamycin 900 mg IV q8h + Gentamicin 5 mg/kg IV q24h (first-line); add Ampicillin if Enterococcus suspected; IV until afebrile ×24 hrs; no routine oral antibiotics on discharge |
| Puerperal Mastitis | Inflammatory condition of the breast parenchyma occurring in the postpartum period, caused by bacterial infection secondary to milk stasis and ductal retrograde spread | S. aureus (40%), E. coli, Streptococcus spp.; community-acquired MRSA increasingly recognised | Onset typically 2nd postpartum week; unilateral severe breast pain, tenderness, erythema, swelling; fever, chills, myalgias; elevated WBC | Continue breastfeeding; antistaphylococcal penicillin or cephalosporin; analgesics; if MRSA suspected — oral clindamycin or IV vancomycin; reassess if no response in 48 hrs |
| Breast Abscess | A localised collection of pus within breast tissue, complicating mastitis in approximately 3% of cases, characterised by discrete encapsulation of infected material | S. aureus including MRSA; failure/inadequate treatment of mastitis; milk stasis with bacterial superinfection | Discrete tender fluctuant mass; pointing/discharging pus; USS shows hypoechoic fluid collection with absent vascular signals; fever persisting despite antibiotics | USS-guided needle aspiration or drainage (first-line); antistaphylococcal antibiotics ± vancomycin for MRSA; continue breastfeeding; surgical drainage reserved as last resort (risk of milk fistula) |
| Wound Infection (Post-Caesarean) | Superficial or deep infection of the abdominal surgical incision following caesarean delivery, occurring in 3–5% of caesarean births | S. aureus, MRSA, aerobic streptococci, aerobic/anaerobic gram-negative bacilli; risk ↑ with prolonged labour, obesity, diabetes, immunosuppression | Erythema, induration, tenderness at incision margins; purulent discharge; onset day 3–8 postpartum; ± extensive cellulitis without frank pus; fever | Open and completely drain wound; irrigate and repack with moist gauze 2–3×/day; antibiotics; add vancomycin if MRSA confirmed; secondary wound closure after granulation; suction device in morbidly obese |
| Necrotizing Fasciitis | A rapidly progressive, life-threatening deep-tissue infection involving subcutaneous tissue and fascia with extensive necrosis, rarely complicating episiotomy or abdominal wounds | Mixed anaerobes + S. pyogenes; risk ↑ with diabetes, obesity, cancer, immunodeficiency; portal of entry: episiotomy, wound, or cryptic (no visible entry) | "Pain out of proportion" to wound appearance (key clue); rapid spread; skin progression: red → purple → blue → blistering/bullae → frank gangrene by day 4–5; high fever, extreme prostration; bacteraemia; shock | Surgical emergency: aggressive wide debridement of ALL necrotic tissue; IV Clindamycin + Vancomycin + Gentamicin/Aztreonam; ICU resuscitation; crystalloid infusion; electrolyte correction; repeated debridement often required |
| Urinary Tract Infection (UTI/Pyelonephritis) | Bacterial infection of the lower (cystitis) or upper (pyelonephritis) urinary tract occurring in the puerperium, facilitated by catheterisation and bladder trauma during labour | E. coli (most common), Klebsiella, Proteus, Enterococcus; catheterisation, bladder overdistension, perineal trauma predispose | Dysuria, frequency, urgency, suprapubic pain (cystitis); fever, rigors, costovertebral angle tenderness, nausea/vomiting (pyelonephritis); pyuria + bacteriuria on urinalysis | MSU culture and sensitivity; oral antibiotics for uncomplicated cystitis (nitrofurantoin/trimethoprim); IV cephalosporin or gentamicin for pyelonephritis; adequate hydration |
| Perineal / Episiotomy Infection | Infection of the perineal body or episiotomy repair site, characterised by wound breakdown, cellulitis, or abscess formation in the postpartum period | S. aureus, E. coli, mixed anaerobes, GBS; predisposed by haematoma, poor tissue apposition, prolonged labour, obesity | Perineal pain, swelling, purulent discharge from wound; wound dehiscence; ± foul odour; fever; ± extension to deeper fascia (necrotizing fasciitis risk) | Wound debridement and opening; antibiotics (broad-spectrum); perineal hygiene (sitz baths); delayed secondary repair after infection fully resolved |
Table 2: Hemorrhagic Puerperal Disorders
| Disorder | Definition | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|---|
| Primary Postpartum Haemorrhage (PPH) | Blood loss >500 mL after vaginal delivery or >1000 mL after caesarean, occurring within the first 24 hours of delivery | 4 Ts: Tone — uterine atony (75–90%); Trauma — lacerations (20%); Tissue — retained placenta (10%); Thrombin — coagulopathy (rare) | Heavy continuous vaginal bleeding; soft, boggy uterus (atony); visible tears/lacerations; signs of haemorrhagic shock; NB: patient may not show shock until >1500 mL lost due to pregnancy-related plasma expansion | Bimanual uterine massage; Oxytocin 10 units IM then IV infusion; Misoprostol; Carboprost; Ergometrine; intrauterine balloon tamponade; B-Lynch suture; uterine artery ligation; emergency hysterectomy as last resort; IV fluids/blood transfusion |
| Secondary PPH | Abnormal or excessive uterine bleeding occurring between 24 hours and 6 weeks postpartum | Retained placental fragments; subinvolution of placental site; endometritis; uterine arteriovenous malformation; coagulopathy | Abnormal heavy vaginal bleeding after initial normal recovery; uterine tenderness if infected; ± fever; USS may show echogenic material (retained products) in uterine cavity | Oxytocics (ergometrine/oxytocin); antibiotics if infection coexists; ultrasound-guided surgical uterine evacuation if retained products confirmed |
| Uterine Atony | Failure of the myometrium to contract adequately after delivery of the placenta, resulting in failure to compress the spiral arteries and causing the most common form of PPH | Multiple gestation; fetal macrosomia; polyhydramnios; prolonged labour; chorioamnionitis; tocolytic agents; halogenated anaesthetic agents; multiparity | Palpable soft, enlarged, boggy uterus; continuous heavy bleeding; haemodynamic instability; diagnosis of exclusion after ruling out trauma and retained placenta | Uterine massage; stepwise uterotonics: Oxytocin → Carboprost → Misoprostol → Ergometrine; intrauterine balloon; compression sutures; uterine artery embolisation; hysterectomy |
| Uterine Inversion | Rare but life-threatening condition where the uterine fundus collapses into the uterine cavity or beyond, occurring during the third stage of labour | Mismanaged third stage (cord traction before placental separation); fundal pressure; fundal placentation; short umbilical cord; uterine atony; connective tissue disorders | Sudden severe pain and haemorrhage; failure to palpate fundus abdominally; visible/palpable mass at cervix, vagina, or introitus; profound haemorrhagic shock | Do NOT manually remove placenta if still attached; manual replacement (Johnson manoeuvre); tocolytics (terbutaline/MgSO₄) to relax uterus; IV fluids/blood; surgical correction if manual replacement fails |
