Teach like a beginner how to read and interprete ECG
how to read ECG for beginners step by step guide
How to Read and Interpret an ECG - A Beginner's Complete Guide
What is an ECG?
Part 1 - The Electrical Story of One Heartbeat

- SA node (sinoatrial node) - the heart's natural pacemaker, in the right atrium. Fires a spark.
- Spark spreads across both atria → they contract (squeeze blood into ventricles).
- Signal reaches the AV node (atrioventricular node) → it intentionally slows the signal to give ventricles time to fill.
- Signal passes down the Bundle of His → splits into right and left bundle branches.
- Branches spread into Purkinje fibers → ventricles depolarize and contract (the main pumping action).
- Heart muscles repolarize (reset electrically) → ready for the next beat.
Part 2 - The ECG Paper: How to Read the Grid
Each tiny square = 0.04 seconds (40 ms) wide, 1 mm tall
Each big square = 0.20 seconds (200 ms) wide, 5 mm tall
Standard speed = 25 mm per second
Standard height = 1 mV = 10 mm (10 small squares)
Part 3 - The Waves, Segments, and Intervals

The P Wave
- What it is: The first small rounded bump.
- What it means: Atrial depolarization - the atria are contracting.
- Normal: Upright (positive) in lead II, rounded, <0.12 s wide (3 small boxes), <2.5 mm tall.
- If abnormal: Missing P waves → think atrial fibrillation. Tall/wide P waves → atrial enlargement.
The PR Interval
- What it is: From the start of P to the start of QRS.
- What it means: Time for the signal to travel from atria through the AV node to the ventricles.
- Normal: 0.12 - 0.20 s (3 to 5 small boxes / up to 1 big box).
- If too long (>0.20 s): First-degree AV block (signal is delayed).
- If too short (<0.12 s): Pre-excitation (signal bypasses the AV node, as in Wolff-Parkinson-White).
The QRS Complex
- What it is: A tall, narrow, sharp spike - the most prominent feature on any ECG.
- What it means: Ventricular depolarization - both ventricles contracting and pumping blood.
- Parts:
- Q wave - first downward deflection (if present)
- R wave - first upward deflection
- S wave - downward deflection after R
- Normal: <0.12 s wide (<3 small boxes), narrow and sharp.
- If wide (≥0.12 s): Bundle branch block, ventricular rhythm, or drug toxicity.
- Pathological Q waves (deep and wide): Old myocardial infarction.
The ST Segment
- What it is: The flat line between the end of QRS and the start of the T wave.
- What it means: Ventricular plateau phase - ventricles are still depolarized (between contraction and recovery).
- Normal: Should sit on the baseline (isoelectric) - neither elevated nor depressed.
- If elevated: STEMI (ST-elevation myocardial infarction) - a heart attack in progress. This is an emergency.
- If depressed: Ischemia (reduced blood flow to heart muscle) or certain drug effects.
The T Wave
- What it is: A broad, rounded bump after the QRS.
- What it means: Ventricular repolarization (the heart "resetting" electrically).
- Normal: Should be upright (same direction as QRS) in most leads, rounded, not too tall or too peaked.
- If inverted: Ischemia, bundle branch block, ventricular hypertrophy.
- If peaked/tall: Hyperkalemia (high potassium) - can be dangerous.
The QT Interval
- What it is: From the start of QRS to the end of T wave.
- What it means: Total time for ventricular depolarization + repolarization.
- Normal: Roughly <440 ms in men, <460 ms in women (varies with heart rate - always "correct" it with the QTc formula).
- If prolonged: Risk of dangerous arrhythmias (Torsades de pointes). Caused by drugs, electrolyte problems, or congenital syndromes.
The U Wave
- What it is: A small, optional bump after the T wave.
- What it means: Thought to represent repolarization of Purkinje fibers or papillary muscles.
- Normal: Present in some people, especially in leads V2-V3, same direction as T.
- If prominent: Hypokalemia (low potassium).
Part 4 - The 12 Leads: What Are They?
- Leads I, II, III (standard limb leads)
- Leads aVR, aVL, aVF (augmented limb leads)
- V1, V2, V3, V4, V5, V6
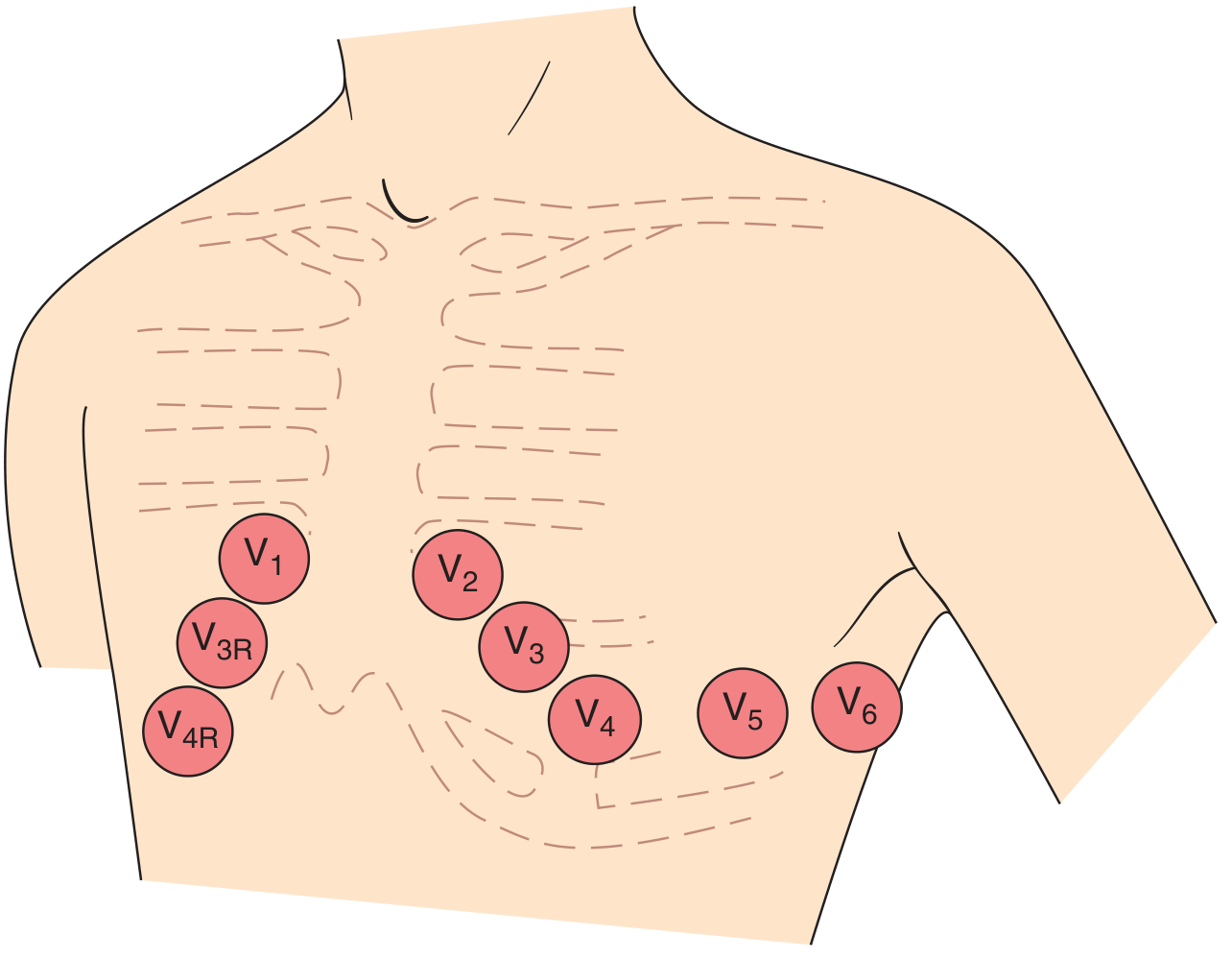
- V1: Right sternal border, 4th intercostal space
- V2: Left sternal border, 4th intercostal space
- V3: Between V2 and V4
- V4: Midclavicular line, 5th intercostal space
- V5: Anterior axillary line, same level as V4
- V6: Midaxillary line, same level as V4 and V5
| Territory | Leads |
|---|---|
| Inferior wall | II, III, aVF |
| Anterior wall | V1 - V4 |
| Lateral wall | I, aVL, V5, V6 |
| Right ventricle | V1, V3R, V4R |
Part 5 - The Systematic 7-Step Approach
Step 1 - Check Rate
1 big box → 300 bpm
2 big boxes → 150 bpm
3 big boxes → 100 bpm
4 big boxes → 75 bpm
5 big boxes → 60 bpm
6 big boxes → 50 bpm
- >100 bpm = Tachycardia
- <60 bpm = Bradycardia
Step 2 - Check Rhythm
- Are the R-R intervals regular or irregular? (Mark peaks on a piece of paper and compare)
- Is there a P wave before every QRS? Is there a QRS after every P?
