Appearances of organs and body parts in pregnancy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Here is the full, organized response:
Appearances of Organs and Body Parts in Pregnancy
Pregnancy produces characteristic changes in the appearance, position, and function of nearly every organ system. These are organized below by system.
1. Uterus
The uterus is the most visibly transformed organ:
- Weeks 1-12: Remains entirely within the bony pelvis; an intrapelvic organ
- Week 12: Begins to rise out of the pelvis, becomes palpable abdominally
- Week 20: Reaches the umbilicus
- Weeks 34-36: Reaches the costal margins
- At term: Enlarged by ~30 cm and increased 15-fold in weight
Signs of uterine change:
- Hegar's sign (8-10 weeks): The isthmus (between the body and cervix) feels soft and compressible on bimanual exam; the cervix feels firm and the body feels elastic
- Braxton Hicks contractions: Intermittent, painless contractions from the 3rd-4th month onward
- Red, subcutaneous scars (striae gravidarum): Appear on the abdomen due to skin stretching
- ROSEN's Emergency Medicine, p. 3289 | P.C. Dikshit Textbook of Forensic Medicine, p. 3284
2. Cervix
- Softens progressively from below upward from the 2nd month onward - this is Goodell's sign, well marked by the 4th month
- At the last month: the cervical os becomes circular (instead of transverse) and admits a fingertip more easily
- At 3rd month: the angle between the body and cervix is accentuated
- P.C. Dikshit Textbook of Forensic Medicine, p. 3309
3. Vagina
- Mucous membrane changes color: pink → violet → blue due to venous congestion
- Visible from the 4th week onward
- Known as Chadwick's sign (or Jacquemier's sign)
- Tissue becomes softer, secretions increase, and pulsations of the vaginal artery become palpable early
- P.C. Dikshit Textbook of Forensic Medicine, p. 3258
4. Breasts
Changes are most significant in a first pregnancy (primigravida):
- Size increases due to hypertrophy of mammary glands
- Superficial veins become engorged and visible
- Nipple becomes deeply pigmented and erectile
- Areola becomes darkly brown by the 2nd month (Montgomery's tubercles - sebaceous glands enlarge and form tubercles around the nipple)
- Colostrum formation begins in the 3rd month (thin yellowish fluid)
- Silvery striae appear on the breast skin after 6 months from stretching
- P.C. Dikshit Textbook of Forensic Medicine, p. 3244
5. Skin
- Skin of the vulva, abdomen, and axilla become darker (hyperpigmented)
- Dark circles form around the eyes (chloasma/melasma)
- Linea nigra forms: a dark, pigmented line running from the pubis, encircling the umbilicus, and continuing up to the ensiform (xiphoid) cartilage
- Striae gravidarum (stretch marks): red/silvery lines on the abdomen and breasts
- P.C. Dikshit Textbook of Forensic Medicine, p. 3257
6. Diaphragm and Chest
- The diaphragm progressively rises as the uterus enlarges
- Compensatory flaring of the ribs occurs
- On a chest X-ray: the heart appears enlarged (shifted position), and prominent vascular markings are visible due to increased pulmonary blood volume
- On ECG: left axis deviation and T-wave changes are seen
- This elevated diaphragm means thoracostomy in the third trimester requires chest tube placement one to two interspaces higher than the usual 5th interspace
- Morgan & Mikhail's Clinical Anesthesiology, p. 2402 | ROSEN's Emergency Medicine, p. 3289
7. Heart
- The heart is displaced upward and to the left by the rising diaphragm
- On physical exam: a grade I-II systolic ejection murmur is common (flow murmur from increased cardiac output)
- Exaggerated splitting of S1; an S3 may be audible
- A small, asymptomatic pericardial effusion may develop
