Supra and infra orbital nerve supplies which muscles
Supraorbital and Infraorbital Nerves - Muscle Supply
Supraorbital Nerve
- Origin: Branch of the frontal nerve, which is a branch of the ophthalmic division (V1) of the trigeminal nerve
- Sensory territory only:
- Skin of the forehead and scalp (up to the vertex)
- Upper eyelid skin and conjunctiva
- Bridge of the nose
- Frontal sinus mucosa
- Exits through the supraorbital notch/foramen
Infraorbital Nerve
- Origin: Terminal branch of the maxillary division (V2) of the trigeminal nerve; exits through the infraorbital foramen
- Sensory territory only:
- Lower eyelid skin
- Medial cheek
- Nasal ala (side of nose)
- Upper lip
- Upper teeth and gums
- Nasal mucosa
Why No Muscle Supply?
The key distinction: Facial nerve (CN VII) supplies the muscles of facial expression (including orbicularis oculi and frontalis in the periorbital region). These muscles are anatomically close to the supraorbital and infraorbital nerves, which often leads to confusion in exam questions - but the nerve supply to those muscles is CN VII, not CN V branches.
Hey ai
I want to make uh clear the I am an mbbs student and whatever I asked to uh please answer it correctly and give answer fast and give answer with full explaination along with clinical and all …! Understand?
- Accurate answers pulled from authoritative medical textbooks (Gray's Anatomy, Robbins Pathology, Harrison's, Guyton, etc.) in my library
- Full explanations - not just facts, but why things work the way they do
- Clinical correlations - signs, symptoms, syndromes, applied anatomy, clinical scenarios, exam-relevant points
- Fast responses - I search multiple sources in parallel
In few time I will send uh my all history that I searched in other ai apps.. after now I will use uh only ok…!
Course of facial nerve with diagrams
facial nerve course diagram MBBS anatomy intracranial intratemporal extracranial
Course of the Facial Nerve (CN VII) - Complete MBBS Guide
Overview
| Component | Function |
|---|---|
| Special Visceral Efferent (SVE) | Motor to muscles of facial expression (main function) |
| General Visceral Efferent (GVE) | Parasympathetic - lacrimal, submandibular, sublingual, nasal glands |
| Special Visceral Afferent (SVA) | Taste - anterior 2/3 of tongue |
| General Somatic Afferent (GSA) | Sensation - skin of EAC, auricle, mastoid |
| General Visceral Afferent (GVA) | Mucosa of nose, pharynx, palate |
Nuclei (Origin in Brainstem)
| Nucleus | Function |
|---|---|
| Motor nucleus (lateral tegmentum, caudal pons) | Motor to facial muscles |
| Superior salivatory nucleus (pons) | Parasympathetic - submandibular & sublingual glands |
| Lacrimal nucleus (pons) | Parasympathetic - lacrimal gland |
| Nucleus tractus solitarius (pons/medulla) | Taste - anterior 2/3 tongue |
Key anatomy point: The facial nerve fascicles loop dorsally around the abducens nucleus (CN VI) before exiting - this forms the facial colliculus on the floor of the 4th ventricle. That is why a pontine lesion affecting CN VI often also affects CN VII.