- No P waves + irregularly irregular → Atrial Fibrillation (AF)
- Sawtooth baseline + rapid rate → Atrial Flutter
- Wide complex + very fast → Ventricular Tachycardia (VT) - emergency
- No organised activity → Ventricular Fibrillation (VF) - cardiac arrest
Step 3 - Check Axis
| Lead I | Lead aVF | Axis |
|---|---|---|
| Positive (up) | Positive (up) | Normal (-30° to +90°) |
| Positive (up) | Negative (down) | Left axis deviation |
| Negative (down) | Positive (up) | Right axis deviation |
| Negative (down) | Negative (down) | Extreme / Northwest |
Step 4 - Check Intervals
| Interval | Normal | Too Long means... |
|---|---|---|
| PR | 0.12 - 0.20 s | AV block (1st, 2nd, 3rd degree) |
| QRS | < 0.12 s | Bundle branch block or ventricular rhythm |
| QTc | <440 ms (men), <460 ms (women) | Drug effect, electrolyte problem, risk of arrhythmia |
Step 5 - Examine the P Wave
- Present before every QRS? → Normal sinus mechanism
- Absent? → AF, junctional rhythm, or SA node problem
- Tall and peaked (>2.5 mm in II)? → Right atrial enlargement
- Wide and notched (>0.12 s in II)? → Left atrial enlargement
- Inverted in II? → Ectopic atrial rhythm (signal not coming from SA node)
Step 6 - Examine the ST Segment and T Waves
- In two or more consecutive leads → STEMI (acute MI) - call for help immediately
- Saddle-shaped, diffuse → Pericarditis
- Persistent with Q wave → Ventricular aneurysm
- Horizontal or downsloping → Ischemia (NSTEMI or unstable angina)
- Upsloping → Less specific, may be normal
- Symmetrically inverted in a territory → Ischemia or post-MI ("Wellens" pattern in V2-V3 is a warning of LAD stenosis)
- Peaked and tall → Hyperkalemia
- Flattened → Hypokalemia, ischemia
Step 7 - Look for Special Patterns
- RBBB (Right Bundle Branch Block): Wide QRS + rSR' ("bunny ears") in V1 + wide S wave in V6. Memory: WiRRy - Wide QRS, R in Right leads (V1).
- LBBB (Left Bundle Branch Block): Wide QRS + broad notched R in I/aVL/V6 + QS in V1. Memory: WiLLiaM - W in V1, M in V6 for LBBB.
- LVH (Left Ventricular Hypertrophy): Tall R in V5 or V6 + deep S in V1 (sum >35 mm = Sokolow-Lyon criterion)
- RVH: Tall R in V1, right axis deviation
- 1st degree: PR >0.20 s, every P followed by QRS - benign
- 2nd degree Mobitz I (Wenckebach): PR gradually lengthens until a beat is dropped
- 2nd degree Mobitz II: PR constant, then a QRS suddenly drops - more serious
- 3rd degree (complete): P waves and QRS complexes march independently - emergency
- Hyperkalemia: Peaked T → widened QRS → sine wave pattern → VF
- Hypokalemia: Flat T + prominent U wave + prolonged QT
- Hypercalcemia: Short QT interval
- Hypocalcemia: Long QT interval
Part 6 - Putting It All Together: A Worked Example
- Rate: Count R-R big boxes → 4 boxes → 75 bpm. Normal.
- Rhythm: R-R regular. P before every QRS. Looks like sinus rhythm.
- Axis: Lead I upright, aVF upright → Normal axis.
- Intervals: PR = 0.16 s ✓. QRS = 0.08 s ✓. QTc = 420 ms ✓.
- P waves: Upright in II, smooth, <2.5 mm. ✓.
- ST/T waves: 2 mm ST elevation in II, III, aVF + reciprocal ST depression in I and aVL → Inferior STEMI (right coronary artery territory). Call a code.
- No bundle branch block or other special patterns noted.
Part 7 - The 14-Point Checklist (Harrison's Framework)
- Standardisation / calibration (is the 1 mV = 10 mm marker present?)
- Technical quality (leads reversed? motion artifact?)
- Rhythm
- Heart rate
- PR interval / AV conduction
- QRS interval
- QT / QTc interval
- Mean QRS electrical axis
- P waves
- QRS voltages
- Precordial R-wave progression (R waves should grow V1 → V6)
- Abnormal Q waves
- ST segments
- T waves (and U waves)
Quick Reference Card
| Feature | Normal Value | Abnormal clue |
|---|---|---|
| Heart rate | 60-100 bpm | Tachy (>100) or Brady (<60) |
| PR interval | 0.12-0.20 s | Long = AV block; Short = pre-excitation |
| QRS duration | <0.12 s | Wide = BBB or ventricular rhythm |
| QTc | <440/460 ms | Long = arrhythmia risk |
| P wave | Upright in II, <2.5 mm, <0.12 s | Absent = AF; Wide = LAE; Tall = RAE |
| ST segment | Isoelectric | Elevation = STEMI; Depression = ischemia |
| T wave | Upright, same direction as QRS | Inverted = ischemia; Peaked = hyperK |
| Axis | -30° to +90° | LAD or RAD = pathology |
Tips for Beginners
- Always compare with a previous ECG - changes are often more important than absolute values.
- Treat the patient, not the ECG - a finding means nothing without clinical context.
- When in doubt, read it systematically - most errors come from skipping steps.
- Practice on real strips - free resources like ECG Wave-Maven (Harvard) let you practice hundreds of real cases.
- The most dangerous ECGs are the normal-looking ones - always do all 7 steps.
Generate a quick-reference PDF cheat sheet on ECG patterns
ls -la /home/daytona/workspace/ 2>/dev/null && mkdir -p /home/daytona/workspace/ecg-cheatsheet
~/ecg-cheatsheet/generate_ecg_cheatsheet.py
#!/usr/bin/env python3
"""
ECG Quick-Reference Cheat Sheet
Generates a professional, color-coded 2-page PDF cheat sheet.
"""
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.lib.styles import ParagraphStyle
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether, PageBreak
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_RIGHT
from reportlab.platypus.flowables import Flowable
from reportlab.pdfgen import canvas
from reportlab.lib.colors import HexColor
# ── Colour palette ──────────────────────────────────────────────────────────
C_NAVY = HexColor("#0D2137")
C_TEAL = HexColor("#0A7E8C")
C_RED = HexColor("#C0392B")
C_ORANGE = HexColor("#E67E22")
C_GREEN = HexColor("#1A7A4A")
C_PURPLE = HexColor("#6C3483")
C_YELLOW = HexColor("#F1C40F")
C_LBLUE = HexColor("#EBF5FB")
C_LGREY = HexColor("#F4F6F7")
C_LRED = HexColor("#FDEDEC")
C_LGREEN = HexColor("#EAFAF1")
C_LORANGE = HexColor("#FEF9E7")
C_LTEAL = HexColor("#E8F8F5")
C_LPURP = HexColor("#F5EEF8")
C_WHITE = colors.white
C_BLACK = colors.black
W, H = A4 # 210 x 297 mm
# ── Styles ───────────────────────────────────────────────────────────────────
def make_styles():
return {
"title": ParagraphStyle("title", fontName="Helvetica-Bold",
fontSize=18, textColor=C_WHITE,
alignment=TA_CENTER, spaceAfter=2),
"subtitle": ParagraphStyle("subtitle", fontName="Helvetica",
fontSize=9, textColor=HexColor("#D6EAF8"),
alignment=TA_CENTER),
"sec_hdr": ParagraphStyle("sec_hdr", fontName="Helvetica-Bold",
fontSize=9, textColor=C_WHITE,
alignment=TA_CENTER, spaceAfter=1,
spaceBefore=1),
"body": ParagraphStyle("body", fontName="Helvetica",
fontSize=7.5, leading=10,
textColor=C_NAVY, spaceAfter=2),
"body_sm": ParagraphStyle("body_sm", fontName="Helvetica",
fontSize=6.8, leading=9,
textColor=C_NAVY),
"bold_sm": ParagraphStyle("bold_sm", fontName="Helvetica-Bold",
fontSize=7.5, leading=10,
textColor=C_NAVY),
"red": ParagraphStyle("red", fontName="Helvetica-Bold",
fontSize=7.5, textColor=C_RED),
"green": ParagraphStyle("green", fontName="Helvetica-Bold",
fontSize=7.5, textColor=C_GREEN),
"teal": ParagraphStyle("teal", fontName="Helvetica-Bold",
fontSize=7.5, textColor=C_TEAL),
"footer": ParagraphStyle("footer", fontName="Helvetica",
fontSize=6, textColor=colors.grey,
alignment=TA_CENTER),
"wave_label": ParagraphStyle("wave_label", fontName="Helvetica-Bold",
fontSize=8, textColor=C_WHITE,
alignment=TA_CENTER),
"cell_hdr": ParagraphStyle("cell_hdr", fontName="Helvetica-Bold",
fontSize=7, textColor=C_WHITE,
alignment=TA_CENTER),
"cell_body": ParagraphStyle("cell_body", fontName="Helvetica",
fontSize=6.8, leading=9,
textColor=C_NAVY),
"cell_bold": ParagraphStyle("cell_bold", fontName="Helvetica-Bold",
fontSize=6.8, leading=9,
textColor=C_NAVY),
"cell_red": ParagraphStyle("cell_red", fontName="Helvetica-Bold",
fontSize=6.8, textColor=C_RED),
"cell_green": ParagraphStyle("cell_green", fontName="Helvetica-Bold",
fontSize=6.8, textColor=C_GREEN),
"mem": ParagraphStyle("mem", fontName="Helvetica-Oblique",
fontSize=7, textColor=C_PURPLE, leading=9),
}
S = make_styles()
# ── Section header banner ────────────────────────────────────────────────────
def section_header(text, bg=C_NAVY, fg=C_WHITE, width=None):
w = width or (W - 2*cm)
return Table(
[[Paragraph(text, ParagraphStyle("sh", fontName="Helvetica-Bold",
fontSize=9, textColor=fg,
alignment=TA_CENTER))]],
colWidths=[w],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), bg),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
])
)
# ── Waveform ASCII art drawn with canvas ──────────────────────────────────
class ECGWaveformArt(Flowable):
"""Draws a simple ECG waveform sketch using reportlab canvas primitives."""