- Blood volume increases ~35%; cardiac output rises ~40%
- Morgan & Mikhail's Clinical Anesthesiology, p. 2402
8. Abdominal Viscera (Bowel, Stomach, Appendix)
- All abdominal organs are pushed upward by the enlarging uterus
- The stomach is displaced upward and anteriorly, promoting gastroesophageal sphincter incompetence - hence heartburn and reflux are common
- The cecum and appendix are displaced upward - right lower quadrant pain shifts toward the right upper quadrant as pregnancy advances, complicating diagnosis of appendicitis
- The normal peritoneal response (guarding, rebound) is blunted because the abdominal wall is stretched - injury severity can be underestimated
- ROSEN's Emergency Medicine, p. 3291 | Tintinalli's Emergency Medicine, p. 338
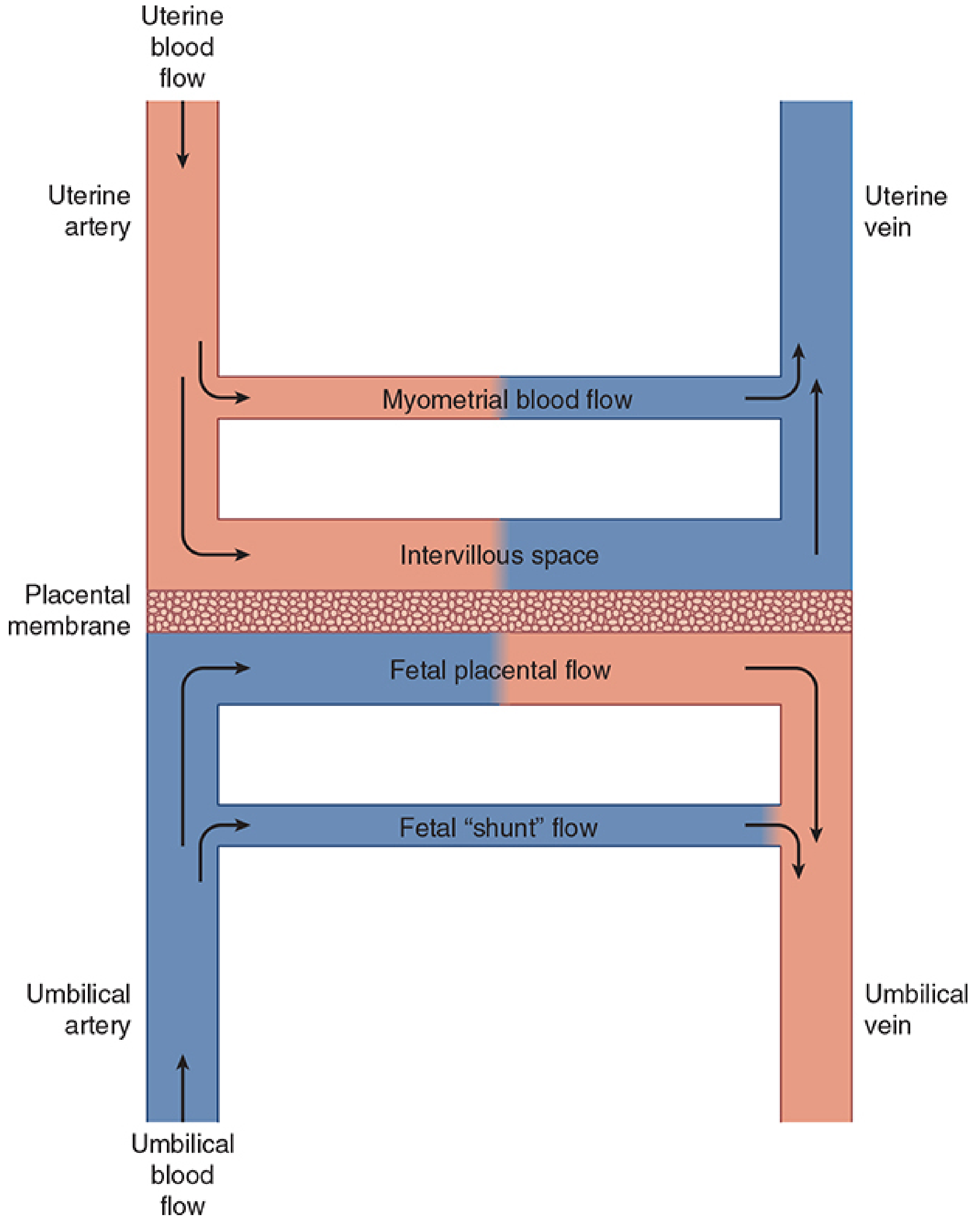
Uteroplacental circulation - Morgan & Mikhail's Clinical Anesthesiology
9. Kidneys and Ureters
- Kidneys increase in size by approximately 1 cm in length (measured by ultrasound)
- Dilation of the collecting system (hydronephrosis/hydroureter) begins as early as the 3rd month - the right renal pelvis is most often affected
- This dilation is partly hormonal (not just mechanical compression) and normally resolves by 12 weeks postpartum
- Persistent dilation beyond 12-16 weeks postpartum suggests true mechanical obstruction
- Ureteral dilation from smooth muscle relaxation or compression by the gravid uterus is a normal finding on imaging
- National Kidney Foundation Primer on Kidney Diseases, p. 2710 | ROSEN's Emergency Medicine, p. 3293
10. Bladder
- In the first trimester: the bladder is protected by the bony pelvis
- After the 3rd month: both the uterus and bladder rise out of the pelvis, becoming vulnerable to direct injury
- Both organs become hyperemic (engorged with blood) during pregnancy
- The enlarging uterus presses on the bladder, causing urinary frequency - this symptom eases mid-pregnancy and returns when the fetal head descends into the pelvis near term
- ROSEN's Emergency Medicine, p. 3293 | P.C. Dikshit Textbook of Forensic Medicine, p. 3269
11. Epidural Venous Plexus and Spine
- Obstruction of the inferior vena cava by the gravid uterus (especially when supine) distends the epidural venous plexus
- This decreases the volume of the epidural space and increases epidural pressure (positive rather than the usual negative)
- Increases the risk of intravascular injection during epidural anesthesia
- Morgan & Mikhail's Clinical Anesthesiology, p. 2366
Summary Table
| Organ/Structure | Key Change in Appearance/Position |
|---|---|
| Uterus | Rises from pelvis to costal margin; 15x weight increase |
| Cervix | Softens, os becomes circular (Goodell's sign) |
| Vagina | Pink → violet → blue (Chadwick's sign) |
| Breasts | Enlarged, engorged veins, dark nipple/areola, striae |
| Skin | Linea nigra, chloasma, striae gravidarum, hyperpigmentation |
| Diaphragm | Elevated; ribs flare; FRC decreases 20% |
| Heart | Shifted left/upward; appears enlarged on CXR; flow murmur |
| Stomach | Displaced upward/anteriorly; reflux common |
| Appendix/Cecum | Displaced upward - pain location shifts |
| Kidneys | 1 cm longer; right-sided hydronephrosis |
| Bladder | Rises from pelvis after week 12; hyperemic |
| Epidural veins | Engorged; reduced epidural space volume |
Fetal parts appearance in Usg
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, image-rich content from multiple authoritative sources. Here is the complete answer:
Fetal Parts - Appearance on Ultrasound (USG)
Obstetric ultrasound identifies fetal parts by their characteristic echogenicity, shape, and location. The standard mid-trimester anatomy scan (18-22 weeks) is the primary window for evaluating all fetal structures.
