Fistula
"arteriovenous fistula" AND classification
Arteriovenous (AV) Fistula - Definition, Types & Classification
Definition
- Harrison's Principles of Internal Medicine 22e, p. 2220
- Bailey and Love's Short Practice of Surgery 28e, p. 1045
Pathophysiological Consequences
| Effect | Mechanism |
|---|---|
| Venous arterialization | Veins become dilated, tortuous, and thick-walled due to high-pressure arterial blood |
| Increased cardiac output | Large fistulas create a significant left-to-right shunt |
| High-output cardiac failure | Consequence of sustained large-volume shunting |
| Venous hypertension | Peripheral edema, varicose veins, stasis pigmentation |
| Distal ischemia | "Steal" phenomenon - reduced arterial perfusion distal to the fistula |
Classification
1. By Etiology
A. Congenital AVF
- Result of persistent embryonic vessels that fail to differentiate into arteries and veins
- Often multiple and extensive communications
- May be associated with birthmarks (port-wine stains, cutaneous hemangiomas)
- Can occur in almost any organ; frequently in the extremities
- Difficult to treat because new communications develop after ligation
B. Acquired AVF
- Created deliberately for hemodialysis vascular access (radiocephalic, brachiocephalic, brachiobasilic)
- Also occur as complications of arterial catheterization (incidence: 0.2-2% post-catheterization femoral AVF)
- Risk factors for iatrogenic femoral AVF: female sex, hypertension, ongoing anticoagulation, left-sided groin puncture, high-dose periprocedural heparin (>12,500 units)
- Iatrogenic AVFs may close spontaneously in 38-56% of cases; traumatic ones rarely do
- Penetrating trauma: gunshot wounds, stab wounds
- Surgical dissection injury
- Rupture of an arterial aneurysm into an adjacent vein (uncommon)
2. By Location / Anatomical Site
| Location | Examples / Notes |
|---|---|
| Peripheral / Extremities | Most common; femoral, radial, brachial AVFs |
| Pulmonary | Pulmonary AVF - often congenital, associated with hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu) |
| Renal | Renal AVF - congenital or post-trauma/biopsy |
| Splanchnic / Hepatic | Splenic AVF - cause of presinusoidal portal hypertension |
| Coronary | Coronary arteriovenous fistula - anomalous coronary origin draining into cardiac chambers |
| Carotid-cavernous | Carotid-cavernous fistula (CCF) - often post-traumatic; classified by Barrow's classification |
| Spinal/Dural | Spinal dural AVF - most common spinal vascular malformation |
3. Surgically Created AVF for Hemodialysis Access (by anastomosis site)
| Type | Artery | Vein | Notes |
|---|---|---|---|
| Radiocephalic (Brescia-Cimino) | Radial artery | Cephalic vein (wrist) | First choice; distal forearm |
| Brachiocephalic | Brachial artery | Cephalic vein (elbow) | Second choice |
| Brachiobasilic | Brachial artery | Basilic vein | Requires transposition; used when cephalic vein unavailable |
4. By Anastomosis Configuration
| Type | Description |
|---|---|
| End-to-side | End of vein anastomosed to side of artery (most common) |
| Side-to-side | Side of vein to side of artery |
| End-to-end | End of vein to end of artery |
Key Clinical Signs
- Pulsatile swelling (if superficial)
- Continuous "machinery" bruit - heard throughout systole and diastole
- Palpable thrill over the fistula
- Nicoladoni-Branham sign - reflex bradycardia on manual compression of the fistula
- Skin warmth directly over the lesion
- Compression of the proximal artery causes the thrill and bruit to cease
Diagnostic Workup
- Duplex ultrasonography (DUS): First-line; shows high arterial peak systolic velocity proximal to fistula, pulsatile venous flow, turbulence at the fistula site, and rapid venous filling
- CT angiography (CTA): Defines anatomy
- Conventional angiography: Gold standard for mapping; guides endovascular treatment
Summary Table
| Feature | Congenital AVF | Acquired Traumatic AVF | Surgical AVF (Dialysis) |
|---|---|---|---|
| Cause | Failed embryonic differentiation | Penetrating trauma, iatrogenic | Deliberately created |
| Multiplicity | Often multiple | Usually single | Single |
| Spontaneous closure | No | Rarely (iatrogenic: 38-56%) | N/A |
| Treatment | Conservative + embolization | Surgery/endovascular | Maintained as access |
- Bailey and Love's Short Practice of Surgery 28e, p. 1045
- Harrison's Principles of Internal Medicine 22e, p. 2220
- Current Surgical Therapy 14e, p. 1150
- Fischer's Mastery of Surgery 8e, pp. 6991-6992
Explain in diagram representation form
Medical educational diagram of Arteriovenous (AV) Fistula - Definition, Types and Classification. Clean white background, professional medical illustration style with color coding. Layout: Vertical flowchart/mind map with sections: 1. TOP CENTER - Title box: "ARTERIOVENOUS FISTULA (AVF)" with subtitle "Abnormal direct communication between artery and vein, bypassing the capillary bed" 2. ANATOMY DIAGRAM (center-left) - Simple cross-section showing: - Red arrow labeled "ARTERY (High pressure)" - Blue arrow labeled "VEIN (Low pressure)" - Green curved arrow between them labeled "AVF = Direct Shunt (bypasses capillaries)" - Small branching capillary bed shown separately as "Normal" and crossed out 3. CLASSIFICATION TREE (right side, branching): BRANCH A: "BY ETIOLOGY" → Congenital: "Failed embryonic vessel differentiation; Multiple communications; Associated with birthmarks" → Acquired: → Traumatic: "Gunshot/stab wounds; Surgical dissection; Aneurysm rupture into vein" → Iatrogenic: "Post-catheterization (0.2-2%); Surgically created for hemodialysis" BRANCH B: "BY LOCATION" → Peripheral/Extremities (most common) → Pulmonary (HHT) → Renal → Coronary → Carotid-Cavernous → Splanchnic/Hepatic BRANCH C: "DIALYSIS AVF TYPES" (table) → Radiocephalic: Radial art. + Cephalic vein (1st choice) → Brachiocephalic: Brachial art. + Cephalic vein (2nd choice) → Brachiobasilic: Brachial art. + Basilic vein (needs transposition) 4. BOTTOM ROW - "CONSEQUENCES" boxes: - Venous arterialization (dilated, tortuous veins) - Increased cardiac output → High-output heart failure - Distal ischemia (steal phenomenon) - Venous hypertension (edema, varicosities) 5. CLINICAL SIGNS box (bottom right): - Continuous machinery bruit - Palpable thrill - Pulsatile swelling - Nicoladoni-Branham sign (bradycardia on compression) Color scheme: Red for arterial, Blue for venous, Green for fistula connections, Orange for consequences, Purple for clinical signs. Bold headers, clean lines, arrows connecting sections.