def __init__(self, width=160*mm, height=28*mm):
super().__init__()
self.width = width
self.height = height
def draw(self):
c = self.canv
w, h = self.width, self.height
base = h * 0.35 # baseline y
# background
c.setFillColor(C_NAVY)
c.rect(0, 0, w, h, fill=1, stroke=0)
# grid lines
c.setStrokeColor(HexColor("#1A3A5C"))
c.setLineWidth(0.3)
for i in range(0, int(w), int(5*mm)):
c.line(i, 0, i, h)
for j in range(0, int(h), int(5*mm)):
c.line(0, j, w, j)
# ECG trace
c.setStrokeColor(HexColor("#00E5FF"))
c.setLineWidth(1.4)
scale = mm
# baseline lead-in
pts = [
(5*scale, base),
(20*scale, base),
# P wave (small hump)
(22*scale, base),
(24*scale, base + 5*scale),
(26*scale, base),
# PR segment
(30*scale, base),
# Q dip
(31*scale, base - 2*scale),
# R peak
(32.5*scale, base + 16*scale),
# S dip
(34*scale, base - 3*scale),
# ST segment
(36*scale, base),
(42*scale, base),
# T wave
(44*scale, base),
(47*scale, base + 6*scale),
(50*scale, base),
# U wave (small)
(53*scale, base + 1.5*scale),
(55*scale, base),
# baseline
(65*scale, base),
# 2nd beat: P
(67*scale, base),
(69*scale, base + 5*scale),
(71*scale, base),
(75*scale, base),
(76*scale, base - 2*scale),
(77.5*scale, base + 16*scale),
(79*scale, base - 3*scale),
(81*scale, base),
(87*scale, base),
(89*scale, base),
(92*scale, base + 6*scale),
(95*scale, base),
(100*scale, base),
]
p = c.beginPath()
p.moveTo(*pts[0])
for x, y in pts[1:]:
p.lineTo(x, y)
c.drawPath(p, stroke=1, fill=0)
# Labels
c.setFont("Helvetica-Bold", 6.5)
c.setFillColor(HexColor("#FFD700"))
labels = [
("P", 24*scale, base + 7*scale),
("Q", 31*scale, base - 5.5*scale),
("R", 32.5*scale, base + 18*scale),
("S", 34*scale, base - 5.5*scale),
("T", 47*scale, base + 8.5*scale),
("U", 53*scale, base + 3.5*scale),
]
for lbl, lx, ly in labels:
c.drawCentredString(lx, ly, lbl)
# Interval arrows
c.setStrokeColor(HexColor("#FF6B6B"))
c.setLineWidth(0.7)
# PR interval arrow
arrow_y = base - 8*scale
c.line(22*scale, arrow_y, 30*scale, arrow_y)
c.drawCentredString(26*scale, arrow_y - 4*scale, "PR int.")
# QRS interval
arrow_y2 = base - 11*scale
c.setStrokeColor(HexColor("#90EE90"))
c.line(31*scale, arrow_y2, 36*scale, arrow_y2)
c.setFont("Helvetica-Bold", 6)
c.setFillColor(HexColor("#90EE90"))
c.drawCentredString(33.5*scale, arrow_y2 - 4*scale, "QRS")
# QT interval
c.setStrokeColor(HexColor("#FFA500"))
c.line(31*scale, 3*scale, 50*scale, 3*scale)
c.setFillColor(HexColor("#FFA500"))
c.drawCentredString(40.5*scale, 0.5*scale, "QT interval")
# ST segment label
c.setFillColor(HexColor("#FFFFFF"))
c.setFont("Helvetica", 6)
c.drawCentredString(39*scale, base + 3*scale, "ST")
# ── Page 1 content ───────────────────────────────────────────────────────────
def build_page1(S):
story = []
col_w = (W - 2*cm) / 2 - 2*mm
# ── HEADER BANNER ──────────────────────────────────────────────
header_table = Table(
[[Paragraph("ECG QUICK-REFERENCE CHEAT SHEET", S["title"]),
Paragraph("Harrison's / Goldberger | For Educational Use", S["subtitle"])]],
colWidths=[W - 2*cm],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_NAVY),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("SPAN", (0,0), (-1,-1)),
])
)
story.append(header_table)
story.append(Spacer(1, 3*mm))
# ── WAVEFORM DIAGRAM ──────────────────────────────────────────
story.append(ECGWaveformArt(width=W - 2*cm, height=30*mm))
story.append(Spacer(1, 3*mm))
# ── WAVES & INTERVALS TABLE ───────────────────────────────────
story.append(section_header("WAVES, SEGMENTS & INTERVALS", C_TEAL))
story.append(Spacer(1, 1.5*mm))
wi_data = [
[Paragraph("Feature", S["cell_hdr"]),
Paragraph("Represents", S["cell_hdr"]),
Paragraph("Normal Values", S["cell_hdr"]),
Paragraph("Abnormal = Think...", S["cell_hdr"])],
[Paragraph("P wave", S["cell_bold"]),
Paragraph("Atrial depolarisation", S["cell_body"]),
Paragraph("< 0.12s wide\n< 2.5 mm tall\nUpright in II", S["cell_body"]),
Paragraph("Absent → AF\nTall → RAE\nWide/notched → LAE", S["cell_body"])],
[Paragraph("PR interval", S["cell_bold"]),
Paragraph("AV node conduction delay", S["cell_body"]),
Paragraph("0.12 – 0.20 s\n(3–5 small boxes)", S["cell_body"]),
Paragraph("Long → AV block\nShort → WPW / pre-excitation", S["cell_body"])],
[Paragraph("QRS complex", S["cell_bold"]),
Paragraph("Ventricular depolarisation", S["cell_body"]),
Paragraph("< 0.12 s narrow\n(< 3 small boxes)", S["cell_body"]),
Paragraph("Wide → BBB, V-tach\nDeep Q → old MI", S["cell_body"])],
[Paragraph("ST segment", S["cell_bold"]),
Paragraph("Ventricular plateau (isoelectric)", S["cell_body"]),
Paragraph("Flat at baseline\n(isoelectric)", S["cell_body"]),
Paragraph("Elevation ≥1mm → STEMI (emergency!)\nDepression → ischaemia / NSTEMI", S["cell_red"])],
[Paragraph("T wave", S["cell_bold"]),
Paragraph("Ventricular repolarisation", S["cell_body"]),
Paragraph("Upright, same dir. as QRS\nRounded", S["cell_body"]),
Paragraph("Inverted → ischaemia / BBB\nPeaked → Hyperkalaemia\nFlat → Hypokalaemia", S["cell_body"])],
[Paragraph("QTc interval", S["cell_bold"]),
Paragraph("Total ventricular electrical cycle", S["cell_body"]),
Paragraph("< 440 ms (men)\n< 460 ms (women)", S["cell_body"]),
Paragraph("Prolonged → Torsades risk\n(drugs, electrolytes, congenital)", S["cell_body"])],
[Paragraph("U wave", S["cell_bold"]),
Paragraph("Purkinje repolarisation", S["cell_body"]),
Paragraph("Small, same dir. as T\n(may be absent)", S["cell_body"]),
Paragraph("Prominent → Hypokalaemia", S["cell_body"])],
]
wi_table = Table(wi_data, colWidths=[2.5*cm, 3.5*cm, 3.5*cm, 5.5*cm])
wi_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_TEAL),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LBLUE]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("LINEBELOW", (0,0), (-1,0), 1, C_NAVY),
]))
story.append(wi_table)
story.append(Spacer(1, 3*mm))
# ── TWO COLUMNS: Heart Rate + Rhythm ──────────────────────────
# Heart rate column
hr_header = section_header("HEART RATE CALCULATION", C_ORANGE, width=col_w)
hr_data = [
[Paragraph("Large boxes (R-R)", S["cell_bold"]),
Paragraph("Rate (bpm)", S["cell_hdr"])],
[Paragraph("1", S["cell_body"]), Paragraph("300", S["cell_red"])],
[Paragraph("2", S["cell_body"]), Paragraph("150", S["cell_red"])],
[Paragraph("3", S["cell_body"]), Paragraph("100", S["cell_body"])],
[Paragraph("4", S["cell_body"]), Paragraph("75", S["cell_green"])],
[Paragraph("5", S["cell_body"]), Paragraph("60", S["cell_green"])],
[Paragraph("6", S["cell_body"]), Paragraph("50", S["cell_body"])],
]
hr_table = Table(hr_data, colWidths=[col_w*0.55, col_w*0.45])
hr_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_ORANGE),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LORANGE]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("ALIGN", (1,0), (1,-1), "CENTER"),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING", (0,0), (-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 4),
]))
hr_note = Paragraph(
"<b>Irregular rhythm:</b> Count QRS in 10-sec strip × 6\n"
"<b>Normal:</b> 60–100 bpm <b>Brady:</b> <60 <b>Tachy:</b> >100",
S["body_sm"])
# Rhythm column
rhy_header = section_header("RHYTHM QUICK ID", C_PURPLE, width=col_w)
rhy_data = [
[Paragraph("Pattern", S["cell_hdr"]),
Paragraph("Likely Rhythm", S["cell_hdr"])],
[Paragraph("Regular, P before QRS, rate 60-100", S["cell_body"]),
Paragraph("Normal Sinus Rhythm", S["cell_green"])],
[Paragraph("No P waves, irregularly irregular", S["cell_body"]),
Paragraph("Atrial Fibrillation", S["cell_red"])],
[Paragraph("Sawtooth P waves ~300/min, 2:1 block", S["cell_body"]),
Paragraph("Atrial Flutter", S["cell_red"])],
[Paragraph("PR lengthens then dropped beat", S["cell_body"]),
Paragraph("Mobitz I (Wenckebach)", S["cell_body"])],
[Paragraph("Constant PR, then sudden dropped QRS", S["cell_body"]),
Paragraph("Mobitz II (dangerous)", S["cell_red"])],
[Paragraph("P & QRS march independently", S["cell_body"]),
Paragraph("Complete (3rd degree) Block", S["cell_red"])],
[Paragraph("Wide QRS, fast, regular", S["cell_body"]),
Paragraph("Ventricular Tachycardia (VT)", S["cell_red"])],
[Paragraph("No organised activity, wavy baseline", S["cell_body"]),
Paragraph("Ventricular Fibrillation (VF)", S["cell_red"])],
]
rhy_table = Table(rhy_data, colWidths=[col_w*0.58, col_w*0.42])
rhy_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_PURPLE),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LPURP]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING", (0,0), (-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
two_col = Table(
[[KeepTogether([hr_header, Spacer(1, 1.5*mm), hr_table, Spacer(1, 2*mm), hr_note]),
KeepTogether([rhy_header, Spacer(1, 1.5*mm), rhy_table])]],
colWidths=[col_w + 2*mm, col_w + 2*mm],
style=TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 3*mm),
("TOPPADDING", (0,0), (-1,-1), 0),
("BOTTOMPADDING", (0,0), (-1,-1), 0),
])
)
story.append(two_col)
return story
# ── Page 2 content ───────────────────────────────────────────────────────────
def build_page2(S):
story = []
story.append(PageBreak())
col_w = (W - 2*cm) / 2 - 2*mm
# ── AXIS TABLE ────────────────────────────────────────────────
story.append(section_header("QRS AXIS (Leads I & aVF)", C_TEAL))
story.append(Spacer(1, 1.5*mm))
ax_data = [
[Paragraph("Lead I", S["cell_hdr"]),
Paragraph("Lead aVF", S["cell_hdr"]),
Paragraph("Axis", S["cell_hdr"]),