| Uterine Rupture | A full-thickness disruption of the uterine wall, most commonly at a prior scar, occurring during labour or the postpartum period | Previous uterine scar (LSCS, myomectomy); obstructed labour; oxytocin misuse; grand multiparity; trauma; congenital uterine anomaly | Sudden severe abdominal pain; cessation of uterine contractions; fetal parts palpable outside uterus abdominally; fetal heart rate abnormalities/loss; maternal haemorrhagic shock | Emergency laparotomy — uterine repair (if feasible) or peripartum hysterectomy; massive blood transfusion; ICU support; neonatal resuscitation |
Table 3: Thromboembolic Puerperal Disorders
| Disorder | Definition | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|---|
| Deep Vein Thrombosis (DVT) | Formation of a thrombus within the deep venous system (typically femoral/iliac veins) during the puerperium, driven by Virchow's triad | Venous stasis (immobility, bedrest, C-section); hypercoagulability (↑ clotting factors in pregnancy); vessel injury (pelvic/surgical trauma); dehydration; obesity | Unilateral leg pain, swelling, warmth, erythema; ± Homans sign (unreliable); low-grade fever; Doppler ultrasound confirms | LMWH (enoxaparin); graduated compression stockings; early mobilisation; convert to warfarin after 6 weeks if not breastfeeding; treat for minimum 3 months |
| Pulmonary Embolism (PE) | Life-threatening obstruction of pulmonary arterial circulation by a dislodged thrombus, most commonly arising from pelvic/leg DVT in the puerperium | Dislodged DVT (pelvic/femoral veins); hypercoagulable puerperal state; immobility; C-section; prior VTE history | Sudden dyspnoea, pleuritic chest pain, haemoptysis, tachycardia, hypoxia; ± haemodynamic collapse (massive PE); elevated D-dimer; CTPA confirms | LMWH or unfractionated heparin; thrombolysis (alteplase) if massive PE with haemodynamic instability; oxygen; ICU; surgical embolectomy rarely needed |
| Septic Pelvic Thrombophlebitis | Thrombosis of the ovarian or pelvic veins superimposed with bacterial infection, complicating <1% of puerperal endometritis cases | Extension of endometritis causing thrombosis of pelvic/ovarian veins; E. coli, Bacteroides, mixed organisms | Fever persisting despite adequate antibiotics (hallmark sign); flank or lower abdominal pain; ± palpable tender mass; no other localising source of fever | IV heparin anticoagulation + continued broad-spectrum antibiotics; fever typically resolves within 24–48 hrs — confirms diagnosis therapeutically |
| Cerebral Venous Thrombosis | Aseptic thrombosis of the cerebral venous sinuses occurring in the hypercoagulable puerperal state, most commonly involving the superior sagittal sinus | Puerperal hypercoagulability; dehydration; sepsis; thrombophilia; prior OCP use; anaemia | Puerperal headache worsening over days; behavioural/personality change; focal neurological deficits; convulsive seizures; papilloedema; ± coma | Anticoagulation (LMWH/heparin even if haemorrhagic infarct); antiepileptics for seizures; ICP management; MRI/MRV is diagnostic gold standard |
Table 4: Puerperal Psychiatric Disorders
| Disorder | Definition | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|---|
| Postpartum Blues ("Baby Blues") | A mild, transient, self-limiting mood disturbance affecting up to 65% of mothers, arising in the first week postpartum and resolving spontaneously within 2 weeks | Rapid postpartum fall in oestrogen and progesterone; psychological adjustment to new role; sleep deprivation; emotional vulnerability; no pathological basis | Onset day 2–5; tearfulness, mood lability, irritability, mild anxiety, emotional sensitivity, fatigue; symptoms mild and self-limiting; no functional impairment | Reassurance and emotional support only; psychoeducation of mother and partner; no pharmacotherapy required; monitor for progression to PPD if persisting >2 weeks |
| Postpartum Depression (PPD) | A major depressive episode occurring during pregnancy or within 4 weeks of delivery (DSM-5 specifier: "with peripartum onset"), affecting 3–6% of women, characterised by sustained depressed mood and functional impairment | Rapid hormonal shifts (oestrogen/progesterone withdrawal); HPA axis dysregulation; prior depressive/bipolar history; poor social support; sleep deprivation; stressful life events; thyroid dysfunction | Persistent low mood, anhedonia, excessive guilt, worthlessness, cognitive impairment, sleep disturbance (beyond neonatal demands), fatigue, poor infant bonding, anxiety, suicidal ideation in severe cases | Screen with EPDS (score ≥13 positive); SSRIs (sertraline first-line — safe in breastfeeding); cognitive-behavioural therapy; peer support; social services; brexanolone (IV neuroactive steroid — new approved option); psychiatric referral if severe/suicidal |
| Postpartum Psychosis | The most severe puerperal psychiatric disorder, characterised by acute onset psychosis within the first 2 weeks postpartum, representing a psychiatric emergency with risk of infanticide and suicide; affects ~1–2 per 1000 deliveries | Strong association with bipolar disorder (strongest risk factor); prior postpartum psychotic episode; family history of bipolar/psychosis; first-time motherhood; sleep deprivation; sudden hormone withdrawal | Onset within first 2 weeks (often days 3–5); confusion, disorientation, rapidly fluctuating mood; command hallucinations (to harm infant); delusions; bizarre behaviour; insomnia; agitation; risk of infanticide | Psychiatric emergency — urgent hospital admission; never leave mother alone with infant; antipsychotics (haloperidol/olanzapine); lithium for bipolar subtype; ECT if refractory; mother-baby unit if available; safeguarding of infant |
Table 5: Other Puerperal Complications
| Disorder | Definition | Causes / Aetiology | Clinical Features | Management |
|---|---|---|---|---|
| Postpartum Urinary Retention | Inability to void spontaneously within 6 hours of delivery, due to impaired bladder function in the immediate puerperium | Perineal oedema causing urethral compression; pain inhibiting micturition reflex; epidural anaesthesia impairing bladder sensation; bladder overdistension during prolonged labour | Inability to void; suprapubic fullness; bladder palpable/percussible abdominally; ± overflow incontinence (dribbling); USS bladder volume >150 mL post-void confirms | Intermittent or indwelling catheterisation; adequate analgesia; trial of void after 24–48 hrs; physiotherapy; anticholinergic reversal if anaesthesia-related; monitor for UTI |