Complete Course - 3 Segments
SEGMENT 1: INTRACRANIAL COURSE
- Nerve exits the ventrolateral pons (at the pontomedullary junction) as two roots:
- Motor root (larger) - facial expression muscles
- Nervus intermedius (sensory + parasympathetic root)
- Both roots cross the cerebellopontine angle (CPA)
- Enter the internal auditory meatus (IAM) together with CN VIII (vestibulocochlear nerve)
SEGMENT 2: INTRATEMPORAL COURSE (Inside the Fallopian/Facial Canal)

A. Meatal Segment (8-10 mm)
- Runs in the superior anterior quadrant of the IAC (above CN VIII)
- No branches arise here
B. Labyrinthine Segment (3-5 mm) - SHORTEST & NARROWEST
- Runs anterolaterally above the cochlea
- Reaches the geniculate ganglion (contains cell bodies of sensory fibers)
- Branch given off: Greater Superficial Petrosal Nerve (GSPN)
- Carries preganglionic parasympathetic fibers → pterygopalatine ganglion → lacrimal gland + nasal/palatal glands
- Also carries taste from palate
- First genu (bend) occurs here - nerve turns sharply posteriorly
C. Horizontal (Tympanic) Segment (8-11 mm)
- Runs along the medial wall of middle ear
- Lies above the oval window, below the lateral semicircular canal
- No major branches arise here
- Second genu occurs at the end - nerve turns inferiorly
D. Mastoid (Vertical) Segment (10-14 mm) - LONGEST intratemporal segment
-
Runs vertically downward in the mastoid
-
Branches given off:
- Nerve to Stapedius (near the upper end) - smallest muscle in the body
- Chorda Tympani - crosses middle ear medial to malleus handle, exits via petrotympanic fissure, joins lingual nerve (V3)
- Carries: taste (anterior 2/3 tongue) + parasympathetic to submandibular & sublingual glands
-
Nerve exits via Stylomastoid Foramen
SEGMENT 3: EXTRACRANIAL COURSE
| Branch | Supply |
|---|---|
| Posterior auricular nerve | Occipitalis, posterior auricular muscle, transverse & oblique auricular muscles |
| Nerve to posterior belly of digastric | Posterior belly of digastric |
| Nerve to stylohyoid | Stylohyoid muscle |
- Temporal branch - frontalis, orbicularis oculi (upper), corrugator supercilii
- Zygomatic branch - orbicularis oculi (lower), zygomaticus
- Buccal branch - buccinator, orbicularis oris, nasalis
- Marginal mandibular branch - depressor anguli oris, depressor labii inferioris, mentalis
- Cervical branch - platysma
Mnemonic for 5 terminal branches: "Two Zebras Bit My Cat" - Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical
Summary Diagram (All Branches)
PONS (Motor nucleus + Superior salivatory nucleus)
↓
Cerebellopontine Angle (CPA)
↓
Internal Auditory Meatus (with CN VIII)
↓
FALLOPIAN CANAL:
Labyrinthine segment → GSPN → Pterygopalatine ganglion → Lacrimal gland
Geniculate ganglion (1st genu)
↓
Horizontal/Tympanic segment (2nd genu)
↓
Mastoid/Vertical segment:
→ Nerve to Stapedius
→ Chorda Tympani → Lingual nerve → submandibular/sublingual glands + taste
↓
STYLOMASTOID FORAMEN
↓
→ Posterior auricular nerve
→ Nerve to posterior digastric
→ Nerve to stylohyoid
↓
PAROTID GLAND (Pes Anserinus)
↓
Temporal | Zygomatic | Buccal | Marginal mandibular | Cervical
Clinical Correlations (HIGH YIELD)
1. Bell's Palsy
- LMN (lower motor neuron) facial palsy - most common cause
- Affects entire half of face (forehead + lower face both affected)
- Due to inflammation of facial nerve in the fallopian canal
- Cannot close eye (lagophthalmos), loss of taste anterior 2/3 tongue, hyperacusis if above stapedius nerve