Paragraph("Think of...", S["cell_hdr"])],
[Paragraph("↑ Positive", S["cell_body"]), Paragraph("↑ Positive", S["cell_body"]),
Paragraph("Normal (-30° to +90°)", S["cell_green"]), Paragraph("Normal heart", S["cell_body"])],
[Paragraph("↑ Positive", S["cell_body"]), Paragraph("↓ Negative", S["cell_body"]),
Paragraph("Left Axis Deviation (LAD)", S["cell_body"]),
Paragraph("LAFB, inferior MI, LVH", S["cell_body"])],
[Paragraph("↓ Negative", S["cell_body"]), Paragraph("↑ Positive", S["cell_body"]),
Paragraph("Right Axis Deviation (RAD)", S["cell_body"]),
Paragraph("RVH, PE, LPFB, tall/thin normal", S["cell_body"])],
[Paragraph("↓ Negative", S["cell_body"]), Paragraph("↓ Negative", S["cell_body"]),
Paragraph("Extreme / NW Axis", S["cell_red"]),
Paragraph("Ventricular tachycardia, dextrocardia", S["cell_body"])],
]
ax_table = Table(ax_data, colWidths=[3*cm, 3*cm, 5*cm, 4.5*cm])
ax_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_TEAL),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LTEAL]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
]))
story.append(ax_table)
story.append(Spacer(1, 3*mm))
# ── TWO COLUMNS: ST changes + Bundle Branch Blocks ───────────
# ST changes
st_header = section_header("ST CHANGES & ISCHAEMIA", C_RED, width=col_w)
st_data = [
[Paragraph("Finding", S["cell_hdr"]), Paragraph("Meaning", S["cell_hdr"])],
[Paragraph("ST elevation ≥ 1 mm\n(≥ 2 mm in V1-V3) in ≥2\nconsecutive leads",
S["cell_red"]),
Paragraph("STEMI — call code NOW\nEmergency revascularisation", S["cell_red"])],
[Paragraph("Diffuse ST elevation +\nPR depression", S["cell_body"]),
Paragraph("Pericarditis\n(saddle-shaped)", S["cell_body"])],
[Paragraph("ST depression\n(horizontal/downsloping)", S["cell_body"]),
Paragraph("NSTEMI / Unstable angina\nDigoxin effect (upsloping)", S["cell_body"])],
[Paragraph("Deep T-wave inversion\nV2-V3 (Wellens sign)", S["cell_red"]),
Paragraph("Critical LAD stenosis\nPre-infarction — urgent!", S["cell_red"])],
[Paragraph("ST depression + tall\nR wave in V1", S["cell_body"]),
Paragraph("Posterior MI (mirror image)\nGet posterior leads V7-V9", S["cell_body"])],
]
st_table = Table(st_data, colWidths=[col_w*0.5, col_w*0.5])
st_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_RED),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LRED]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
# Bundle Branch Blocks
bbb_header = section_header("BUNDLE BRANCH BLOCKS (BBB)", C_PURPLE, width=col_w)
bbb_data = [
[Paragraph("Feature", S["cell_hdr"]),
Paragraph("RBBB", S["cell_hdr"]),
Paragraph("LBBB", S["cell_hdr"])],
[Paragraph("QRS width", S["cell_bold"]),
Paragraph("≥ 0.12 s", S["cell_body"]),
Paragraph("≥ 0.12 s", S["cell_body"])],
[Paragraph("V1 pattern", S["cell_bold"]),
Paragraph("rSR' (\"bunny ears\")", S["cell_body"]),
Paragraph("QS or rS (W-shape)", S["cell_body"])],
[Paragraph("V6 pattern", S["cell_bold"]),
Paragraph("Wide S wave", S["cell_body"]),
Paragraph("Broad R (M-shape)", S["cell_body"])],
[Paragraph("Mnemonic", S["cell_bold"]),
Paragraph("WiRRy\n(Wide R in Right V1)", S["mem"]),
Paragraph("WiLLiaM\n(W in V1, M in V6)", S["mem"])],
[Paragraph("Clinical", S["cell_bold"]),
Paragraph("Often benign; watch for new RBBB", S["cell_body"]),
Paragraph("Do NOT diagnose MI on LBBB ECG", S["cell_red"])],
]
bbb_table = Table(bbb_data, colWidths=[col_w*0.3, col_w*0.35, col_w*0.35])
bbb_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_PURPLE),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LPURP]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING", (0,0), (-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
two_col = Table(
[[KeepTogether([st_header, Spacer(1, 1.5*mm), st_table]),
KeepTogether([bbb_header, Spacer(1, 1.5*mm), bbb_table])]],
colWidths=[col_w + 2*mm, col_w + 2*mm],
style=TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 3*mm),
("TOPPADDING", (0,0), (-1,-1), 0),
("BOTTOMPADDING", (0,0), (-1,-1), 0),
])
)
story.append(two_col)
story.append(Spacer(1, 3*mm))
# ── TWO COLUMNS: Electrolytes + Lead Territories ──────────────
# Electrolytes
elec_header = section_header("ELECTROLYTE ECG CHANGES", C_GREEN, width=col_w)
elec_data = [
[Paragraph("Electrolyte", S["cell_hdr"]),
Paragraph("ECG Finding", S["cell_hdr"])],
[Paragraph("Hyperkalaemia ↑K+", S["cell_bold"]),
Paragraph("Peaked T → wide QRS → sine wave → VF", S["cell_red"])],
[Paragraph("Hypokalaemia ↓K+", S["cell_bold"]),
Paragraph("Flat T, prominent U wave, long QT", S["cell_body"])],
[Paragraph("Hypercalcaemia ↑Ca2+", S["cell_bold"]),
Paragraph("Short QT interval", S["cell_body"])],
[Paragraph("Hypocalcaemia ↓Ca2+", S["cell_bold"]),
Paragraph("Prolonged QT interval", S["cell_body"])],
[Paragraph("Hypomagnesaemia ↓Mg2+", S["cell_bold"]),
Paragraph("Long QT, Torsades de Pointes risk", S["cell_red"])],
[Paragraph("Digoxin toxicity", S["cell_bold"]),
Paragraph("\"Salvador Dali\" ST (scooped), short QT,\nbradyarrhythmias", S["cell_body"])],
]
elec_table = Table(elec_data, colWidths=[col_w*0.42, col_w*0.58])
elec_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_GREEN),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LGREEN]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING", (0,0), (-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
# Lead territories
terr_header = section_header("LEAD TERRITORIES (MI Localisation)", C_ORANGE, width=col_w)
terr_data = [
[Paragraph("Territory", S["cell_hdr"]),
Paragraph("Leads", S["cell_hdr"]),
Paragraph("Artery", S["cell_hdr"])],
[Paragraph("Inferior", S["cell_bold"]),
Paragraph("II, III, aVF", S["cell_body"]),
Paragraph("RCA", S["cell_body"])],
[Paragraph("Anterior", S["cell_bold"]),
Paragraph("V1 – V4", S["cell_body"]),
Paragraph("LAD", S["cell_body"])],
[Paragraph("Lateral", S["cell_bold"]),
Paragraph("I, aVL, V5, V6", S["cell_body"]),
Paragraph("LCx", S["cell_body"])],
[Paragraph("Anterolateral", S["cell_bold"]),
Paragraph("V1–V6, I, aVL", S["cell_body"]),
Paragraph("LAD/LCx", S["cell_body"])],
[Paragraph("Posterior", S["cell_bold"]),
Paragraph("V7–V9 (posterior leads)\nMirror: tall R + ST dep in V1-V2", S["cell_body"]),
Paragraph("RCA/LCx", S["cell_body"])],
[Paragraph("RV infarct", S["cell_bold"]),
Paragraph("V3R, V4R (right-sided leads)", S["cell_body"]),
Paragraph("RCA (proximal)", S["cell_red"])],
]
terr_table = Table(terr_data, colWidths=[col_w*0.28, col_w*0.43, col_w*0.29])
terr_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_ORANGE),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_LORANGE]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING", (0,0), (-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
two_col2 = Table(
[[KeepTogether([elec_header, Spacer(1, 1.5*mm), elec_table]),
KeepTogether([terr_header, Spacer(1, 1.5*mm), terr_table])]],
colWidths=[col_w + 2*mm, col_w + 2*mm],
style=TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 3*mm),
("TOPPADDING", (0,0), (-1,-1), 0),
("BOTTOMPADDING", (0,0), (-1,-1), 0),
])
)
story.append(two_col2)
story.append(Spacer(1, 3*mm))
# ── SYSTEMATIC APPROACH BANNER ────────────────────────────────
story.append(section_header("7-STEP SYSTEMATIC APPROACH", C_NAVY))
story.append(Spacer(1, 1.5*mm))
steps = [
("1", "RATE", "Count large boxes between R-R peaks; divide 300 by that number. Irregular? Count QRS in 10 s × 6."),
("2", "RHYTHM", "Are R-R intervals regular? Is there a P before every QRS? QRS after every P? → Normal sinus or arrhythmia?"),
("3", "AXIS", "Leads I and aVF: both positive = normal. I+/aVF- = LAD. I-/aVF+ = RAD. Both negative = extreme."),
("4", "INTERVALS", "PR: 0.12–0.20 s. QRS: <0.12 s. QTc: <440 ms men / <460 ms women. Long QRS = BBB."),
("5", "P WAVES", "Upright in II? Present before every QRS? Width/height normal? Abnormal → atrial issues or non-sinus rhythm."),
("6", "ST & T WAVES", "Flat ST baseline? Any elevation or depression? T wave direction and shape? This step catches MI and ischaemia."),
("7", "SPECIAL", "Hypertrophy criteria? Bundle branch block? Electrolyte pattern? Delta waves (WPW)? Clinical context?"),
]
step_data = [[
Paragraph(f"<b>{num}</b>", ParagraphStyle("sn", fontName="Helvetica-Bold",
fontSize=10, textColor=C_WHITE, alignment=TA_CENTER)),
Paragraph(f"<b>{name}</b>", ParagraphStyle("sn2", fontName="Helvetica-Bold",
fontSize=8, textColor=C_YELLOW)),
Paragraph(desc, S["cell_body"]),
] for num, name, desc in steps]
step_table = Table(step_data, colWidths=[0.8*cm, 2.5*cm, W - 2*cm - 3.3*cm])
step_table.setStyle(TableStyle([
("ROWBACKGROUNDS", (0,0), (-1,-1), [C_NAVY, HexColor("#162944")]),
("GRID", (0,0), (-1,-1), 0.3, HexColor("#2C4A6A")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("TEXTCOLOR", (2,0), (2,-1), C_WHITE),
]))
story.append(step_table)
story.append(Spacer(1, 2*mm))
# ── FOOTER ────────────────────────────────────────────────────
story.append(HRFlowable(width=W - 2*cm, thickness=0.5, color=colors.grey))
story.append(Spacer(1, 1*mm))
story.append(Paragraph(
"For educational use only. Not a substitute for clinical judgment. "
"Sources: Harrison's Principles of Internal Medicine 22E (2025) | "
"Goldberger's Clinical Electrocardiography 10E (2024)",
S["footer"]))
return story
# ── Page canvas decoration ───────────────────────────────────────────────────
def add_page_decorations(canvas_obj, doc):
"""Add page number and thin border to each page."""