| Breast Engorgement | Painful bilateral overfilling of the breasts with milk due to inadequate milk removal, typically occurring on days 3–5 postpartum | Inadequate milk removal; infant separation; sore nipples preventing latch; improper breastfeeding technique; sudden cessation of breastfeeding; milk stasis | Onset day 3–5; bilateral painful, hard, engorged breasts; warmth; ± low-grade fever; nausea; compressed nipple-areola complex making latch difficult | Frequent breastfeeding or pumping; correct latch technique; warm compresses before feeding; cold compresses after feeding; manual massage to facilitate milk let-down; analgesics (ibuprofen/paracetamol) |
| Subinvolution of Uterus | Failure of the puerperal uterus to return to its normal pre-pregnant size within the expected timeframe, due to incomplete physiological regression | Retained placental fragments; endometritis; uterine fibroids; polyhydramnios; multiple gestation; prolonged labour; high parity | Uterus larger and softer than expected for postpartum day; prolonged/excessive lochia; ± offensive lochia if infected; ± pelvic pain; fever if endometritis coexists | Oxytocics (ergometrine or oral oxytocin); antibiotics if infection present; USS-guided surgical evacuation (ERPC) if retained products confirmed; follow-up pelvic USS to confirm resolution |
| Postpartum Thyroiditis | An autoimmune inflammatory thyroid condition occurring within the first year postpartum, characterised by a transient hyperthyroid phase followed by a hypothyroid phase, affecting 5–10% of women | Autoimmune rebound after postpartum immune tolerance reversal; anti-TPO antibody positivity; underlying Hashimoto's thyroiditis; genetic predisposition | Phase 1 (1–4 months): fatigue, palpitations, tremor, heat intolerance, weight loss (hyperthyroid) → Phase 2 (4–8 months): fatigue, cold intolerance, weight gain, constipation, depression (hypothyroid) → Phase 3: usually recovery by 12–18 months | Hyperthyroid phase: beta-blockers (propranolol) — no antithyroid drugs (not autoimmune-driven); Hypothyroid phase: levothyroxine replacement; monitor TFTs every 3–6 months; ~25% develop permanent hypothyroidism — screen annually |
| Puerperal / Postpartum Eclampsia | Occurrence of grand mal seizures in a woman with pre-eclampsia or de novo hypertension, arising within 48 hours (occasionally up to 4 weeks) postpartum, without other neurological cause | Persistence or new onset of severe hypertension postpartum; cerebral vasospasm; endothelial dysfunction; failure of pre-eclampsia to resolve after delivery; cerebral oedema | Grand mal tonic-clonic seizures; severe headache; visual disturbances (blurring, scotomata); hypertension (BP ≥160/110 mmHg); proteinuria; facial/peripheral oedema; ± HELLP syndrome | IV Magnesium sulphate (4–6 g loading dose, then 1–2 g/hr) — prevents/controls seizures; antihypertensives: IV labetalol/hydralazine or oral nifedipine; strict fluid balance; ICU monitoring; rectal diazepam for breakthrough seizures |
Master Quick-Reference Summary
| # | Disorder | Definition (One Line) | Key Cause | Pathognomonic Feature | First-Line Treatment |
|---|---|---|---|---|---|
| 1 | Puerperal Sepsis | GAS bacteraemia within 4 days postpartum | S. pyogenes | Fever + hypotension without tachycardia | IV Penicillin G |
| 2 | Endometritis | Uterine infection within 10 days postpartum | Polymicrobial ascending flora | Malodorous lochia + uterine tenderness | Clindamycin + Gentamicin |
| 3 | Primary PPH | >500 mL blood loss within 24 hrs | Uterine atony (75–90%) | Soft, boggy uterus | Oxytocin + bimanual massage |
| 4 | Secondary PPH | Heavy bleeding 24 hrs to 6 weeks | Retained products/endometritis | Echogenic material on USS | Oxytocics ± evacuation |
| 5 | Uterine Inversion | Fundus collapses into cavity | Mismanaged 3rd stage | No fundus palpable abdominally | Johnson manoeuvre |
| 6 | Uterine Rupture | Full-thickness uterine wall disruption | Previous C-section scar | Fetal parts palpable outside uterus | Emergency laparotomy |
| 7 | Wound Infection | Incision site infection post-LSCS | S. aureus/MRSA | Erythema + pus at wound | Open, drain, antibiotics |
| 8 | Necrotizing Fasciitis | Rapidly spreading deep tissue necrosis | Mixed anaerobes + GAS | Pain out of proportion + gangrene | Emergency surgical debridement |
| 9 | Puerperal Mastitis | Breast parenchymal infection, 2nd week | S. aureus | Localised red, hot, tender breast | Antistaphylococcal antibiotics |
| 10 | Breast Abscess | Localised pus collection in breast | S. aureus/MRSA | Fluctuant mass + hypoechoic USS | USS-guided drainage |
| 11 | DVT | Deep venous thrombosis | Virchow's triad | Unilateral leg swelling + Doppler USS | LMWH |
| 12 | Pulmonary Embolism | Pulmonary arterial occlusion by thrombus | Dislodged pelvic DVT | Sudden dyspnoea + hypoxia | LMWH / thrombolysis |
| 13 | Septic Pelvic Thrombophlebitis | Infected pelvic vein thrombosis | Endometritis extension | Fever persisting despite antibiotics | Heparin + antibiotics |
| 14 | Cerebral Venous Thrombosis | Cerebral sinus thrombosis | Puerperal hypercoagulability | Worsening postpartum headache + seizures | Heparin + MRI/MRV |
| 15 | Baby Blues | Transient mild mood disturbance | Hormonal withdrawal | Self-limiting tearfulness, day 2–5 | Reassurance only |
| 16 | Postpartum Depression | Major depressive episode peripartum | Hormonal/psychosocial | Sustained low mood + poor bonding | SSRI + psychotherapy |
| 17 | Postpartum Psychosis | Acute psychosis with infanticide risk | Bipolar predisposition | Command hallucinations within 2 weeks | Emergency hospitalisation |
| 18 | Subinvolution | Failure of uterine regression | Retained products/infection | Uterus larger than expected | Ergometrine ± evacuation |
| 19 | Postpartum Thyroiditis | Autoimmune biphasic thyroid disorder | Anti-TPO antibodies | Hyper then hypothyroid phases | Beta-blockers/Levothyroxine |
| 20 | Puerperal Eclampsia | Post-delivery seizures with hypertension | Persistent/de novo pre-eclampsia | Seizures + BP ≥160/110 mmHg | IV Magnesium sulphate |
Sources: Creasy & Resnik's Maternal-Fetal Medicine • Rosen's Emergency Medicine • Tintinalli's Emergency Medicine • Goldman-Cecil Medicine • Kaplan & Sadock's Comprehensive Textbook of Psychiatry • Adams & Victor's Principles of Neurology • Berek & Novak's Gynecology
Will you present the all disorder including its defination ,cause ,clinical features and management in point wise
Puerperal Disorders — Complete Point-wise Presentation
PRELIMINARY NOTE
Puerperium = The 6-week period following delivery during which the maternal body returns to its pre-pregnant state. Puerperal disorder = Any pathological condition arising during this period.
SECTION 1: INFECTIOUS PUERPERAL DISORDERS
1. PUERPERAL PYREXIA / PUERPERAL SEPSIS
📌 Definition
- Temperature ≥ 38°C (100.4°F) occurring on any two of the first 10 days postpartum, excluding the first 24 hours
- Any fever ≥ 38.5°C in the first 24 hours is also significant
- Caused by Group A Streptococcal (GAS) bacteraemia in classical puerperal sepsis
🔴 Causes
- Primary organism: Streptococcus pyogenes (Group A Streptococcus)
- Nosocomial transmission from healthcare workers