2. UMN vs LMN Facial Palsy - KEY EXAM TOPIC
| Feature | UMN (above motor nucleus) | LMN (at/below motor nucleus) |
|---|---|---|
| Forehead spared? | YES (bilateral cortical input to upper face) | NO - forehead also affected |
| Eye closure | Preserved | Lost (lagophthalmos) |
| Cause | Stroke, tumor | Bell's palsy, parotid tumor, otitis media |
3. Lesion Localization (Topodiagnosis)
| Level of Lesion | Features |
|---|---|
| Above GSPN (geniculate ganglion) | All features below + reduced lacrimation |
| Above nerve to stapedius | All below + hyperacusis |
| Above chorda tympani | All below + loss of taste anterior 2/3 tongue + dry mouth |
| Below chorda tympani / at stylomastoid foramen | Only motor paralysis - no taste/lacrimation changes |
4. Parotid Surgery Risk
- Parotid tumors/surgery can damage the facial nerve as it passes through the parotid
- Results in ipsilateral facial muscle paralysis
5. Chorda Tympani during middle ear surgery
- Injury during middle ear (tympanoplasty/mastoidectomy) → loss of taste anterior 2/3 tongue + dry mouth
6. House-Brackmann Scale
Send me images of it’s exit from cranium to face
facial nerve exit stylomastoid foramen course to face anatomy diagram
facial nerve intratemporal segments geniculate ganglion labyrinthine tympanic mastoid diagram labeled
Facial Nerve - Visual Journey from Cranium to Face
📍 IMAGE 1 - Intratemporal Segments (Inside the Temporal Bone)

- Lab = Labyrinthine segment (with GSPN branching off)
- Horiz = Horizontal/Tympanic segment
- 2nd genu = The sharp bend where nerve turns downward
- Vert = Vertical/Mastoid segment (with Chorda tympani branching off)
- LSCC/PSCC = Lateral & Posterior Semicircular Canals (surgical landmarks)
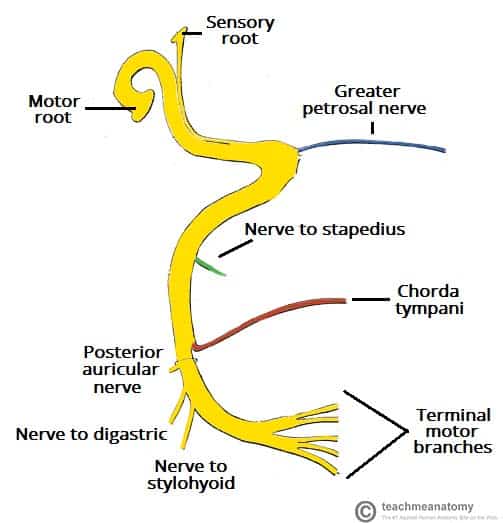
📍 IMAGE 2 - Exit from Stylomastoid Foramen + Branches

- Facial nerve [VII] coursing vertically downward in the mastoid
- Geniculate ganglion at the top (1st genu)
- Greater petrosal nerve (GSPN) heading anteriorly toward pterygopalatine fossa → lacrimal gland
- Nerve to Stapedius (inside pyramidal process)
- Chorda tympani crossing the middle ear
- Exit at Stylomastoid foramen
- Posterior auricular nerve, Digastric branch, Stylohyoid branch after exit
📍 IMAGE 3 - Extracranial Course through Parotid to Face

- Facial nerve (CN VII) emerging just below and in front of the ear
- Posterior auricular nerve going backward
- Nerve to posterior belly of digastric
- Nerve entering the parotid gland
- Dividing into Temporal branches (going upward to forehead)
- Cervical branch going downward to platysma
- Relations with parotid duct, external carotid artery, and neighboring vessels
📍 IMAGE 4 - Full Schematic (Branches + Parasympathetic connections)
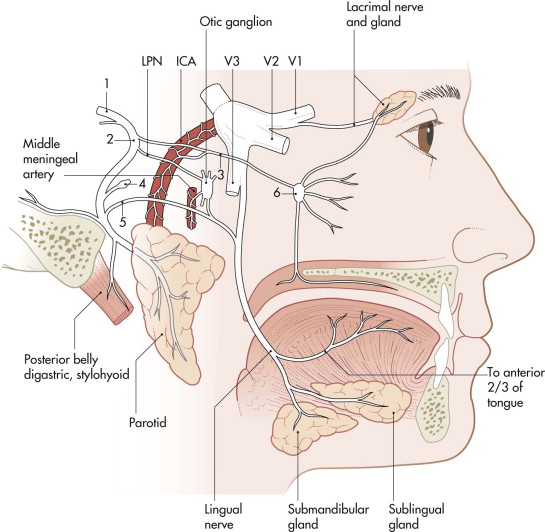
- Complete circuit from the temporal bone all the way to the tongue, submandibular gland, sublingual gland, and lacrimal gland
- Chorda tympani joining the lingual nerve
- Greater petrosal nerve → pterygopalatine ganglion → lacrimal gland
- Parotid and its relationship to the extracranial nerve trunk
📍 IMAGE 5 - Brainstem Origin + Geniculate Ganglion

- Origin from brainstem (pons)
- Traveling to geniculate ganglion inside the temporal bone
- Left panel: full extracranial branching pattern on the face (all 5 terminal branches fanning out)
Quick Recap of the Route:
PONS → CPA → IAC → Labyrinthine segment (GSPN off)