canvas_obj.saveState()
# thin border
canvas_obj.setStrokeColor(C_NAVY)
canvas_obj.setLineWidth(1.5)
canvas_obj.rect(0.5*cm, 0.5*cm, W - 1*cm, H - 1*cm, stroke=1, fill=0)
# page number
canvas_obj.setFont("Helvetica", 7)
canvas_obj.setFillColor(colors.grey)
canvas_obj.drawRightString(W - 0.8*cm, 0.65*cm,
f"Page {doc.page}")
canvas_obj.restoreState()
# ── Main ─────────────────────────────────────────────────────────────────────
def main():
out_path = "/home/daytona/workspace/ecg-cheatsheet/ECG_QuickReference.pdf"
doc = SimpleDocTemplate(
out_path,
pagesize=A4,
leftMargin=1*cm,
rightMargin=1*cm,
topMargin=1*cm,
bottomMargin=1.2*cm,
title="ECG Quick-Reference Cheat Sheet",
author="Orris Medical Education",
subject="ECG Interpretation",
)
story = build_page1(S) + build_page2(S)
doc.build(story, onFirstPage=add_page_decorations,
onLaterPages=add_page_decorations)
print(f"PDF generated: {out_path}")
if __name__ == "__main__":
main()
cd /home/daytona/workspace/ecg-cheatsheet && python3 generate_ecg_cheatsheet.py 2>&1
~/ecg-cheatsheet/generate_ecg_cheatsheet.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/ecg-cheatsheet/generate_ecg_cheatsheet.py'
~/ecg-cheatsheet/generate_ecg_cheatsheet.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/ecg-cheatsheet/generate_ecg_cheatsheet.py'
~/ecg-cheatsheet/generate_ecg_cheatsheet.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/ecg-cheatsheet/generate_ecg_cheatsheet.py'
cd /home/daytona/workspace/ecg-cheatsheet && python3 generate_ecg_cheatsheet.py 2>&1
ls -lh /home/daytona/workspace/ecg-cheatsheet/ECG_QuickReference.pdf
ECG QuickReference
PDF Document · PDF
- Color-coded header banner
- ECG waveform diagram (drawn programmatically) with P, Q, R, S, T, U labels and PR/QRS/QT interval arrows
- Waves & Intervals table - all 7 features (P wave, PR, QRS, ST, T, QTc, U) with what each represents, normal values, and what abnormalities suggest
- Heart Rate Calculator (big-box counting table + irregular method)
- Rhythm Quick-ID - 8 key rhythms from normal sinus to VF
- QRS Axis table (Leads I + aVF method, all 4 quadrants)
- ST Changes & Ischaemia - STEMI, pericarditis, NSTEMI, Wellens sign, posterior MI
- Bundle Branch Blocks - RBBB vs LBBB comparison with WiRRy/WiLLiaM mnemonics
- Electrolyte ECG Changes - hyper/hypokalaemia, calcium, magnesium, digoxin
- Lead Territories - inferior/anterior/lateral/posterior with culprit arteries
- 7-Step Systematic Approach strip - dark navy banner summarising the full method
- Source attribution footer
Calculate the ml/hr of the following: Dobutamine stock=250mg/5ml, patient's weight = 75kg. Dose=2mcg/kg/min
Dobutamine Infusion Rate Calculation
Given Information
| Parameter | Value |
|---|---|
| Stock concentration | 250 mg / 5 ml |
| Patient weight | 75 kg |
| Prescribed dose | 2 mcg/kg/min |
Step 1 - Find the Stock Concentration in mcg/ml
Step 2 - Calculate the Dose Required per Minute
Step 3 - Convert to mcg per Hour
Step 4 - Calculate the Infusion Rate in ml/hr
Summary
| Step | Calculation | Result |
|---|---|---|
| Stock concentration | 250 mg ÷ 5 ml | 50 mg/ml = 50,000 mcg/ml |
| Required dose | 2 mcg × 75 kg | 150 mcg/min |
| Per hour | 150 × 60 | 9,000 mcg/hr |
| Infusion rate | 9,000 ÷ 50,000 | 0.18 ml/hr |
Clinical note: 0.18 ml/hr is an extremely low infusion rate that most standard syringe pumps can deliver, but always verify the pump's minimum delivery threshold (typically 0.1 ml/hr). If using a diluted solution (e.g. 250 mg in 250 ml = 1,000 mcg/ml), the rate would be 9 ml/hr - which is more practical for bedside administration. Always confirm with your institution's pharmacy protocol.
Create a reference table of common IV infusion calculations
mkdir -p /home/daytona/workspace/iv-infusion-ref
~/iv-infusion-ref/generate_iv_reference.py
#!/usr/bin/env python3
"""
IV Infusion Calculations - Clinical Reference Table PDF
Multi-page, color-coded, printable A4 reference.