- Household transmission from children/family with streptococcal pharyngitis
- Women are discharged at 48 hours, so home acquisition is common
- Other organisms: E. coli, anaerobes, Staphylococcus aureus
🟡 Clinical Features
- Fever — high grade, rapid onset
- Abdominal pain — severe, diffuse
- Hypotension — disproportionate to apparent severity
- Deceptively absent tachycardia or leukocytosis in early GAS sepsis
- Onset typically within 4 days of delivery
- Incidence: 6–80 cases per 100,000 live births
- Case-fatality rate: approximately 3.5%
- Higher risk: vaginal delivery, young age, prior streptococcal exposure
🟢 Management
- Blood cultures before starting antibiotics
- IV Penicillin G or ampicillin — first-line
- Clindamycin added if toxic shock syndrome suspected (inhibits toxin production)
- IV fluid resuscitation
- ICU admission if septic shock develops
- Source control — drain any abscess
- Notify public health if nosocomial cluster suspected
2. PUERPERAL ENDOMETRITIS
📌 Definition
- Infection of the uterine endometrium (and often extending to myometrium)
- Arises within the first 10 days postpartum
- Most common cause of puerperal fever
- Incidence: 5–35% depending on mode of delivery and prophylaxis
🔴 Causes
- Polymicrobial ascending infection from normal vaginal flora
- Key organisms:
- Group B Streptococcus (GBS)
- Anaerobic gram-positive cocci (Peptostreptococcus)
- Aerobic gram-negative bacilli (E. coli, K. pneumoniae, Proteus)
- Anaerobic gram-negative bacilli (Bacteroides, Prevotella)
- Chlamydia trachomatis — late-onset endometritis
- Mycoplasma hominis, Ureaplasma urealyticum — minor role
- Risk factors:
- Caesarean delivery (greatest single risk factor)
- Intraamniotic infection (chorioamnionitis)
- Prolonged labour and ruptured membranes
- Multiple vaginal examinations during labour
- Internal fetal monitoring
- Young maternal age
- Pre-existing GBS, gonorrhoea, or bacterial vaginosis
🟡 Clinical Features
- Fever ≥ 38°C within 36 hours of delivery
- Uterine tenderness on palpation
- Malodorous (foul-smelling) lochia — hallmark
- Lower abdominal pain
- Tachycardia
- Malaise, lethargy
- ± Tender indurated mass in broad ligament or posterior cul-de-sac
- Raised WBC count
- Differential includes: UTI, perineal infection, mastitis, wound infection, atelectasis, DVT
🟢 Management
- First-line regimen:
- Clindamycin 900 mg IV q8h + Gentamicin 5 mg/kg IV q24h
- Add Ampicillin 2 g IV q6h if Enterococcus suspected or GBS with clindamycin resistance
- Alternative single agents: ampicillin-sulbactam, piperacillin-tazobactam, imipenem
- 90–95% of patients defervesce within 48–72 hours
- Discontinue IV antibiotics once afebrile and asymptomatic for ~24 hours
- No routine oral antibiotics required after discharge
- Failure to respond → suspect: resistant organism, wound abscess, pelvic abscess, septic pelvic thrombophlebitis, or drug reaction
3. PUERPERAL MASTITIS
📌 Definition
- Inflammatory infection of the breast parenchyma occurring in the postpartum lactating period
- Typically presents in the second postpartum week
- Caused by bacterial infection secondary to milk stasis and retrograde ductal spread
🔴 Causes
- Staphylococcus aureus — 40% of cases (most common)
- Community-acquired MRSA — increasingly recognised
- Escherichia coli
- Streptococcus species
- Predisposing factors:
- Milk stasis
- Cracked or damaged nipples
- Improper breastfeeding technique / poor latch
- Infant separation
- Prior history of mastitis
🟡 Clinical Features
- Severe unilateral breast pain
- Localised tenderness, swelling, redness
- Warmth over affected area
- Fever, chills, myalgias (systemic features)
- Usually affects one breast/quadrant
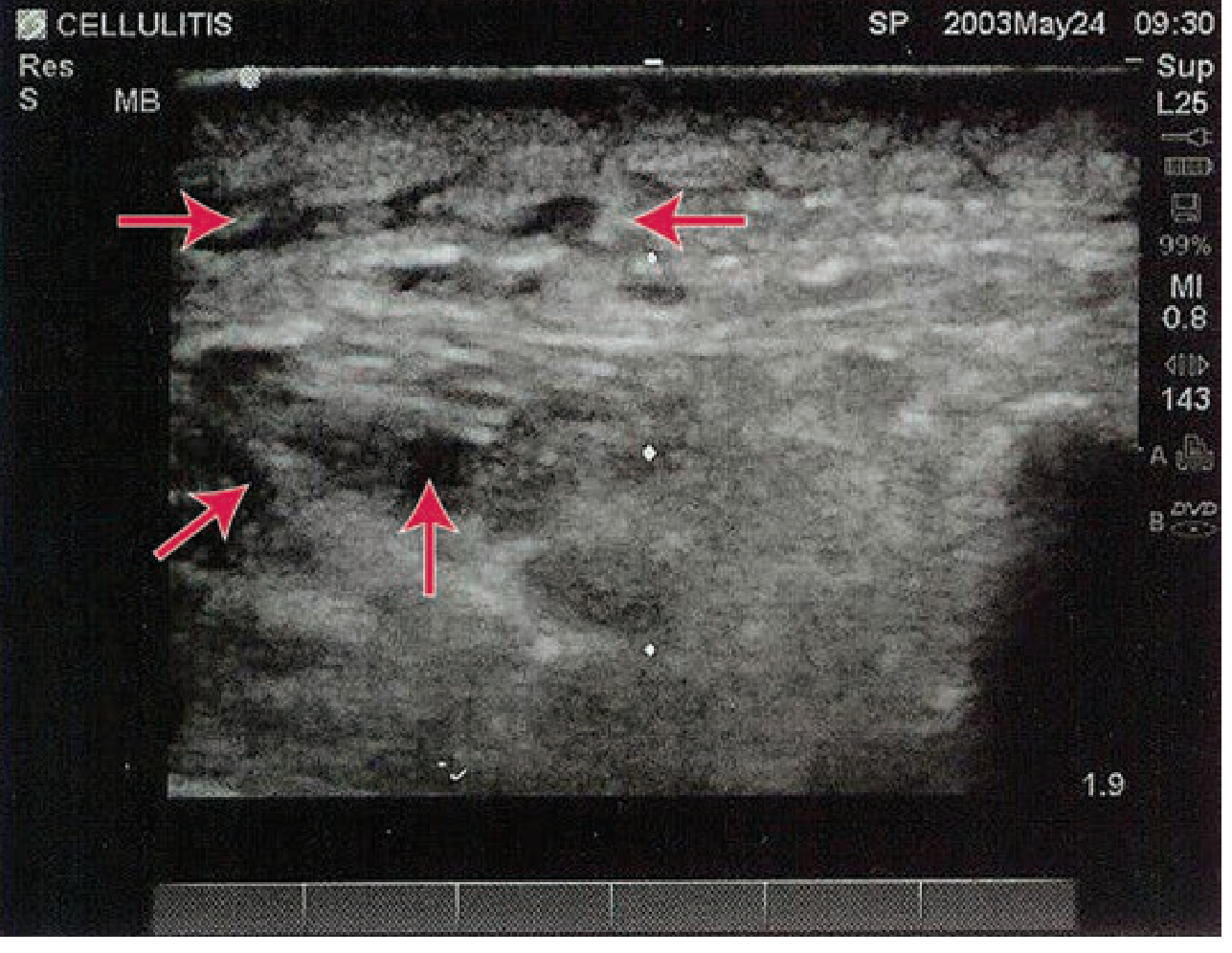
- USS: hypoechoic fluid surrounding subcutaneous fat lobules — no discrete collection
- Differentials: breast engorgement, plugged duct, inflammatory carcinoma (rare)
🟢 Management
- Continue breastfeeding — do NOT interrupt
- Frequent breast emptying (breastfeeding or pumping)
- Antibiotics:
- Antistaphylococcal penicillin (flucloxacillin) or cephalosporins (first-line)
- Clindamycin if penicillin-allergic
- Vancomycin IV if MRSA suspected
- Note: Sulfamethoxazole-trimethoprim contraindicated in lactating mothers with infants < 2 months
- Analgesics (ibuprofen/paracetamol)
- Warm compresses before feeding
- Reassess in 48 hours — if no improvement, evaluate for abscess
4. BREAST ABSCESS
📌 Definition
- A localised collection of pus within breast tissue
- Complicates mastitis in approximately 3% of cases
- Characterised by discrete encapsulation of purulent material
🔴 Causes
- Staphylococcus aureus including MRSA
- Inadequate/delayed treatment of mastitis
- Milk stasis with bacterial superinfection
- Risk factors: cracked nipples, poor drainage, delayed antibiotic therapy
🟡 Clinical Features
- Discrete tender, fluctuant mass in breast
- Pointing/discharging pus through skin
- Persistent fever despite antibiotic treatment
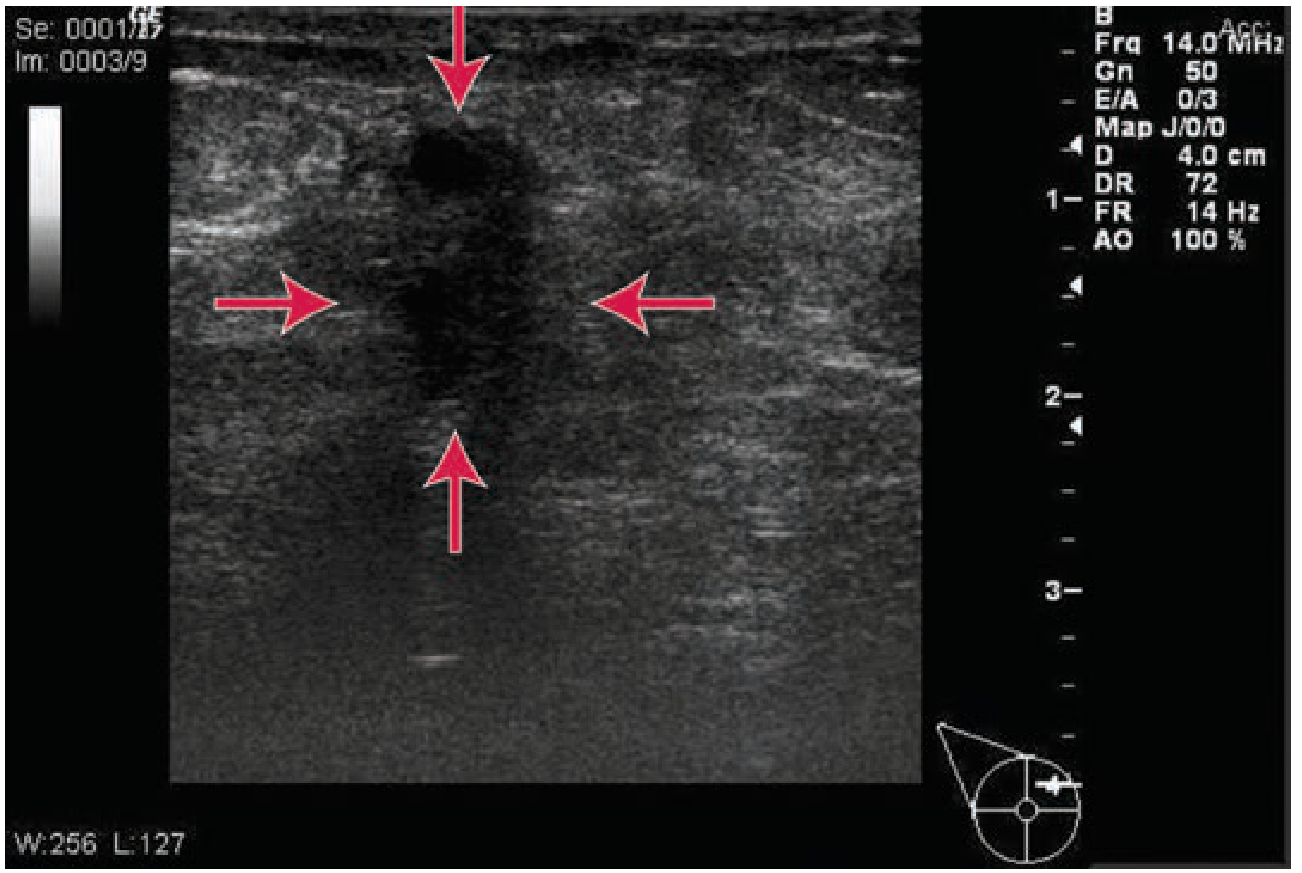
- Ultrasound shows:
- Hypoechoic (dark) fluid collection
- Absence of vascular signals within collection
- This distinguishes it from mastitis (no discrete collection)
🟢 Management
- Ultrasound-guided needle aspiration or drainage — first-line
- Antibiotics: cephalosporin, clindamycin, or IV vancomycin for MRSA
- Continue breastfeeding throughout treatment unless antibiotic is contraindicated in newborn
- Surgical drainage — reserved as last resort only
- Risk of milk fistula in lactating patients
- Repeat USS to confirm resolution
5. POST-CAESAREAN WOUND INFECTION
📌 Definition
- Infection of the abdominal surgical incision following caesarean delivery
- Occurs in approximately 3–5% of caesarean deliveries
- May be superficial (skin/subcutaneous) or deep (fascia/muscle)
🔴 Causes
- Staphylococcus aureus — most common
- MRSA — increasingly important
- Aerobic streptococci
- Aerobic and anaerobic gram-negative bacilli
- Risk factors:
- Prolonged labour and ruptured membranes
- Pre-existing intraamniotic infection
- Obesity (major independent risk factor)
- Insulin-dependent diabetes
- Immunodeficiency or corticosteroid therapy
- Poor surgical technique
🟡 Clinical Features
- Erythema, induration, tenderness at incision margins
- Purulent discharge from wound
- Onset typically day 3–8 postpartum
- ± Extensive cellulitis without frank pus in some patients
- Fever persisting despite antibiotic therapy for endometritis should raise suspicion
- Wound culture: routinely performed to exclude MRSA
🟢 Management
- Open wound completely to provide drainage
- Irrigate and repack with moist gauze 2–3 times daily
- Initial healing by secondary intention
- Antibiotics — modify to include antistaphylococcal coverage
- Vancomycin 1 g IV q12h if MRSA confirmed on culture
- In morbidly obese patients: suction wound device to enhance healing
- Secondary closure considered once healthy granulation tissue develops