→ Geniculate ganglion (1st genu)
→ Horizontal segment → 2nd genu
→ Mastoid/Vertical segment (Stapedius nerve + Chorda tympani off)
→ STYLOMASTOID FORAMEN (exits skull here)
→ Post. auricular n. + Digastric + Stylohyoid
→ Parotid gland (Pes Anserinus)
→ Temporal | Zygomatic | Buccal | Marginal mandibular | Cervical
Styloid process and mastoid process on human skull both in one image
styloid process mastoid process human skull labeled anatomy image
📍 Image 1 - Right Lateral View (Best labeled image - OpenStax)
- Styloid process - the thin, pointed, downward projection (like a spike/needle) just below the external acoustic meatus
- Mastoid process - the rounded, cone-shaped projection just behind and below the ear
📍 Image 2 - Classic Lateral Skull Diagram
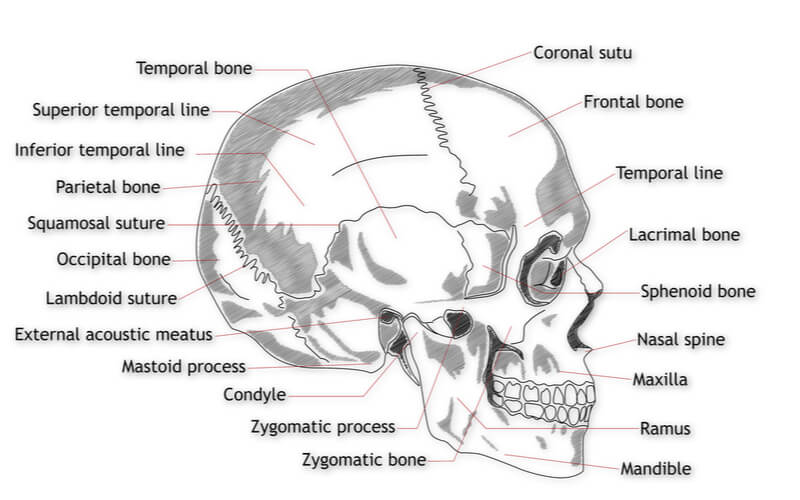
Key Differences to Remember:
| Feature | Styloid Process | Mastoid Process |
|---|---|---|
| Shape | Thin, sharp, needle-like spike | Broad, rounded, cone-shaped |
| Location | Anterior to mastoid, below EAM | Posterior to EAM, behind ear |
| Part of | Temporal bone (styloid part) | Temporal bone (mastoid part) |
| What attaches | Stylohyoid, styloglossus, stylopharyngeus muscles + stylohyoid & stylomandibular ligaments ("bouquet of Riolán") | Sternocleidomastoid, splenius capitis, longissimus capitis muscles |
| Facial nerve relation | Stylomastoid foramen lies between both - facial nerve exits here | Facial nerve exits between styloid & mastoid |
| Clinical | Eagle's syndrome (elongated styloid) | Mastoiditis (infection), surgical landmark |
Mnemonic for styloid attachments: "S-S-S + 2 Ligaments" - Stylohyoid muscle, Styloglossus muscle, Stylopharyngeus muscle + Stylohyoid ligament + Stylomandibular ligament
Function of stapedius muscle
Stapedius Muscle - Complete Guide
Basic Facts
| Feature | Detail |
|---|---|
| Location | Inside the pyramidal eminence on the posterior wall of middle ear |
| Attachment | Tendon inserts onto the neck of stapes |
| Nerve supply | Facial nerve (CN VII) - branch from mastoid/vertical segment |
| Size | Smallest skeletal muscle in the human body (~6 mm) |
| Blood supply | Stapedial artery (branch of posterior auricular artery) |
Functions (EXAM HIGH YIELD)
1. 🔊 Acoustic (Stapedius) Reflex - PRIMARY FUNCTION
- When a loud sound (>70-80 dB) is detected, the stapedius reflexly contracts
- Contraction pulls the annular ligament at the stapes footplate
- This stiffens the ossicular chain → increases middle ear impedance
- Result: attenuates (reduces) sound transmission to the cochlea
- Specifically dampens low-frequency sounds more than high frequencies
- This protects the delicate hair cells of the cochlea from damage by intense sounds
2. 🎙️ Pre-vocalization Reflex (Self-protection)
- Stapedius contracts just before you speak
- Protects the cochlea from your own voice (which travels via bone conduction to the inner ear)
- That's why your voice sounds different on a recording - you normally hear it dampened by this reflex
3. 🎵 High-pass Filtering / Speech Preservation
- By attenuating loud, low-frequency background noise, the stapedius reflex preserves speech-frequency sounds from being masked
- Acts as a biological noise-canceller to improve speech intelligibility in loud environments
4. Anti-masking
- Prevents intense background noise from masking high-frequency speech signals
The Acoustic Reflex Arc (Important for exams!)