"""
from reportlab.lib.pagesizes import A4, landscape
from reportlab.lib import colors
from reportlab.lib.units import mm, cm
from reportlab.lib.styles import ParagraphStyle
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT
from reportlab.lib.colors import HexColor
from reportlab.pdfgen import canvas as rl_canvas
# ── Palette ──────────────────────────────────────────────────────────────────
NAVY = HexColor("#0D2137")
TEAL = HexColor("#0A7E8C")
DKBLUE = HexColor("#1A3A6C")
RED = HexColor("#C0392B")
ORANGE = HexColor("#D35400")
GREEN = HexColor("#1A7A4A")
PURPLE = HexColor("#6C3483")
MAROON = HexColor("#7B241C")
SLATE = HexColor("#2E4057")
GOLD = HexColor("#B7950B")
LBLUE = HexColor("#EBF5FB")
LTEAL = HexColor("#E8F8F5")
LRED = HexColor("#FDEDEC")
LGREEN = HexColor("#EAFAF1")
LORANGE = HexColor("#FEF5E7")
LPURP = HexColor("#F5EEF8")
LGREY = HexColor("#F4F6F7")
LYELLOW = HexColor("#FDFBE4")
WHITE = colors.white
W, H = landscape(A4) # 297 x 210 mm landscape
# ── Paragraph Styles ─────────────────────────────────────────────────────────
def ps(name, font="Helvetica", size=7.5, color=NAVY, align=TA_LEFT,
bold=False, leading=10, space_before=0, space_after=1):
fn = "Helvetica-Bold" if bold else font
return ParagraphStyle(name, fontName=fn, fontSize=size, textColor=color,
alignment=align, leading=leading,
spaceBefore=space_before, spaceAfter=space_after)
STYLES = {
"title": ps("title", size=15, color=WHITE, align=TA_CENTER, bold=True, leading=18),
"subtitle": ps("sub", size=8, color=HexColor("#AED6F1"), align=TA_CENTER),
"sec": ps("sec", size=8.5, color=WHITE, align=TA_CENTER, bold=True, leading=11),
"hdr": ps("hdr", size=7, color=WHITE, align=TA_CENTER, bold=True, leading=9),
"body": ps("body", size=7, leading=9.5),
"bodyc": ps("bodyc", size=7, leading=9.5, align=TA_CENTER),
"bold": ps("bold", size=7, bold=True, leading=9.5),
"boldc": ps("boldc", size=7, bold=True, leading=9.5, align=TA_CENTER),
"red": ps("red", size=7, color=RED, bold=True, leading=9.5),
"redc": ps("redc", size=7, color=RED, bold=True, leading=9.5, align=TA_CENTER),
"green": ps("green", size=7, color=GREEN, bold=True, leading=9.5),
"greenc": ps("greenc", size=7, color=GREEN, bold=True, leading=9.5, align=TA_CENTER),
"orange": ps("orange", size=7, color=ORANGE, bold=True, leading=9.5),
"formula": ps("formula",size=7.5,color=NAVY, bold=True, leading=11,
font="Courier-Bold"),
"formulac": ps("formulac",size=7,color=DKBLUE, bold=True, leading=10,
font="Courier-Bold", align=TA_CENTER),
"note": ps("note", size=6, color=HexColor("#555555"), leading=8),
"notec": ps("notec", size=6, color=HexColor("#555555"), leading=8, align=TA_CENTER),
"footer": ps("footer", size=6, color=colors.grey, align=TA_CENTER),
"warn": ps("warn", size=6.5,color=RED, bold=True, leading=9),
}
S = STYLES
# ── Helper: section banner ────────────────────────────────────────────────────
def banner(text, bg=NAVY, width=None):
w = width or (W - 1.6*cm)
return Table(
[[Paragraph(text, S["sec"])]],
colWidths=[w],
style=TableStyle([
("BACKGROUND", (0,0),(-1,-1), bg),
("TOPPADDING", (0,0),(-1,-1), 4),
("BOTTOMPADDING", (0,0),(-1,-1), 4),
("LEFTPADDING", (0,0),(-1,-1), 6),
("RIGHTPADDING", (0,0),(-1,-1), 6),
])
)
# ── Helper: make a styled data table ────────────────────────────────────────
def make_table(data, col_widths, header_bg=NAVY, row_colors=(WHITE, LGREY),
grid_color=HexColor("#BFC9CA"), v_pad=3, h_pad=4):
t = Table(data, colWidths=col_widths, repeatRows=1)
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), header_bg),
("ROWBACKGROUNDS",(0,1), (-1,-1), row_colors),
("GRID", (0,0), (-1,-1), 0.4, grid_color),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), v_pad),
("BOTTOMPADDING", (0,0), (-1,-1), v_pad),
("LEFTPADDING", (0,0), (-1,-1), h_pad),
("RIGHTPADDING", (0,0), (-1,-1), h_pad),
("LINEBELOW", (0,0), (-1,0), 1, NAVY),
]))
return t
# ── Page canvas callback ──────────────────────────────────────────────────────
def page_deco(c, doc):
c.saveState()
c.setStrokeColor(NAVY)
c.setLineWidth(1.5)
c.rect(0.4*cm, 0.4*cm, W-0.8*cm, H-0.8*cm, stroke=1, fill=0)
c.setFont("Helvetica", 6.5)
c.setFillColor(colors.grey)
c.drawRightString(W-0.6*cm, 0.55*cm, f"Page {doc.page}")
c.drawString(0.6*cm, 0.55*cm, "IV Infusion Calculations Reference | For Educational Use Only")
c.restoreState()
# ══════════════════════════════════════════════════════════════════════════════
# CONTENT BUILDERS
# ══════════════════════════════════════════════════════════════════════════════
def page1_formulas(story):
"""Master formulas box + unit conversion table + drop rate table."""
# ── TITLE HEADER ──────────────────────────────────────────────────────
hdr = Table(
[[Paragraph("COMMON IV INFUSION CALCULATIONS", S["title"])],
[Paragraph(
"Clinical Reference Table | Nurses, Pharmacists & Medical Staff | "
"Always verify with local protocols and pharmacy",
S["subtitle"])]],
colWidths=[W - 1.6*cm],
style=TableStyle([
("BACKGROUND", (0,0),(-1,-1), NAVY),
("TOPPADDING", (0,0),(-1,-1), 7),
("BOTTOMPADDING", (0,0),(-1,-1), 7),
])
)
story.append(hdr)
story.append(Spacer(1, 3*mm))
# ── SECTION 1: Core Formulas ───────────────────────────────────────────
story.append(banner("SECTION 1 — MASTER FORMULAS", TEAL))
story.append(Spacer(1, 2*mm))
# Two-column formula layout
LEFT_W = (W - 1.6*cm) * 0.5 - 3*mm
RIGHT_W = (W - 1.6*cm) * 0.5 - 3*mm
formulas_left = [
("ml/hr from mcg/kg/min",
"ml/hr = (Dose mcg/kg/min x Wt kg x 60)\n"
" ----------------------------------\n"
" Concentration mcg/ml",
"Catecholamines (dopamine, dobutamine,\nnoradrenaline, adrenaline)"),
("ml/hr from mcg/min",
"ml/hr = (Dose mcg/min x 60)\n"
" -----------------------\n"
" Concentration mcg/ml",
"Non-weight-based infusions\n(e.g. GTN, sodium nitroprusside)"),
("ml/hr from mg/hr",
"ml/hr = Dose mg/hr\n"
" ---------------\n"
" Concentration mg/ml",
"Morphine, midazolam, labetalol"),
("ml/hr from units/hr",
"ml/hr = Dose units/hr\n"
" -----------------\n"
" Concentration units/ml",
"Insulin, heparin, oxytocin"),
]
formulas_right = [
("Concentration (mg/ml)",
"Concentration = Total drug (mg)\n"
" -------------------\n"
" Total volume (ml)",
"First step in ALL calculations"),
("Dose check (reverse calc)",
"Dose = ml/hr x Concentration mcg/ml\n"
" ----------------------------------\n"
" 60 x Weight kg",
"Verify the running rate makes sense"),
("Drop rate (drops/min)",
"Drops/min = Volume (ml) x Drop factor\n"
" -----------------------------\n"
" Time (min)",
"Used when IV pump not available"),
("Infusion time (hours)",
"Time (hr) = Volume (ml)\n"
" ---------------\n"
" Rate (ml/hr)",
"Estimate when a bag will finish"),
]
def formula_block(title, formula, use):
return [
Paragraph(title, S["bold"]),
Paragraph(formula, S["formulac"]),
Paragraph(f"Use: {use}", S["note"]),
]
left_cells = [formula_block(t,f,u) for t,f,u in formulas_left]
right_cells = [formula_block(t,f,u) for t,f,u in formulas_right]
def formula_table(cells, bg, row_colors):
data = [[Paragraph("Formula", S["hdr"]),
Paragraph("Expression", S["hdr"]),
Paragraph("Common Use", S["hdr"])]]
for title, formula, use in [(t,f,u) for t,f,u in
(formulas_left if bg==TEAL else formulas_right)]:
data.append([
Paragraph(title, S["bold"]),
Paragraph(formula, S["formulac"]),
Paragraph(f"Use: {use}", S["note"]),
])
return make_table(data,
[LEFT_W*0.28, LEFT_W*0.42, LEFT_W*0.30],
header_bg=bg, row_colors=row_colors)
f_left = formula_table(left_cells, TEAL, (WHITE, LTEAL))