Developmental Landmarks by Gestational Age (Transabdominal USG)
| Landmark | Gestational Age (from LMP) |
|---|---|
| Gestational sac visible | 5-6 weeks |
| Embryonic pole | 6-7 weeks |
| Fetal heart motion | 7-8 weeks |
| Fetal movement | 8-9 weeks |
| Biparietal diameter (BPD) measurable | 12-13 weeks |
(All of the above can be seen 1 week earlier with transvaginal scanning)
- Pfenninger & Fowler's Procedures for Primary Care, p. 5081
Early Pregnancy Structures
Gestational Sac (5-6 weeks)
- Appears as a hypoechogenic (anechoic/dark) area = the chorionic vesicle
- Surrounded by a bright echogenic rim = the trophoblast
- A double echogenic ring is the hallmark of a normal intrauterine pregnancy:
- Inner ring = decidua capsularis + chorion laeve
- Outer ring = decidua vera
- Measured inside the hyperechoic rim (anechoic space only); if round - one diameter; if ovoid - average of three diameters
Yolk Sac (from ~5 weeks TVS, ~6-7 weeks TAS)
- Small, round, bright echogenic ring within the gestational sac
- Its presence confirms an intrauterine gestation
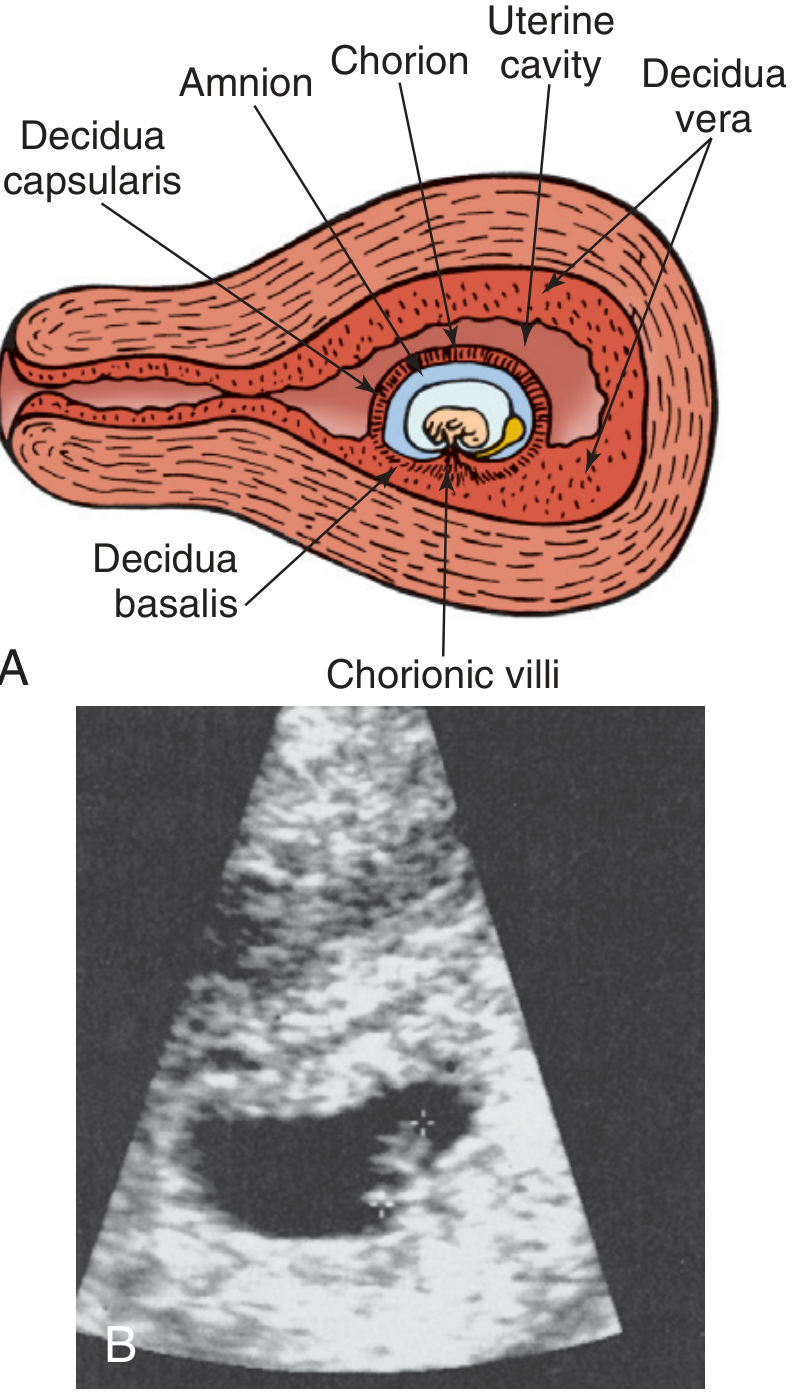
Early gestation: decidua capsularis and decidua vera form the double echogenic ring - Pfenninger & Fowler's, p. 5120
- Pfenninger & Fowler's Procedures for Primary Care, p. 5109-5124
Fetal Biometry: The Four Key Measurements
Standard biometry measurements - Langman's Medical Embryology, p. 3367
1. Crown-Rump Length (CRL) - 6 to 12 weeks
- The longest sagittal diameter of the fetus, from top of skull to base of rump
- Excludes limb buds and the yolk sac