Loud sound
↓
Cochlear hair cells
↓
Cochlear nerve (CN VIII) - AFFERENT
↓
Cochlear nuclei → Superior olivary complex (bilateral)
↓
Facial nerve motor nucleus (CN VII) - both sides
↓
Facial nerve (CN VII) → Nerve to Stapedius - EFFERENT
↓
Stapedius muscle contracts (BILATERAL)
↓
Stapes stiffened → reduced cochlear stimulation
Key point: The reflex is bilateral - loud sound in one ear causes stapedius contraction in both ears (ipsilateral and contralateral). This is used diagnostically in audiology.
Stapedius vs Tensor Tympani - Comparison
| Feature | Stapedius | Tensor Tympani |
|---|---|---|
| Nerve | CN VII (Facial) | CN V3 (Mandibular) |
| Ganglion relay | None direct | Via otic ganglion |
| Attaches to | Neck of stapes | Manubrium of malleus |
| Action | Pulls stapes posteriorly | Pulls malleus anteriorly/medially |
| Dominant in acoustic reflex? | YES - primary muscle | No - minimal response to sound |
| Responds to? | Loud sounds | Startle, tactile stimulation of face, swallowing |
| Length | ~6 mm | ~25 mm |
Clinical Correlations (HIGH YIELD)
1. Hyperacusis in Bell's Palsy / Facial Nerve Palsy
- Facial nerve damaged above the nerve to stapedius
- Stapedius is paralyzed → no damping of loud sounds
- Patient experiences hyperacusis (sounds perceived as abnormally loud/painful)
- This is used in topodiagnosis of facial nerve lesions:
- Lesion above nerve to stapedius → hyperacusis present
- Lesion below nerve to stapedius → hyperacusis absent
2. Acoustic Reflex Testing (Tympanometry)
- Used in audiology to test facial nerve integrity and hearing loss type
- Absent reflex can indicate: CN VII palsy, CN VIII damage, otosclerosis, middle ear effusion
- Reflex decay suggests retrocochlear pathology (e.g. acoustic neuroma)
3. Otosclerosis
- Stapes footplate is fixed by abnormal bone → stapedius contraction has no effect → absent reflex
4. Surgical significance
- During stapedectomy (surgery for otosclerosis), the stapedius tendon may be cut
- Postoperative hyperacusis can result
Memory Mnemonics
"Stapedius = Safety guard of the ear" - supplied by 7 (CN VII), protects from sound above 70 dB
Lesion level memory:
- Above GSPN → no tears + no taste + hyperacusis + paralysis
- Above stapedius nerve → hyperacusis + no taste + paralysis
- Above chorda tympani → no taste + paralysis
- At stylomastoid foramen → paralysis only
Hyperacusis
Hyperacusis - Complete Guide for MBBS
Definition
Simply put: Normal sounds feel unbearably loud or painful to the patient.
Mechanism - Why Does It Happen?