f_right = formula_table(right_cells, DKBLUE, (WHITE, LBLUE))
two_col = Table(
[[f_left, f_right]],
colWidths=[LEFT_W + 3*mm, RIGHT_W + 3*mm],
style=TableStyle([
("VALIGN", (0,0),(-1,-1), "TOP"),
("LEFTPADDING", (0,0),(-1,-1), 0),
("RIGHTPADDING",(0,0),(-1,-1), 3*mm),
("TOPPADDING", (0,0),(-1,-1), 0),
("BOTTOMPADDING",(0,0),(-1,-1), 0),
])
)
story.append(two_col)
story.append(Spacer(1, 3*mm))
# ── SECTION 2: Unit Conversions ────────────────────────────────────────
story.append(banner("SECTION 2 — UNIT CONVERSIONS & KEY EQUIVALENCES", SLATE))
story.append(Spacer(1, 2*mm))
UC_W = W - 1.6*cm
uc_data = [
[Paragraph("From", S["hdr"]),
Paragraph("To", S["hdr"]),
Paragraph("Multiply by", S["hdr"]),
Paragraph("Example", S["hdr"]),
Paragraph("", S["hdr"]), # separator
Paragraph("From", S["hdr"]),
Paragraph("To", S["hdr"]),
Paragraph("Multiply by", S["hdr"]),
Paragraph("Example", S["hdr"])],
[Paragraph("mg", S["body"]),
Paragraph("mcg (micrograms)", S["body"]),
Paragraph("x 1,000", S["boldc"]),
Paragraph("5 mg = 5,000 mcg", S["body"]),
Paragraph("", S["body"]),
Paragraph("mcg/min", S["body"]),
Paragraph("mcg/hr", S["body"]),
Paragraph("x 60", S["boldc"]),
Paragraph("10 mcg/min = 600 mcg/hr", S["body"])],
[Paragraph("mcg", S["body"]),
Paragraph("mg", S["body"]),
Paragraph("÷ 1,000", S["boldc"]),
Paragraph("2,500 mcg = 2.5 mg", S["body"]),
Paragraph("", S["body"]),
Paragraph("mg/min", S["body"]),
Paragraph("mg/hr", S["body"]),
Paragraph("x 60", S["boldc"]),
Paragraph("2 mg/min = 120 mg/hr", S["body"])],
[Paragraph("g", S["body"]),
Paragraph("mg", S["body"]),
Paragraph("x 1,000", S["boldc"]),
Paragraph("1 g = 1,000 mg", S["body"]),
Paragraph("", S["body"]),
Paragraph("units/min", S["body"]),
Paragraph("units/hr", S["body"]),
Paragraph("x 60", S["boldc"]),
Paragraph("3 units/min = 180 units/hr", S["body"])],
[Paragraph("mg", S["body"]),
Paragraph("g", S["body"]),
Paragraph("÷ 1,000", S["boldc"]),
Paragraph("500 mg = 0.5 g", S["body"]),
Paragraph("", S["body"]),
Paragraph("mcg/kg/min", S["body"]),
Paragraph("mcg/min (70 kg)", S["body"]),
Paragraph("x 70", S["boldc"]),
Paragraph("5 mcg/kg/min = 350 mcg/min", S["body"])],
[Paragraph("nanogram (ng)", S["body"]),
Paragraph("mcg", S["body"]),
Paragraph("÷ 1,000", S["boldc"]),
Paragraph("1,000 ng = 1 mcg", S["body"]),
Paragraph("", S["body"]),
Paragraph("% solution", S["body"]),
Paragraph("mg/ml", S["body"]),
Paragraph("x 10", S["boldc"]),
Paragraph("0.9% NaCl = 9 mg/ml NaCl", S["body"])],
]
cw = UC_W / 9
uc_col_w = [cw*1.1, cw*1.4, cw*0.9, cw*1.7, cw*0.2, cw*1.1, cw*1.4, cw*0.9, cw*1.3]
uc_table = make_table(uc_data, uc_col_w, header_bg=SLATE, row_colors=(WHITE, LGREY))
# Add vertical divider styling
uc_table.setStyle(TableStyle([
("BACKGROUND", (4,0), (4,-1), HexColor("#D0D3D4")), # separator col
("BACKGROUND", (0,0), (-1,0), SLATE),
("ROWBACKGROUNDS",(0,1), (-1,-1), (WHITE, LGREY)),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("LINEBELOW", (0,0), (-1,0), 1, NAVY),
]))
story.append(uc_table)
story.append(Spacer(1, 3*mm))
# ── SECTION 3: Drop Factor / Gravity Reference ────────────────────────
story.append(banner("SECTION 3 — GRAVITY DRIP RATE (Drops/min) REFERENCE", GOLD))
story.append(Spacer(1, 2*mm))
drop_intro = Table(
[[Paragraph(
"Formula: Drops/min = Volume (ml) x Drop Factor / Time (min) "
"| Standard drop factors: Macrodrip = 10, 15, or 20 gtts/ml "
"| Microdrip = 60 gtts/ml",
S["formulac"])]],
colWidths=[W - 1.6*cm],
style=TableStyle([
("BACKGROUND", (0,0),(-1,-1), LYELLOW),
("TOPPADDING", (0,0),(-1,-1), 4),
("BOTTOMPADDING", (0,0),(-1,-1), 4),
("BOX", (0,0),(-1,-1), 0.8, GOLD),
])
)
story.append(drop_intro)
story.append(Spacer(1, 2*mm))
# Drop rate lookup table: volume vs time
volumes = [50, 100, 150, 250, 500, 1000]
times_hr = [0.5, 1, 2, 4, 6, 8]
df = 20 # drop factor for table
drop_hdr = [Paragraph("Volume (ml)", S["hdr"])]
for t in times_hr:
lbl = f"{int(t*60)} min" if t < 1 else f"{int(t)} hr"
drop_hdr.append(Paragraph(lbl, S["hdr"]))
drop_data = [drop_hdr]
for vol in volumes:
row = [Paragraph(str(vol), S["boldc"])]
for t in times_hr:
mins = t * 60
rate = (vol * df) / mins
style = S["redc"] if rate > 60 else (S["greenc"] if rate <= 30 else S["bodyc"])
row.append(Paragraph(f"{rate:.0f}", style))
drop_data.append(row)
drop_note_row = [
Paragraph("", S["note"]),
Paragraph("", S["note"]),
Paragraph("Red = >60 drops/min (difficult to count)", S["warn"]),
Paragraph("", S["note"]),
Paragraph("Green = ≤30 drops/min (easy to count)", S["note"]),
Paragraph("", S["note"]),
Paragraph("", S["note"]),
]
dcw = (W - 1.6*cm) / 7
drop_table = make_table(drop_data, [dcw]*7, header_bg=GOLD,
row_colors=(WHITE, LYELLOW))
story.append(Paragraph(
f"Drop rate lookup table (drop factor = {df} gtts/ml) — values in drops/min",
S["notec"]))
story.append(Spacer(1, 1*mm))
story.append(drop_table)
def page2_drugs(story):
"""Common IV drugs: standard dilutions, dose ranges, infusion rates."""
story.append(PageBreak())
# ── SECTION 4: Common IV Drug Reference ──────────────────────────────
story.append(banner("SECTION 4 — COMMON IV DRUG INFUSIONS: STANDARD DILUTIONS & DOSE RANGES", RED))
story.append(Spacer(1, 2*mm))
story.append(Paragraph(
"Note: Concentrations vary by institution. Always check local formulary. "
"Worked ml/hr values use a 70 kg patient for weight-based drugs.",
S["warn"]))
story.append(Spacer(1, 2*mm))
# Data: [Drug, Category, Stock, Standard dilution, Usual dose range,
# Concentration, Example ml/hr (70kg), Key nursing notes]
drug_data_raw = [
# VASOPRESSORS / INOTROPES
("Noradrenaline\n(Norepinephrine)", "Vasopressor",
"4 mg / 4 ml (1 mg/ml)", "4 mg in 48 ml NS = 50 ml\n(80 mcg/ml)",
"0.01–3 mcg/kg/min", "80 mcg/ml",
"0.01 x 70 x 60 / 80 = 0.5 ml/hr\n(at 0.01 mcg/kg/min)",
"Central line only. Titrate to MAP ≥65. Monitor for peripheral ischaemia."),
("Adrenaline\n(Epinephrine)", "Vasopressor/Inotrope",
"1 mg/ml ampoule", "1 mg in 49 ml NS = 50 ml\n(20 mcg/ml)",
"0.01–1 mcg/kg/min", "20 mcg/ml",
"0.1 x 70 x 60 / 20 = 21 ml/hr\n(at 0.1 mcg/kg/min)",
"Central line preferred. Risk of arrhythmia. Monitor lactate."),
("Dopamine", "Vasopressor/Inotrope",
"200 mg / 5 ml (40 mg/ml)", "200 mg in 45 ml NS = 50 ml\n(4,000 mcg/ml)",
"2–20 mcg/kg/min", "4,000 mcg/ml",
"5 x 70 x 60 / 4000 = 5.25 ml/hr\n(at 5 mcg/kg/min)",
"Low dose (2-5): renal. Mid (5-10): cardiac. High (>10): vasopressor."),
("Dobutamine", "Inotrope",
"250 mg / 5 ml (50 mg/ml)", "250 mg in 45 ml NS = 50 ml\n(5,000 mcg/ml)",
"2–20 mcg/kg/min", "5,000 mcg/ml",
"5 x 70 x 60 / 5000 = 4.2 ml/hr\n(at 5 mcg/kg/min)",
"May cause tachycardia. Monitor BP closely. Not for obstructive cardiomyopathy."),
("Vasopressin", "Vasopressor",
"20 units / ml", "20 units in 30 ml NS = 50 ml\n(0.4 units/ml)",
"0.01–0.04 units/min\n(fixed dose, NOT wt-based)", "0.4 units/ml",
"0.04 units/min x 60 / 0.4 = 6 ml/hr\n(at 0.04 units/min)",
"Fixed dose adjunct in septic shock. Mesenteric ischaemia risk."),
# ANTIARRHYTHMICS
("Amiodarone", "Antiarrhythmic",
"150 mg / 3 ml (50 mg/ml)", "300 mg in 250 ml D5W\n(1.2 mg/ml)",
"Load: 5 mg/kg over 1 hr\nMaint: 10-20 mg/kg/day", "1.2 mg/ml",
"Load 70 kg: 350 mg over 1 hr\n= 350/1.2 = 292 ml/hr x 1 hr",
"Vesicant — use central line for prolonged infusion. Prolongs QT. Check TFTs."),
("Lignocaine\n(Lidocaine)", "Antiarrhythmic",
"200 mg / 10 ml (20 mg/ml)", "1 g in 500 ml NS\n(2 mg/ml)",
"1–4 mg/min", "2 mg/ml",
"2 mg/min x 60 / 2 = 60 ml/hr", "Monitor for toxicity: tinnitus, seizures. Reduce in liver failure."),