- Fetus appears as a small elongated echogenic structure within the anechoic amniotic fluid
- Most accurate between 7-9 weeks (TVS) or 9-11 weeks (TAS)
- Formula: Gestational age (weeks) = (CRL [mm] + 65) / 10
- Accuracy: ±3-5 days
2. Biparietal Diameter (BPD) - from 12-13 weeks
- Cross-sectional view of the fetal skull at the level of the thalami
- The skull appears as a bright oval echogenic ring
- Measured outer table to inner table (only outer-to-inner measurement in all of sonography - because the posterior calvarium causes artifact that distorts outer-to-outer measurements)
- Reference plane cuts through: falx cerebri, thalamus, cavum septi pellucidi, and medial cerebral artery
- Head should be oval-shaped at this plane
- Normal cephalic index (BPD:OFD) = 78.3% ± 8%; below = dolichocephalic; above = brachycephalic
- Accuracy: ±1.5 weeks (14-20 wks); ±3-4 weeks (third trimester)
3. Head Circumference (HC)
- Measured in the same BPD plane
- HC = 1.57 × (BPD + OFD)
- More reliable than BPD when skull shape is abnormal
4. Abdominal Circumference (AC)
- Cross-section of the fetal abdomen at the level of the portal vein junction
- Structures visible in this plane:
- Stomach - seen as a hypoechoic (dark) bubble on the LEFT side of the fetus
- Umbilical vein (UV) - echogenic curved structure joining the left portal vein
- Spine (Sp) - echogenic shadowing structure posteriorly
- Aorta (Ao) and Vena Cava (VC) - visible as small circular structures near the spine
- AC = 1.57 × (transverse diameter + anteroposterior diameter)