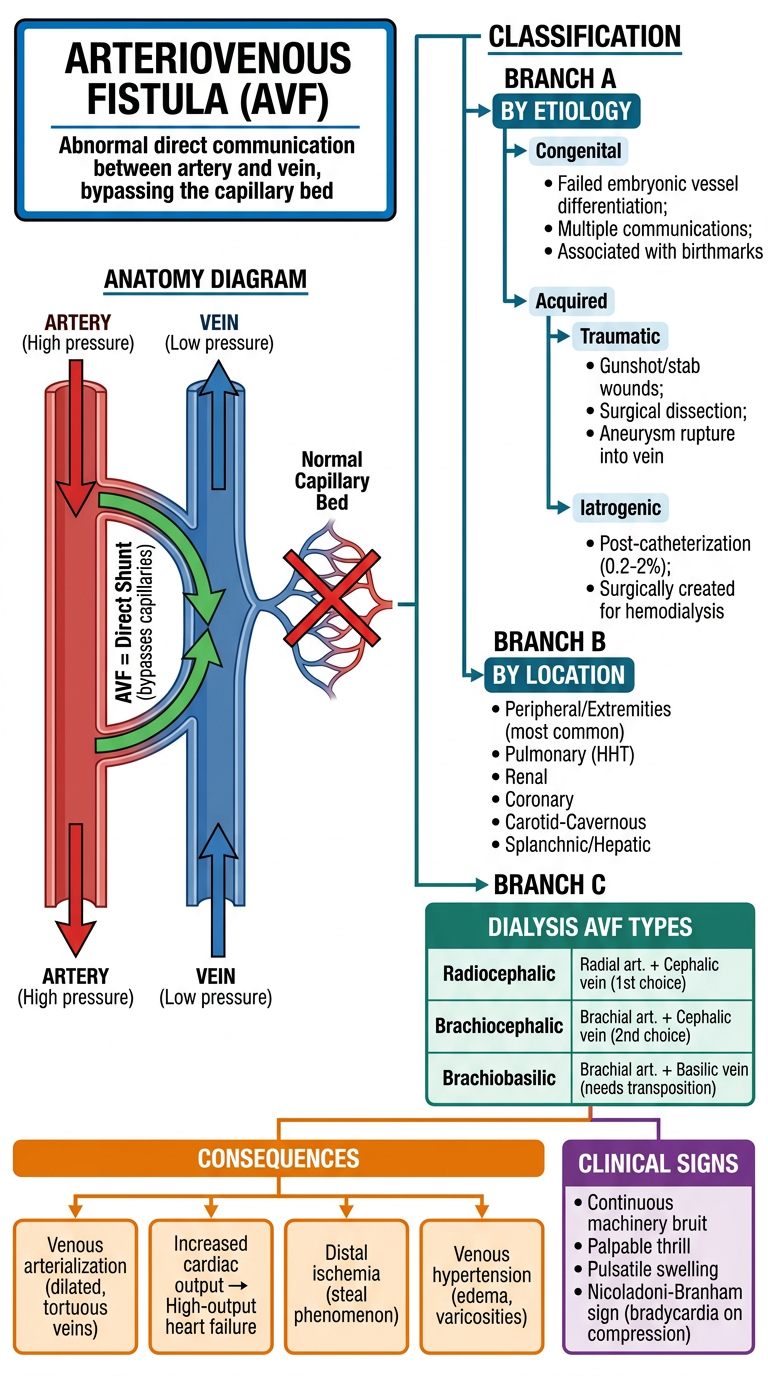
- Core concept - The direct artery-to-vein shunt bypassing the capillary bed
- Classification by Etiology - Congenital vs. Acquired (Traumatic vs. Iatrogenic)
- Classification by Location - Peripheral, Pulmonary, Renal, Coronary, Carotid-Cavernous, Splanchnic
- Dialysis AVF types - Radiocephalic (1st choice) → Brachiocephalic (2nd) → Brachiobasilic (needs transposition)
- Hemodynamic consequences - High-output failure, venous arterialization, distal steal ischemia, venous hypertension
- Clinical signs - Machinery bruit, thrill, pulsatile swelling, Nicoladoni-Branham sign