- Prevention: chlorhexidine skin prep, preoperative antibiotic prophylaxis, clippers (not razor) for hair removal
6. NECROTIZING FASCIITIS
📌 Definition
- A rapidly progressive, life-threatening deep-tissue infection involving subcutaneous tissue and fascia
- Characterised by extensive and rapidly spreading necrosis (gangrene) of skin and underlying structures
- Rare but potentially fatal complication of episiotomy or abdominal wound
🔴 Causes
- Mixed anaerobes + Streptococcus pyogenes
- Portal of entry: surgical incision, episiotomy, or cryptic (no visible entry point)
- Risk factors:
- Insulin-dependent diabetes
- Morbid obesity
- Cancer or immunodeficiency
- Corticosteroid therapy
🟡 Clinical Features
- "Pain out of proportion" to wound appearance — cardinal early sign
- Rapid spread both proximally and distally within 24 hours
- Skin progression:
- Red → Purple → Blue (within 24–48 hrs)
- → Blistering/bullae with clear yellow fluid
- → Frank gangrene by day 4–5
- → Extensive skin sloughing
- High fever, extreme prostration, tachycardia
- Bacteraemia frequently present
- Metastatic abscesses may form
- Elevated creatine phosphokinase (CK) — important clue
- Unexplained tachycardia + marked left shift on CBC
- CT/MRI: soft tissue swelling, no frank gas (not definitive)
- Biopsy with frozen section may confirm
🟢 Management
- SURGICAL EMERGENCY — immediate aggressive action required
- Wide surgical debridement of ALL necrotic tissue — most critical step
- Often requires repeated debridements
- IV antibiotics:
- Clindamycin 900 mg IV q8h (or metronidazole 500 mg IV q12h)
- + Vancomycin 1 g IV q12h
- + Gentamicin 5 mg/kg IV q24h or Aztreonam 1–2 g IV q8h
- Maintain intravascular volume with crystalloid infusions
- Correct electrolyte abnormalities
- ICU admission and haemodynamic monitoring
- Consult experienced general or plastic surgeon
7. URINARY TRACT INFECTION (UTI / PYELONEPHRITIS)
📌 Definition
- Bacterial infection of the lower (cystitis) or upper (pyelonephritis) urinary tract occurring in the puerperium
- Facilitated by catheterisation, bladder trauma, and urinary stasis during labour
🔴 Causes
- Escherichia coli — most common (80%)
- Klebsiella pneumoniae, Proteus mirabilis, Enterococcus
- Predisposing factors: urinary catheterisation, bladder overdistension, perineal trauma, urinary retention
🟡 Clinical Features
- Cystitis: dysuria, frequency, urgency, suprapubic pain, haematuria
- Pyelonephritis: fever, rigors, nausea/vomiting, costovertebral angle tenderness, flank pain
- Urinalysis: pyuria, bacteriuria, ± nitrites positive
- Raised WBC; urine culture confirms organism
🟢 Management
- Mid-stream urine (MSU) culture and sensitivity before starting antibiotics
- Cystitis: oral nitrofurantoin, trimethoprim, or cefalexin — 5–7 days
- Pyelonephritis: IV cephalosporin (ceftriaxone) or gentamicin
- Adequate oral/IV hydration
- Monitor for septicaemia
- Follow-up urine culture to confirm clearance
8. PERINEAL / EPISIOTOMY INFECTION
📌 Definition
- Infection of the perineal body or episiotomy repair site characterised by wound breakdown, cellulitis, or abscess formation in the postpartum period
🔴 Causes
- Staphylococcus aureus, E. coli, mixed anaerobes, GBS
- Predisposing factors: haematoma formation, poor tissue apposition, prolonged labour, obesity, anaemia, immunosuppression
🟡 Clinical Features
- Perineal pain, swelling, purulent discharge from wound
- Wound dehiscence (wound edges separating)
- Foul-smelling discharge
- Fever
- Risk of extension to deeper fascia → necrotizing fasciitis
🟢 Management
- Wound debridement and opening of infected area
- Broad-spectrum antibiotics (covering gram-positives, gram-negatives, and anaerobes)
- Perineal hygiene — sitz baths, regular cleaning
- Delayed secondary repair after infection completely resolved
- Monitor for necrotizing fasciitis
SECTION 2: HAEMORRHAGIC PUERPERAL DISORDERS
9. PRIMARY POSTPARTUM HAEMORRHAGE (PPH)
📌 Definition
- Blood loss > 500 mL after vaginal delivery or > 1000 mL after caesarean delivery
- Occurring within the first 24 hours of delivery
- Most common complication of labour and delivery
- Accounts for up to 11% of obstetric deaths
🔴 Causes — "The Four Ts"
| T | Cause | Frequency |
|---|---|---|
| Tone | Uterine atony | 75–90% |
| Trauma | Genital tract lacerations | ~20% |
| Tissue | Retained placental fragments | ~10% |
| Thrombin | Coagulopathy | Uncommon |
- Uterine atony risk factors: multiple gestation, fetal macrosomia, polyhydramnios, prolonged labour, chorioamnionitis, tocolytics, halogenated anaesthetic agents, multiparity
- Note: maternal plasma volume expansion means shock may not appear until > 1500 mL blood lost
🟡 Clinical Features
- Heavy, continuous vaginal bleeding
- Soft, boggy, enlarged uterus (atony)
- Visible perineal/vaginal/cervical tears (trauma)
- Signs of haemorrhagic shock: pallor, tachycardia, hypotension, cold clammy skin, reduced consciousness
- Failure to deliver placenta within 30 minutes (retained placenta)
🟢 Management
Step-wise escalation:
- Bimanual uterine massage — stimulates contractions
- Uterotonics:
- Oxytocin 10 units IM immediately after delivery → IV infusion up to 40 units
- Carboprost (prostaglandin F2α)
- Misoprostol 800 mcg rectally
- Ergometrine (avoid in hypertension)
- IV fluids and blood transfusion — O-negative in emergency
- Balloon tamponade (intrauterine balloon)
- Surgical:
- B-Lynch compression suture
- Uterine artery ligation
- Internal iliac artery ligation
- Emergency peripartum hysterectomy — last resort
- Interventional radiology — uterine artery embolisation
- Repair lacerations with absorbable suture
- Manual removal of retained placenta
10. SECONDARY POSTPARTUM HAEMORRHAGE
📌 Definition
- Abnormal or excessive uterine bleeding occurring between 24 hours and 6 weeks postpartum
🔴 Causes
- Retained placental fragments — most common
- Subinvolution of placental site
- Endometritis
- Uterine arteriovenous malformation
- Coagulopathy (rare)
🟡 Clinical Features
- Heavy vaginal bleeding after initial normal recovery
- Uterine tenderness if infection coexists
- ± Offensive lochia
- Fever if endometritis present
- USS: echogenic material in uterine cavity (retained products)
🟢 Management
- Oxytocics (ergometrine, oral misoprostol)
- Antibiotics if infection present
- USS-guided surgical uterine evacuation (ERPC) if retained products confirmed
- Blood transfusion if severe haemorrhage
- Follow-up USS to confirm clearance
11. UTERINE INVERSION
📌 Definition
- Rare but life-threatening condition where the uterine fundus collapses into or beyond the uterine cavity
- Occurs during the third stage of labour
🔴 Causes
- Mismanaged third stage — cord traction before placental separation
- Excessive fundal pressure (Credé manoeuvre)
- Fundal placentation
- Short umbilical cord
- Uterine atony
- Connective tissue disorders (rare)
🟡 Clinical Features
- Sudden severe abdominal pain
- Heavy haemorrhage