5. Femur Length (FL) - from ~14 weeks
- The femoral diaphysis appears as a bright echogenic line (the calcified shaft)
- Measured along the central shaft only - NOT including the epiphysis
- The beam should be as perpendicular to the shaft as possible
- Distal femoral epiphyseal ossification center (echogenic dot at the distal end) appears at 33 weeks or more - a maturity marker
- FL/BPD ratio is constant after 22 weeks = 79% ± 8%
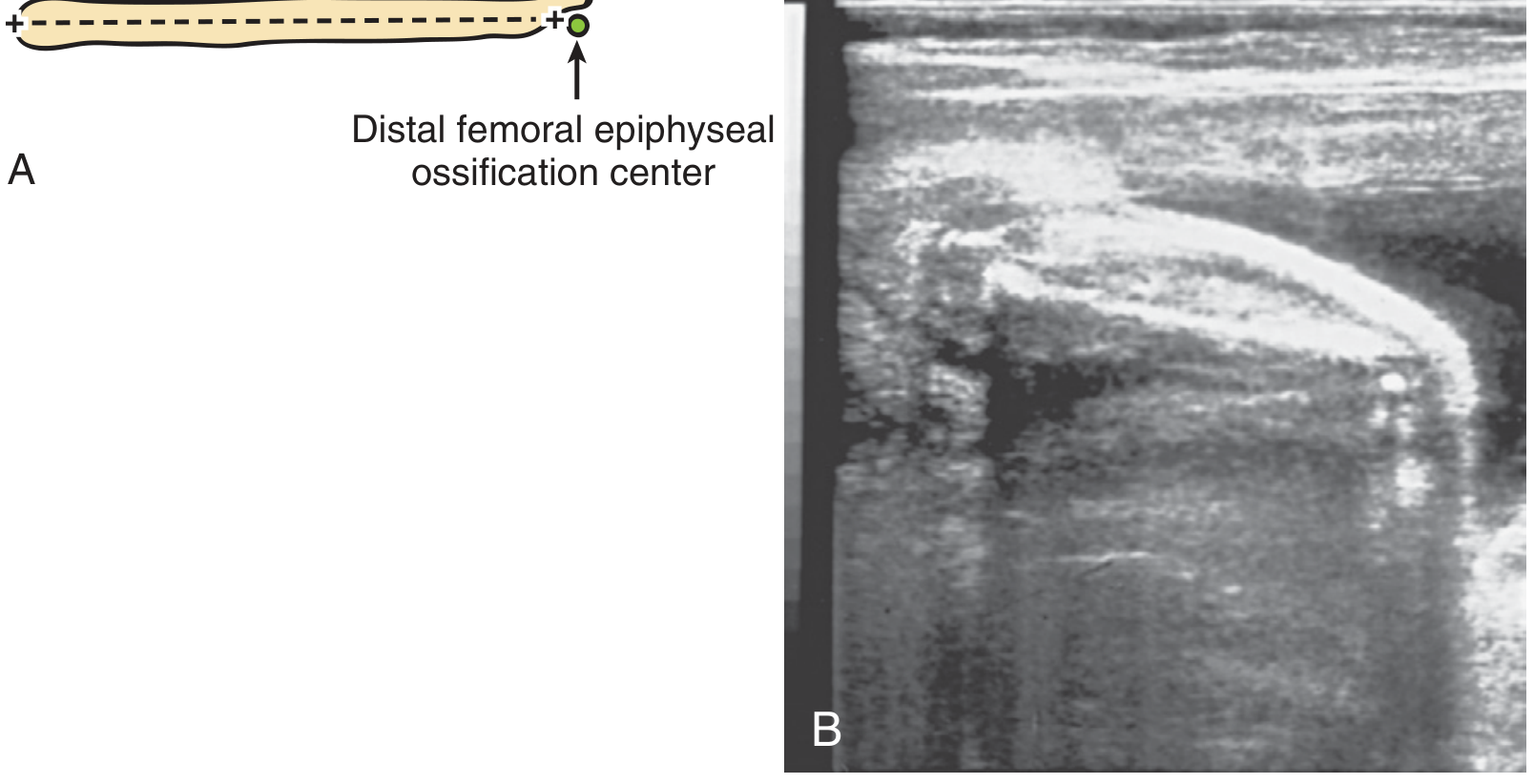
Femur length measurement - Pfenninger & Fowler's, p. 5218
Head and Brain Structures
Cranial Vault
- Appears as a bright echogenic oval ring in cross-section
- Falx cerebri: a midline echogenic line dividing the two hemispheres
Structures Assessed at the BPD Plane
- Thalami - paired symmetric hypoechoic structures at the center
- Cavum septi pellucidi - a small fluid-filled (anechoic) box-like space between the two leaflets of the septum pellucidum; present between 18-37 weeks; its absence suggests holoprosencephaly or agenesis of the corpus callosum
- Lateral ventricles - measured at the atrium; normal width <10 mm (anechoic fluid-filled spaces)
Cerebellum / Posterior Fossa
- Viewed on a plane slightly inferior and posterior to the BPD plane
- Cerebellum: appears as a "dumbbell" or "butterfly" shape - two echogenic cerebellar hemispheres connected by the hypoechoic vermis
- Cisterna magna: anechoic space behind the cerebellum (normal 2-10 mm)
- Nuchal translucency (NT): measured 11-14 weeks - the anechoic translucent space at the back of the fetal neck; thickness >3 mm associated with Down syndrome