Two main mechanisms:
1. Peripheral - Loss of Stapedius Reflex
- Facial nerve (CN VII) palsy → stapedius muscle paralyzed
- No acoustic reflex = no damping of sound
- Every sound hits the cochlea at full intensity → perceived as excessively loud
- This is peripheral hyperacusis - sudden onset, with identifiable nerve lesion
2. Central - Auditory Pathway Hypersensitivity
- More common overall
- Thought to involve increased gain in central auditory processing
- Central neurons become hyperexcitable - possibly from:
- Loss of normal auditory input (sensory deprivation)
- Plastic reorganization of auditory cortex
- Limbic system involvement (explains anxiety component)
- NOT correlated with audiometric threshold - patient may have normal hearing yet still have hyperacusis
Important distinction: Hyperacusis ≠ Recruitment
- Recruitment = rapid growth of loudness perception seen in cochlear (outer hair cell) damage - a peripheral phenomenon
- Hyperacusis = central phenomenon, does NOT correlate with audiometric threshold shift
Causes (Etiology)
| Category | Causes |
|---|---|
| Peripheral (CN VII) | Bell's palsy, Ramsay Hunt syndrome, facial nerve injury, stapedectomy |
| Neurological | Migraine, head injury, Lyme disease |
| Withdrawal | Benzodiazepine withdrawal |
| Genetic/Syndromic | Williams syndrome (classic association - cheerful personality + hyperacusis) |
| Psychiatric comorbidity | Anxiety, PTSD, depression |
| Post-noise trauma | Acoustic trauma, noise-induced hearing loss |
| Idiopathic | Most common - no identifiable cause |
Clinical Features
- Everyday sounds like dishes clinking, vacuum cleaner, traffic feel painfully loud
- Tinnitus is a very frequent comorbidity (18-80% of hyperacusis patients also have tinnitus)
- Anxiety and emotional distress - nearly 50-56% have at least one psychiatric disorder
- Avoidance behavior - avoid restaurants, concerts, social settings
- Safety behaviors - constant use of earplugs/earmuffs
- Severe cases → social withdrawal, becoming housebound
- Prevalence in general population: 5.9-7.7% (some studies report up to 22%)
Hyperacusis in Bell's Palsy - HIGH YIELD
- In Bell's palsy, CN VII is affected above the origin of the nerve to stapedius
- Stapedius is paralyzed → acoustic reflex lost
- Patient complains sounds have a "booming" quality - loud and distorted
- Associated with: loss of taste (anterior 2/3 tongue), facial paralysis, sometimes reduced lacrimation
- Occurs in up to 30% of Bell's palsy patients
Topodiagnosis Using Hyperacusis (VERY HIGH YIELD EXAM TOPIC)
Bell's palsy lesion levels:
ABOVE geniculate ganglion:
→ Hyperacusis ✓ + No taste ✓ + No lacrimation ✓ + Facial palsy ✓
ABOVE nerve to stapedius (below geniculate):
→ Hyperacusis ✓ + No taste ✓ + Lacrimation intact + Facial palsy ✓
ABOVE chorda tympani (below stapedius nerve):
→ Hyperacusis absent + No taste ✓ + Facial palsy ✓
AT/BELOW stylomastoid foramen:
→ Hyperacusis absent + Taste intact + Facial palsy only ✓
Investigations
- Pure tone audiometry - to assess hearing thresholds (often normal in hyperacusis)
- Loudness Discomfort Levels (LDLs) - reduced in hyperacusis (normal ~100 dB, hyperacusis <90 dB)
- Acoustic reflex testing (tympanometry) - absent if stapedius paralyzed
- Psychiatric assessment - screen for anxiety, depression, PTSD
- MRI with gadolinium - if Bell's palsy suspected (enhancement of facial nerve)
Treatment
| Approach | Details |
|---|---|
| Sound therapy / Desensitization | White noise generators with gradually increasing sound levels - reconditions auditory system |
| Tinnitus Retraining Therapy (TRT) | Reduces avoidance, improves LDLs by ~12 dB, broadens dynamic range |
| Cognitive Behavioural Therapy (CBT) | Addresses anxiety, fear-avoidance behavior - shown effective in RCT |
| Treat underlying cause | Facial nerve palsy → corticosteroids; Lyme disease → antibiotics; BZD withdrawal → slow taper |
| Hearing aids | Can be adjusted to limit loud sounds; helpful if combined with hearing loss |
| Avoid ear protection overuse | Paradoxically, constant earplugs worsen central sensitization over time |
Key Associations to Remember
| Condition | Type of Abnormal Sound Perception |
|---|---|
| Hyperacusis | Ordinary sounds feel painfully LOUD (sensitivity) |
| Recruitment | Rapid loudness growth above threshold (cochlear OHC damage) |
| Diplacusis | Same sound heard at different pitches in each ear |
| Paracusis | Better hearing in noisy environments (otosclerosis - Willis paracusis) |
| Phonophobia | Fear/aversion to sound (psychological, without actual loudness distortion) |
One-liner for Viva
"Hyperacusis is increased sensitivity to normal sounds - peripheral cause is stapedius paralysis (Bell's palsy), central cause is auditory gain dysregulation; treated by sound desensitization and CBT."