- Failure to palpate uterine fundus abdominally — key sign
- Visible or palpable mass at cervix, vaginal introitus, or protruding externally
- Profound haemorrhagic shock — often disproportionate to visible blood loss (vasovagal mechanism)
🟢 Management
- Do NOT remove placenta if still attached (causes massive haemorrhage)
- Manual replacement — Johnson manoeuvre:
- Push fundus upward through cervix with palm
- Apply steady continuous pressure
- Tocolytics to relax uterus: terbutaline, magnesium sulphate, or nitroglycerin
- IV fluids and blood transfusion
- Hydrostatic method (O'Sullivan technique) — warm saline into vagina under pressure
- Surgical correction (Huntington/Haultain procedure) if manual replacement fails
- Oxytocics only AFTER successful replacement
12. UTERINE RUPTURE
📌 Definition
- A full-thickness disruption of all layers of the uterine wall
- A life-threatening obstetric emergency occurring during labour or early postpartum
🔴 Causes
- Previous uterine scar — LSCS (most common), myomectomy
- Obstructed labour
- Oxytocin misuse (excessive stimulation)
- Grand multiparity (thin myometrium)
- Uterine trauma
- Congenital uterine anomaly
🟡 Clinical Features
- Sudden severe abdominal pain — often with sudden cessation of contractions
- Fetal parts palpable outside uterus abdominally
- Fetal heart rate abnormalities or sudden loss of fetal heart rate
- Maternal haemorrhagic shock
- Vaginal bleeding (may be minimal if intraperitoneal)
- Scar tenderness before rupture (impending rupture)
- Recession of presenting part on vaginal examination
🟢 Management
- Emergency laparotomy — immediate
- Uterine repair (if feasible and patient desires future fertility)
- Peripartum hysterectomy — if repair not possible or bleeding uncontrollable
- Massive blood transfusion protocol
- ICU admission post-operatively
- Neonatal resuscitation team on standby
SECTION 3: THROMBOEMBOLIC PUERPERAL DISORDERS
13. DEEP VEIN THROMBOSIS (DVT)
📌 Definition
- Formation of a thrombus within the deep venous system (typically femoral or iliac veins)
- Puerperium is a high-risk period due to Virchow's triad
🔴 Causes — Virchow's Triad
- Stasis: immobility, bedrest, prolonged labour, C-section
- Hypercoagulability: increased clotting factors during pregnancy (I, VII, VIII, X, XII, vWF); decreased Protein S
- Vessel injury: pelvic/surgical trauma during delivery
- Additional risk factors: obesity, dehydration, prior VTE, thrombophilia, age > 35
🟡 Clinical Features
- Unilateral leg pain, swelling, warmth, erythema
- Pitting oedema of affected limb
- ± Homans sign (calf pain on dorsiflexion — unreliable)
- Low-grade fever
- Doppler USS — confirms diagnosis
🟢 Management
- Low Molecular Weight Heparin (LMWH) — enoxaparin (first-line, safe in breastfeeding)
- Graduated compression stockings
- Early mobilisation
- Adequate hydration
- Convert to warfarin after 6 weeks if not breastfeeding
- Minimum treatment duration: 3–6 months
- Screen for underlying thrombophilia (antiphospholipid syndrome, Factor V Leiden, etc.)
14. PULMONARY EMBOLISM (PE)
📌 Definition
- Life-threatening obstruction of pulmonary arterial circulation by a dislodged thrombus
- Most commonly arises from pelvic or femoral DVT in the puerperium
- A leading cause of direct maternal mortality
🔴 Causes
- Dislodged DVT from pelvic or leg veins
- Hypercoagulable puerperal state
- Immobility post-C-section
- Prior VTE history
- Thrombophilia
🟡 Clinical Features
- Sudden onset dyspnoea — most common symptom
- Pleuritic chest pain
- Haemoptysis
- Tachycardia, hypoxia
- ± Syncope/collapse (massive PE)
- Raised D-dimer (limited utility in postpartum)
- ABG: hypoxia + hypocapnia (type 1 respiratory failure)
- ECG: sinus tachycardia; S1Q3T3 pattern (classic but rare)
- CTPA — diagnostic gold standard
🟢 Management
- LMWH or unfractionated heparin — immediate anticoagulation
- Thrombolysis (alteplase) — if massive PE with haemodynamic instability
- Oxygen supplementation
- ICU admission for massive PE
- Surgical embolectomy — rare, last resort
- Long-term anticoagulation for 3–6 months
15. SEPTIC PELVIC THROMBOPHLEBITIS
📌 Definition
- Thrombosis of the ovarian or pelvic veins superimposed with bacterial infection
- Complicates < 1% of puerperal endometritis cases
- Presents as two distinct clinical forms:
- Acute ovarian vein thrombosis
- "Enigmatic fever" — persistent fever with no localising signs
🔴 Causes
- Extension of endometritis causing septic thrombus in pelvic/ovarian veins
- Common organisms: E. coli, Bacteroides, mixed gram-negative anaerobes
🟡 Clinical Features
- Persistent/spiking fever despite adequate antibiotic therapy — hallmark sign
- Flank or lower abdominal pain
- ± Palpable tender mass (ovarian vein thrombosis form)
- No other identifiable source of persistent fever
- CT scan may show thrombus in ovarian/pelvic vein
🟢 Management
- IV heparin anticoagulation + continued broad-spectrum antibiotics
- Fever typically resolves within 24–48 hours — this therapeutic response confirms the diagnosis
- Continue antibiotics until afebrile
- Long-term anticoagulation for 4–6 weeks debated
16. CEREBRAL VENOUS THROMBOSIS (CVT)
📌 Definition
- Aseptic thrombosis of the cerebral venous sinuses (most commonly superior sagittal sinus)
- Occurs in the hypercoagulable puerperal state
🔴 Causes
- Puerperal hypercoagulability
- Dehydration
- Sepsis
- Thrombophilia (antiphospholipid antibodies, Factor V Leiden)
- Prior OCP use
🟡 Clinical Features
- Progressive headache worsening over several days — earliest and most common symptom
- Behavioural or personality change
- Focal neurological deficits
- Convulsive seizures
- Papilloedema (raised ICP)
- ± Focal motor deficits, aphasia
- ± Coma in severe cases
🟢 Management
- Anticoagulation with LMWH or heparin — even if haemorrhagic infarct present
- Antiepileptics for seizures
- ICP management (head elevation, mannitol if needed)
- MRI/MRV — diagnostic gold standard (CT may miss early CVT)
- Long-term anticoagulation for 3–12 months
- Screen for thrombophilia
SECTION 4: PUERPERAL PSYCHIATRIC DISORDERS
17. POSTPARTUM BLUES ("BABY BLUES")
📌 Definition
- A mild, transient, self-limiting mood disturbance affecting up to 65% of mothers
- Arises in the first week postpartum and resolves spontaneously within 2 weeks
- Considered a normal physiological response — NOT a psychiatric disorder
🔴 Causes
- Rapid postpartum fall in oestrogen and progesterone
- Sleep deprivation
- Psychological adjustment to new maternal role
- Emotional vulnerability in the perinatal period
🟡 Clinical Features
- Onset: day 2–5 postpartum (correlates with peak hormonal withdrawal)
- Tearfulness — most characteristic feature
- Mood lability and emotional sensitivity
- Mild anxiety and irritability
- Fatigue
- Mild insomnia
- No functional impairment
- No psychotic features
- Symptoms mild and intermittent
🟢 Management
- Reassurance and emotional support — only intervention needed