Face
- Orbits: two symmetric anechoic circles (the lens appears as a bright echogenic dot)
- Facial profile (sagittal view): nasal bone, forehead, lips, chin all assessable
- Upper lip continuity: assessed to exclude cleft lip (gap in echogenic lip line)
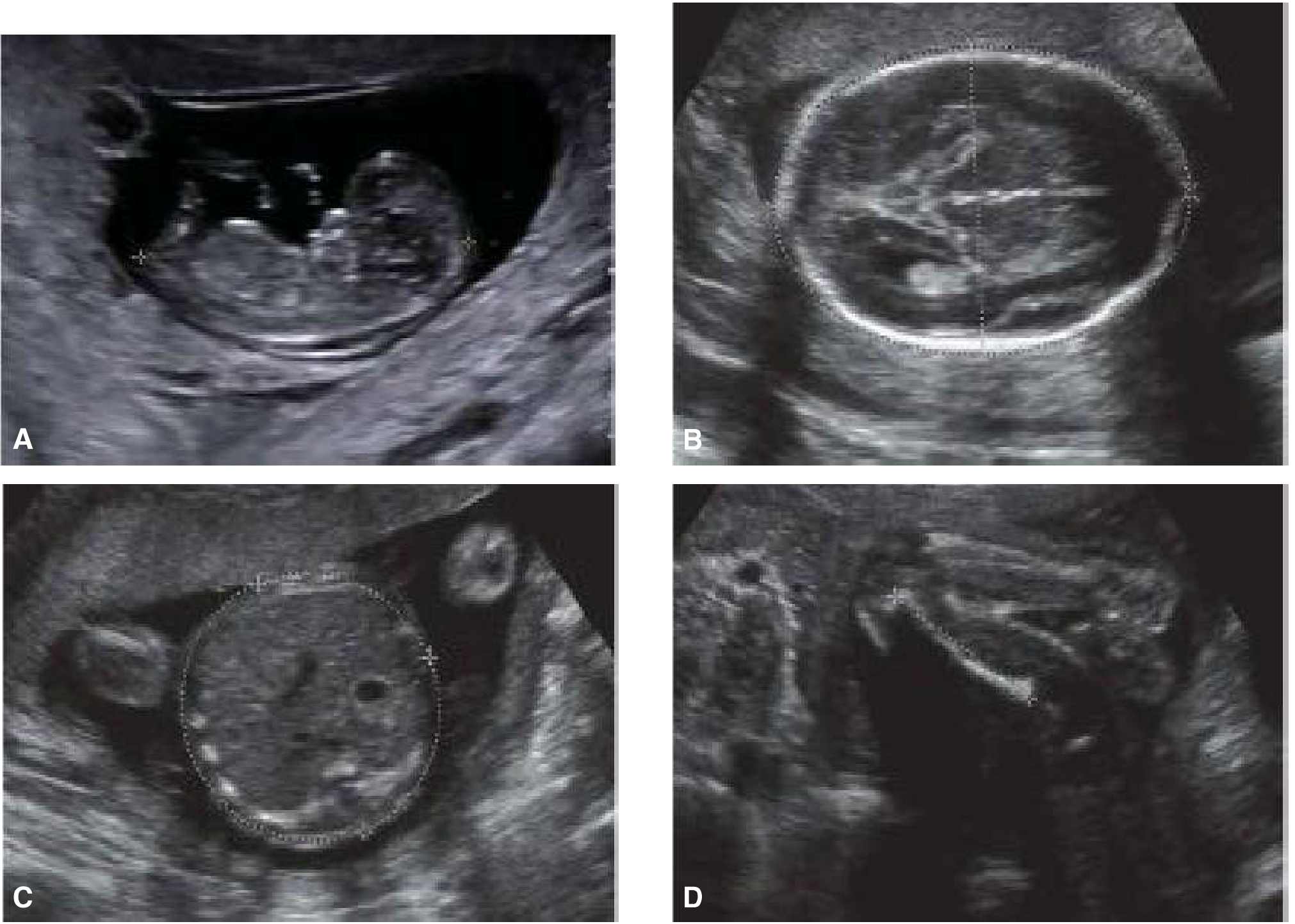
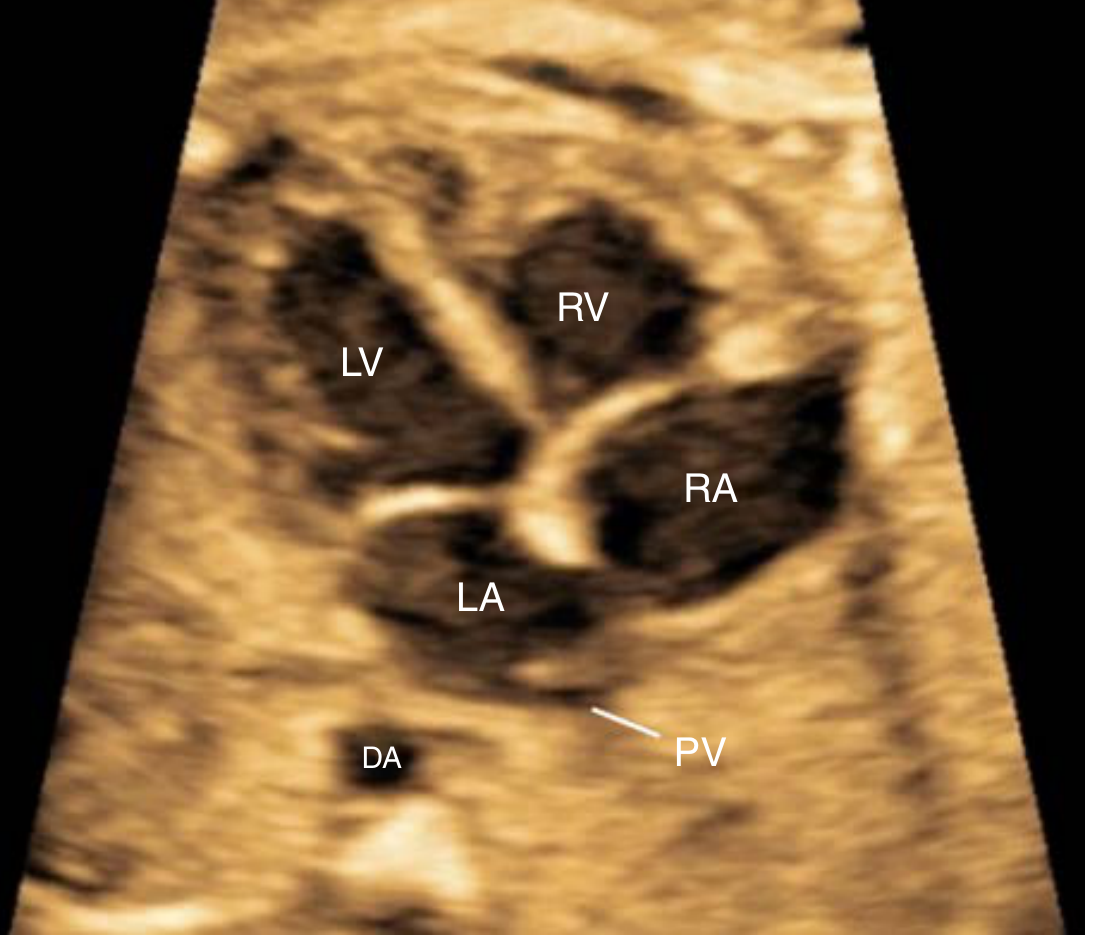
Heart (18-22 weeks)
The heart should occupy no more than one-third of the cross-sectional area of the thorax.
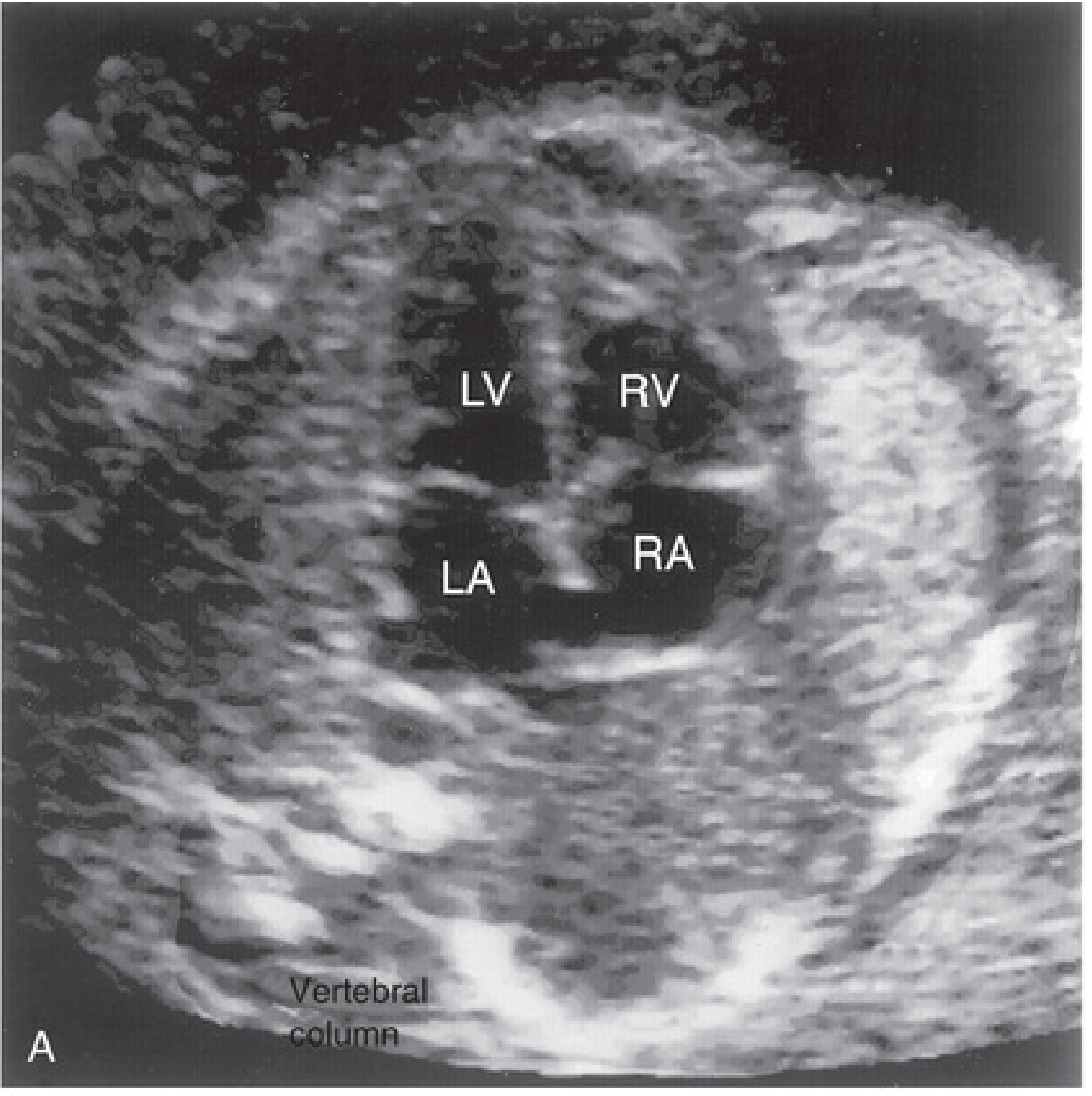
Fetal four-chamber view - The Developing Human (Clinically Oriented Embryology), p. 4091
Fetal echocardiography four-chamber view - Creasy & Resnik's Maternal-Fetal Medicine, p. 46
Four-Chamber View
- Both atria and both ventricles appear as four anechoic (dark) chambers separated by echogenic walls and septa
- Right side (RV, RA) is normally slightly larger than left
- Ventricular septum: echogenic line between ventricles (dropout artifact can mimic VSD - assess with beam perpendicular to septum)
- Foramen ovale flap: visible in the left atrium, normally opens toward LA
- Tricuspid valve inserts slightly more apically (toward apex) than the mitral valve - an important landmark
- Moderator band: characterizes the right ventricular apex (echogenic trabecular band)
- Pulmonary veins drain into the left atrium (visible as small anechoic channels)
- Descending aorta (DA): visible as a small anechoic circle posterior to the heart near the spine
Outflow Tracts
- LVOT (left ventricular outflow tract) and RVOT are also assessed in the standard scan