- Psychoeducation of mother and partner
- No pharmacotherapy required
- Encourage adequate rest and sleep
- Monitor: if symptoms persist beyond 2 weeks → screen for postpartum depression
18. POSTPARTUM DEPRESSION (PPD)
📌 Definition
- A major depressive episode occurring during pregnancy or within 4 weeks of delivery (DSM-5)
- Affects 3–6% of women (major depression); broader postpartum depressive symptoms in up to 10–15%
- DSM-5 specifier: "with peripartum onset"
🔴 Causes
- Rapid hormonal shifts (oestrogen/progesterone/allopregnanolone withdrawal)
- HPA axis dysregulation
- Prior history of depression or bipolar disorder (strongest risk factor)
- Poor social support and social isolation
- Stressful life events
- Sleep deprivation and exhaustion
- Relationship difficulties
- Unplanned pregnancy
- Postpartum thyroid dysfunction
🟡 Clinical Features
- Persistent low mood for > 2 weeks
- Anhedonia — loss of interest or pleasure
- Excessive guilt, worthlessness, hopelessness
- Cognitive impairment — poor concentration, indecisiveness
- Sleep disturbance beyond that attributable to infant care
- Fatigue and loss of energy
- Poor bonding with infant — important clinical feature
- Anxiety and panic symptoms (common in postpartum depression)
- Suicidal ideation in severe cases
- No psychotic features (distinguishes from postpartum psychosis)
🟢 Management
- Screen using Edinburgh Postnatal Depression Scale (EPDS) — score ≥ 13 is positive
- Mild-to-moderate:
- Psychotherapy — cognitive-behavioural therapy (CBT), interpersonal therapy (IPT)
- Peer support groups
- Social support enhancement
- Moderate-to-severe:
- SSRIs — Sertraline (first-line — safest in breastfeeding)
- Paroxetine (second-line)
- Brexanolone IV (neuroactive steroid — FDA-approved for PPD)
- Psychiatric referral if severe or suicidal
- Father/partner screening — fathers also at risk of PPD
19. POSTPARTUM PSYCHOSIS
📌 Definition
- The most severe puerperal psychiatric disorder
- Acute onset psychosis within the first 2 weeks postpartum (often days 3–5)
- Affects 1–2 per 1000 deliveries
- A psychiatric emergency with significant risk of infanticide and maternal suicide
🔴 Causes
- Bipolar disorder — strongest risk factor (20–50× increased risk)
- Prior postpartum psychotic episode (50% recurrence risk)
- Family history of bipolar disorder or postpartum psychosis
- First-time motherhood
- Sudden oestrogen and progesterone withdrawal
- Severe sleep deprivation
- Dopaminergic system dysregulation
🟡 Clinical Features
- Onset: first 2 weeks (most commonly days 3–5)
- Confusion and disorientation — often the earliest sign
- Command auditory hallucinations (to harm infant or self)
- Delusions (often about the infant — e.g., baby is evil, possessed, or must be saved)
- Rapidly fluctuating mood (manic, depressed, mixed)
- Bizarre behaviour, agitation, restlessness
- Severe insomnia
- Risk of infanticide — always assess
- Risk of maternal suicide
- May appear superficially well between episodes ("lucid intervals")
🟢 Management
- PSYCHIATRIC EMERGENCY — immediate action required
- Urgent psychiatric hospital admission
- Never leave mother alone with the infant — safeguarding priority
- Antipsychotics:
- Haloperidol, olanzapine, quetiapine
- Lithium — treatment of choice for bipolar-related postpartum psychosis
- Benzodiazepines for acute agitation
- ECT (Electroconvulsive Therapy) — highly effective if refractory
- Mother-and-baby unit (MBU) admission — if available, maintains mother-infant bond
- Discontinue breastfeeding if medication unsafe for infant
- Psychoeducation of family
SECTION 5: OTHER PUERPERAL COMPLICATIONS
20. POSTPARTUM URINARY RETENTION
📌 Definition
- Inability to void spontaneously within 6 hours of delivery
- Due to impaired bladder function from perineal and bladder trauma during labour
🔴 Causes
- Perineal oedema compressing urethra
- Pain inhibiting micturition reflex
- Epidural anaesthesia impairing bladder sensation
- Bladder overdistension during prolonged labour
- Regional anaesthesia (spinal/epidural)
- Perineal trauma or haematoma
🟡 Clinical Features
- Inability to void despite urge
- Suprapubic fullness and discomfort
- Bladder palpable/percussible above pubic symphysis
- ± Overflow incontinence (dribbling of urine)
- Bladder scan/USS: post-void residual > 150 mL confirms retention
🟢 Management
- Intermittent clean catheterisation — preferred
- Indwelling catheter if unable to void repeatedly
- Adequate analgesia
- Trial of voiding after 24–48 hours
- Pelvic floor physiotherapy
- Monitor closely for associated UTI
21. BREAST ENGORGEMENT
📌 Definition
- Painful bilateral overfilling of the breasts with milk due to inadequate milk removal
- Typically occurring on days 3–5 postpartum
- A physiological problem, not infection
🔴 Causes
- Inadequate milk removal
- Infant separation from mother
- Sore or cracked nipples preventing proper feeding
- Improper breastfeeding technique/poor latch
- Sudden cessation of breastfeeding
- Milk stasis
🟡 Clinical Features
- Onset: day 3–5 postpartum
- Bilateral painful, hard, enlarged breasts
- Warmth and skin tightness
- ± Low-grade fever (< 38.5°C)
- Nausea
- Compressed, flattened nipple-areola complex → difficulty with infant latch
- Distinguish from mastitis: bilateral, no systemic features, resolves with feeding
🟢 Management
- Frequent breastfeeding or pumping to empty breasts
- Correct latch technique — most important intervention
- Warm compresses before feeding to facilitate let-down
- Cold compresses after feeding to reduce oedema
- Manual massage to facilitate milk release
- Analgesics — ibuprofen, paracetamol
- Cabbage leaf application — evidence limited but commonly used
22. SUBINVOLUTION OF THE UTERUS
📌 Definition
- Failure of the puerperal uterus to return to its normal pre-pregnant size within the expected timeframe (usually by 6 weeks)
- Due to incomplete physiological regression of the uterus
🔴 Causes
- Retained placental fragments — most common
- Endometritis (infection prevents normal involution)
- Uterine fibroids
- Polyhydramnios
- Multiple gestation
- Grand multiparity
- Prolonged labour
🟡 Clinical Features
- Uterus larger and softer than expected for postpartum day
- Prolonged or excessive lochia (lochia persisting beyond normal)
- ± Offensive/purulent lochia if endometritis coexists
- ± Pelvic pain and heaviness
- Fever if infection present
- USS confirms enlarged uterus ± echogenic material
🟢 Management
- Oxytocics: ergometrine tablets, oral misoprostol
- Antibiotics if infection (endometritis) coexists
- Ultrasound-guided ERPC (Evacuation of Retained Products of Conception) if retained products confirmed
- Follow-up USS to confirm complete involution
- Monitor for secondary PPH
23. POSTPARTUM THYROIDITIS
📌 Definition
- An autoimmune inflammatory thyroid condition occurring within the first year postpartum
- Characterised by a transient hyperthyroid phase followed by a hypothyroid phase
- Affects approximately 5–10% of postpartum women
🔴 Causes
- Autoimmune rebound following postpartum reversal of pregnancy-induced immune tolerance
- Anti-TPO (anti-thyroid peroxidase) antibody positivity — primary marker
- Underlying Hashimoto's thyroiditis — predisposing condition
- Genetic predisposition (HLA-DR3/DR5)
- Type 1 diabetes mellitus — associated risk
🟡 Clinical Features
- Phase 1 — Hyperthyroid (months 1–4):
- Fatigue, palpitations, tremor, anxiety
- Heat intolerance, sweating
- Weight loss
- TSH low, free T4 elevated
- Phase 2 — Hypothyroid (months 4–8):
- Fatigue, cold intolerance, constipation
- Weight gain, dry skin, hair loss
- Depression (may mimic/exacerbate PPD)
- TSH elevated, free T4 low
- Phase 3 — Recovery (by 12–18 months): majority recover
- ~25% develop permanent hypothyroidism
🟢 Management
- Hyperthyroid phase:
- Beta-blockers (propranolol) for symptomatic relief
- Do NOT use antithyroid drugs (carbimazole/PTU) — destructive process, not Graves'
- Hypothyroid phase:
- Levothyroxine replacement therapy
- Especially important if breastfeeding or planning further pregnancy
- Monitor TFTs every 3–6 months
- Annual TFT screening — 25% risk of permanent hypothyroidism
- Screen for PPD — hypothyroid phase can precipitate depressive episodes
24. PUERPERAL / POSTPARTUM ECLAMPSIA
📌 Definition
- Occurrence of grand mal tonic-clonic seizures in a woman with pre-eclampsia or de novo hypertension
- Arising within 48 hours postpartum (occasionally up to 4 weeks postpartum)
- Without other neurological cause (e.g., epilepsy, meningitis)
🔴 Causes
- Persistence of severe hypertension postpartum
- New-onset hypertension after delivery (de novo)
- Cerebral vasospasm
- Endothelial dysfunction (hallmark of pre-eclampsia pathophysiology)
- Failure of pre-eclampsia to resolve after delivery
- Cerebral oedema
🟡 Clinical Features
- Grand mal tonic-clonic seizures
- Severe headache (frontal/occipital)
- Visual disturbances — blurring, scotomata, flashing lights, diplopia
- Hypertension — BP ≥ 160/110 mmHg
- Proteinuria (≥ 2+ on dipstick)
- Facial and peripheral oedema
- Epigastric/right upper quadrant pain (liver involvement)
- ± HELLP syndrome (Haemolysis, Elevated Liver enzymes, Low Platelets)
- Altered consciousness after seizure (postictal state)
🟢 Management
- IV Magnesium Sulphate — treatment of choice
- Loading dose: 4–6 g IV over 15–20 minutes
- Maintenance: 1–2 g/hr IV infusion
- Monitor: urine output, reflexes, respiratory rate (toxicity signs)
- Antidote: Calcium gluconate 10 mL of 10% IV if toxicity occurs
- Antihypertensives:
- IV Labetalol (first-line)
- IV Hydralazine
- Oral Nifedipine (if IV access difficult)
- Strict fluid balance monitoring (restrict IV fluids — risk of pulmonary oedema)
- Oxygen supplementation
- ICU/HDU admission
- Rectal diazepam for breakthrough seizures
- Continue MgSO₄ for 24 hours after last seizure
MASTER SUMMARY — ALL 24 DISORDERS AT A GLANCE
| # | Disorder | Section | Key Definition | Key Cause | Key Feature | Key Treatment |
|---|---|---|---|---|---|---|
| 1 | Puerperal Sepsis | Infection | GAS bacteraemia postpartum | S. pyogenes | Fever + hypotension | IV Penicillin G |
| 2 | Endometritis | Infection | Uterine infection within 10 days | Polymicrobial ascending | Malodorous lochia | Clindamycin + Gentamicin |
| 3 | Mastitis | Infection | Breast parenchymal infection | S. aureus | Tender red breast, 2nd week | Antistaphylococcal antibiotics |
| 4 | Breast Abscess | Infection | Localised pus in breast | S. aureus/MRSA | Discrete fluctuant mass on USS | USS-guided drainage |
| 5 | Wound Infection | Infection | Incision infection post-LSCS | S. aureus/MRSA | Pus at incision | Open, drain, antibiotics |
| 6 | Necrotizing Fasciitis | Infection | Rapidly spreading deep necrosis | Mixed anaerobes + GAS | Pain out of proportion + gangrene | Emergency debridement |
| 7 | UTI/Pyelonephritis | Infection | Urinary tract bacterial infection | E. coli | Dysuria/flank pain | Antibiotics per culture |
| 8 | Perineal Infection | Infection | Episiotomy/perineal wound infection | Mixed organisms | Wound dehiscence + discharge | Debridement + antibiotics |
| 9 | Primary PPH | Haemorrhage | >500 mL blood loss within 24 hrs | Uterine atony (75–90%) | Boggy uterus + heavy bleeding | Oxytocin + massage |
| 10 | Secondary PPH | Haemorrhage | Heavy bleeding 24 hrs–6 weeks | Retained products | Echogenic material on USS | Oxytocics ± evacuation |
| 11 | Uterine Inversion | Haemorrhage | Fundus collapses into cavity | Mismanaged 3rd stage | No fundus palpable | Johnson manoeuvre |
| 12 | Uterine Rupture | Haemorrhage | Full-thickness uterine wall breach | Previous LSCS scar | Fetal parts outside uterus | Emergency laparotomy |
| 13 | DVT | Thromboembolism | Deep venous thrombus | Virchow's triad | Unilateral leg swelling | LMWH |
| 14 | Pulmonary Embolism | Thromboembolism | Pulmonary artery obstruction | Dislodged pelvic DVT | Sudden dyspnoea + hypoxia | LMWH / thrombolysis |
| 15 | Septic Pelvic Thrombophlebitis | Thromboembolism | Infected pelvic vein thrombosis | Endometritis extension | Fever despite antibiotics | Heparin + antibiotics |
| 16 | Cerebral Venous Thrombosis | Thromboembolism | Cerebral sinus thrombosis | Puerperal hypercoagulability | Worsening headache + seizures | Heparin + MRI/MRV |
| 17 | Baby Blues | Psychiatric | Transient mild mood change | Hormonal withdrawal | Tearfulness day 2–5 | Reassurance only |
| 18 | Postpartum Depression | Psychiatric | Major depressive episode | Hormonal + psychosocial | Sustained low mood + poor bonding | SSRI + psychotherapy |
| 19 | Postpartum Psychosis | Psychiatric | Acute psychosis with infanticide risk | Bipolar disorder | Hallucinations within 2 weeks | Emergency hospitalisation |
| 20 | Urinary Retention | Other | Inability to void within 6 hrs | Bladder trauma + anaesthesia | Suprapubic fullness | Catheterisation |
| 21 | Breast Engorgement | Other | Bilateral painful milk overfilling | Poor milk removal | Bilateral hard painful breasts | Frequent emptying + correct latch |
| 22 | Subinvolution | Other | Failure of uterine regression | Retained products/infection | Uterus larger than expected | Ergometrine ± evacuation |
| 23 | Postpartum Thyroiditis | Other | Autoimmune biphasic thyroid disorder | Anti-TPO antibodies | Hyper then hypothyroid phases | Beta-blockers / Levothyroxine |
| 24 | Puerperal Eclampsia | Other | Post-delivery seizures + hypertension | Persistent pre-eclampsia | Seizures + BP ≥160/110 | IV Magnesium sulphate |
Sources: Creasy & Resnik's Maternal-Fetal Medicine • Rosen's Emergency Medicine • Tintinalli's Emergency Medicine • Goldman-Cecil Medicine • Kaplan & Sadock's Comprehensive Textbook of Psychiatry • Adams & Victor's Principles of Neurology • Berek & Novak's Gynecology
Present important puerperial disorder for 10 mark which is mostly asked in exams
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.