- Creasy & Resnik's Maternal-Fetal Medicine, p. 50-64
Thorax / Lungs
- Lung parenchyma: appears as homogeneously echogenic tissue on both sides of the heart
- Lungs should be symmetric; hyperechoic lung mass = may indicate CCAM or sequestration; anechoic pleural fluid = effusion
Abdomen
Stomach
- Appears as a well-defined anechoic (black) cystic bubble in the LEFT upper abdomen
- Absence of stomach bubble raises concern for esophageal atresia or CNS abnormality
Liver and Intestines
- Liver: the largest abdominal organ; moderately echogenic (mid-gray)
- Small bowel loops: mildly echogenic, not as bright as bone; colon is more prominent in late pregnancy
- Umbilical cord insertion into the anterior abdominal wall: confirms normal abdominal wall closure (absence/defect = omphalocele or gastroschisis)
Kidneys
- Located bilaterally flanking the spine
- Renal cortex: slightly less echogenic than adjacent liver/spleen
- Renal pelvis: small anechoic center (fluid); dilated >7 mm = pyelectasis, may indicate obstruction or Down syndrome
- Bladder: oval anechoic structure in the pelvis; should fill and empty cyclically; two umbilical arteries run alongside it (visible with colour Doppler)
- Creasy & Resnik's Maternal-Fetal Medicine, Box 16.3, p. 931-960
Spine
- Longitudinal view: two parallel echogenic lines (posterior elements), converging at the sacrum
- Transverse view: three echogenic dots in a triangle (vertebral body + two posterior elements)
- Normal skin covering overlying the spine should be visible and intact
- Open neural tube defects (spina bifida) show a gap with soft tissue protrusion; associated "banana sign" (cerebellum pulled down, looking like a banana) and "lemon sign" (frontal bossing of skull)
Extremities
- Long bones (humerus, radius, ulna, femur, tibia, fibula): appear as bright echogenic lines with acoustic shadowing (dark shadow behind them)
- All four extremities must be visualized; upper and lower long bones assessed
- Hands and feet: fingers and toes visible; posture and movement assessed
- Shortening, bowing, or fractures suggest skeletal dysplasia
Genitalia
- Male: echogenic scrotum and penis visible, testes may be seen in the scrotum after 28-32 weeks
- Female: three echogenic lines (labial folds) visible in the perineum
Placenta and Amniotic Fluid (Assessed Alongside Fetal Parts)
- Placenta: uniformly granular echogenic structure; classified by Grannum grading (Grade 0-III for maturity)
- Umbilical cord: contains 2 arteries + 1 vein; appears as a 3-vessel cord on transverse section
- Amniotic fluid: anechoic (black); assessed by amniotic fluid index (AFI) or single deepest pocket
Accuracy of USG Dating
| Gestational Age | Measurement | Accuracy |
|---|---|---|
| 3-5 weeks | None | - |
| 5-6 weeks | Gestational sac | ±1 week |
| 6-12 weeks | CRL | ±3-5 days |
| 12-20 weeks | BPD, HC, AC, FL | ±1-1.5 weeks |
| 20-30 weeks | Multiple parameters | ±2-3 weeks |
| >30 weeks | Multiple parameters | ±3-4 weeks |
- Pfenninger & Fowler's Procedures for Primary Care, p. 5225
This is a shared conversation. Sign in to Orris to start your own chat.