# ANTICOAGULANTS
("Unfractionated\nHeparin", "Anticoagulant",
"1,000 units/ml or\n5,000 units/ml", "25,000 units in 50 ml NS\n(500 units/ml)",
"Per weight-based protocol\n(e.g. 18 units/kg/hr start)", "500 units/ml",
"18 x 70 / 500 = 2.5 ml/hr\n(initial rate)",
"Monitor APTT 6-hrly. Target APTT ratio 1.5-2.5. Adjust per protocol."),
# SEDATION / ANALGESIA
("Morphine", "Opioid Analgesic",
"10 mg / ml ampoule", "50 mg in 50 ml NS\n(1 mg/ml)",
"0–10 mg/hr (adult)\nOR PCA protocol", "1 mg/ml",
"5 mg/hr / 1 mg/ml = 5 ml/hr", "Titrate to pain score. Monitor respiratory rate, GCS. Naloxone on hand."),
("Fentanyl", "Opioid Analgesic",
"500 mcg / 10 ml\n(50 mcg/ml)", "500 mcg in 50 ml NS\n(10 mcg/ml)",
"25–200 mcg/hr", "10 mcg/ml",
"50 mcg/hr / 10 mcg/ml = 5 ml/hr", "ICU analgesia. Chest wall rigidity at high doses. Titrate cautiously."),
("Midazolam", "Benzodiazepine Sedative",
"5 mg/ml ampoule", "50 mg in 50 ml NS\n(1 mg/ml)",
"0.01–0.1 mg/kg/hr", "1 mg/ml",
"0.05 x 70 / 1 = 3.5 ml/hr\n(at 0.05 mg/kg/hr)",
"Titrate to RASS/Richmond scale. Accumulates in renal/hepatic failure."),
("Propofol", "IV Anaesthetic/Sedative",
"10 mg/ml emulsion\n(ready to use)", "Use undiluted\n(10 mg/ml)",
"0.5–4 mg/kg/hr (ICU)\n1–4 mg/kg/hr (GA)", "10 mg/ml",
"1 mg/kg/hr x 70 / 10 = 7 ml/hr\n(at 1 mg/kg/hr)",
"Propofol infusion syndrome at >4 mg/kg/hr > 48 hrs. Provides calories (1.1 kcal/ml)."),
# VASODILATORS
("GTN\n(Glyceryl Trinitrate)", "Vasodilator",
"5 mg / ml ampoule", "50 mg in 50 ml NS\n(1,000 mcg/ml) or\n50 mg in 500 ml = 100 mcg/ml",
"10–200 mcg/min", "1,000 mcg/ml\n(concentrated)\nOR 100 mcg/ml",
"100 mcg/min x 60 / 1000 = 6 ml/hr\n(concentrated bag)",
"Non-PVC tubing required. Tolerance after 24 hrs. Monitor BP closely."),
("Labetalol", "Alpha/Beta-Blocker",
"5 mg / ml ampoule", "200 mg in 200 ml NS\n(1 mg/ml)",
"0.5–2 mg/min", "1 mg/ml",
"1 mg/min x 60 / 1 = 60 ml/hr", "Hypertensive emergency/eclampsia. Avoid in asthma, severe bradycardia."),
# ELECTROLYTES / OTHERS
("Potassium Chloride\n(KCl)", "Electrolyte",
"1 mmol/ml (ready-to-use)", "NEVER give undiluted!\n20 mmol in 100 ml or 250 ml",
"Max 10 mmol/hr peripheral\nMax 20 mmol/hr central", "0.1 mmol/ml (100 ml bag)\nor 0.08 mmol/ml (250 ml)",
"10 mmol/hr: 100 ml/hr (peripheral)\n20 mmol/hr: 100 ml/hr (central, 250 ml bag)",
"FATAL if given undiluted IV push! Cardiac monitoring required >10 mmol/hr."),
("Insulin (Actrapid)", "Hormone",
"100 units/ml", "50 units in 50 ml NS\n(1 unit/ml)",
"Vary by BGL protocol\n(0.5–10 units/hr typical)", "1 unit/ml",
"2 units/hr / 1 unit/ml = 2 ml/hr", "BGL every 1-2 hr. Separate flush syringe. Insulin adheres to PVC tubing."),
("Magnesium Sulphate", "Electrolyte/Tocolytic",
"2 g / 10 ml\n(0.2 g/ml)", "8 g in 100 ml NS\n(0.08 g/ml)\nor per protocol",
"Loading: 4 g over 20 min\nMaint: 1–2 g/hr", "0.08 g/ml",
"1 g/hr: 12.5 ml/hr (in 0.08 g/ml bag)", "Eclampsia: loading dose 4 g IV. Monitor reflexes, resp rate, urine output. Antidote: calcium gluconate."),
("Oxytocin\n(Syntocinon)", "Uterotonic",
"10 units / ml", "30 units in 500 ml NS\n(0.06 units/ml)",
"Labour: 1–20 milliunits/min\nPost-partum: per protocol", "0.06 units/ml\n= 60 milliunits/ml",
"6 milliunits/min x 60 / 60 = 6 ml/hr\n(at 6 milliunits/min)",
"Electronic pump mandatory. Monitor uterine tone and CTG. Risk of uterine hyperstimulation."),
]
drug_hdr = [
Paragraph("Drug", S["hdr"]),
Paragraph("Category", S["hdr"]),
Paragraph("Stock / Ampoule", S["hdr"]),
Paragraph("Standard Dilution", S["hdr"]),
Paragraph("Usual Dose Range", S["hdr"]),
Paragraph("Working Conc.", S["hdr"]),
Paragraph("Example ml/hr (70 kg)", S["hdr"]),
Paragraph("Key Nursing Notes", S["hdr"]),
]
drug_rows = [drug_hdr]
CATS = {
"Vasopressor": (LRED, RED),
"Vasopressor/Inotrope": (LRED, RED),
"Inotrope": (LRED, RED),
"Antiarrhythmic": (LPURP, PURPLE),
"Anticoagulant": (LORANGE, ORANGE),
"Opioid Analgesic": (LTEAL, TEAL),
"Benzodiazepine Sedative": (LTEAL, TEAL),
"IV Anaesthetic/Sedative": (LTEAL, TEAL),
"Vasodilator": (LBLUE, DKBLUE),
"Alpha/Beta-Blocker": (LBLUE, DKBLUE),
"Electrolyte": (LGREEN, GREEN),
"Hormone": (LGREEN, GREEN),
"Uterotonic": (LYELLOW, GOLD),
}
for row in drug_data_raw:
drug, cat, stock, dilution, dose, conc, example, notes = row
drug_rows.append([
Paragraph(drug, S["bold"]),
Paragraph(cat, S["body"]),
Paragraph(stock, S["body"]),
Paragraph(dilution, S["formulac"]),
Paragraph(dose, S["body"]),
Paragraph(conc, S["boldc"]),
Paragraph(example, S["formulac"]),
Paragraph(notes, S["note"]),
])
total_w = W - 1.6*cm
d_col_w = [
total_w * 0.095, # Drug
total_w * 0.075, # Category
total_w * 0.100, # Stock
total_w * 0.115, # Dilution
total_w * 0.095, # Dose range
total_w * 0.085, # Concentration
total_w * 0.145, # Example ml/hr
total_w * 0.290, # Notes
]
drug_table = Table(drug_rows, colWidths=d_col_w, repeatRows=1)
# Build alternating row colors based on category
row_styles = [
("BACKGROUND", (0,0), (-1,0), RED),
("LINEBELOW", (0,0), (-1,0), 1, NAVY),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING", (0,0), (-1,-1), 2),
("LEFTPADDING", (0,0), (-1,-1), 3),
("RIGHTPADDING", (0,0), (-1,-1), 3),
]
prev_cat = None
for i, row in enumerate(drug_data_raw):
cat = row[1]
light_color, dark_color = CATS.get(cat, (LGREY, NAVY))
row_idx = i + 1 # 0 is header
row_styles.append(("BACKGROUND", (0, row_idx), (-1, row_idx), light_color))
# Thicker border when category changes
if cat != prev_cat and i > 0:
row_styles.append(("LINEABOVE", (0, row_idx), (-1, row_idx), 1.2, dark_color))
prev_cat = cat
drug_table.setStyle(TableStyle(row_styles))
story.append(drug_table)
def page3_worked(story):
"""Worked examples and common pitfalls."""
story.append(PageBreak())
# ── SECTION 5: Worked Examples ────────────────────────────────────────
story.append(banner("SECTION 5 — WORKED EXAMPLES (Step-by-Step)", GREEN))
story.append(Spacer(1, 2*mm))
EX_W = (W - 1.6*cm) / 3 - 2*mm
examples = [
{
"title": "Example 1 — Weight-Based (mcg/kg/min)",
"bg": LTEAL, "border": TEAL,
"steps": [
("Given", "Drug: Dobutamine\nStock: 250 mg/5 ml\nWeight: 80 kg\nDose: 5 mcg/kg/min"),
("Step 1: Concentration",
"250 mg / 5 ml = 50 mg/ml\n50 mg/ml x 1000 = 50,000 mcg/ml"),
("Step 2: Dose required/min",
"5 mcg/kg/min x 80 kg\n= 400 mcg/min"),
("Step 3: Dose/hr",
"400 mcg/min x 60 min\n= 24,000 mcg/hr"),
("Step 4: ml/hr",
"24,000 mcg/hr / 50,000 mcg/ml\n= 0.48 ml/hr"),
("Answer", "0.48 ml/hr\n(Consider diluting for practicality)"),
]
},
{
"title": "Example 2 — Non-Weight-Based (mcg/min)",
"bg": LBLUE, "border": DKBLUE,
"steps": [
("Given", "Drug: GTN\nDilution: 50 mg in 500 ml\nDose: 60 mcg/min"),
("Step 1: Concentration",
"50 mg / 500 ml = 0.1 mg/ml\n0.1 x 1000 = 100 mcg/ml"),
("Step 2: Dose/hr",
"60 mcg/min x 60 min\n= 3,600 mcg/hr"),
("Step 3: ml/hr",
"3,600 mcg/hr / 100 mcg/ml\n= 36 ml/hr"),
("Answer", "36 ml/hr"),
("Check", "36 ml/hr x 100 mcg/ml / 60\n= 60 mcg/min CORRECT"),
]
},
{
"title": "Example 3 — Units/hr (Heparin)",
"bg": LORANGE, "border": ORANGE,
"steps": [
("Given", "Drug: Heparin\nDilution: 25,000 u in 50 ml\nDose: 1,500 units/hr"),
("Step 1: Concentration",
"25,000 units / 50 ml\n= 500 units/ml"),
("Step 2: ml/hr",
"1,500 units/hr / 500 units/ml\n= 3 ml/hr"),
("Answer", "3 ml/hr"),
("Reverse check",
"3 ml/hr x 500 units/ml\n= 1,500 units/hr CORRECT"),
("Note", "Always reconcile with APTT\nresult per protocol"),
]
},
]
col_tables = []
for ex in examples:
rows = [[Paragraph(ex["title"],
ParagraphStyle("et", fontName="Helvetica-Bold",
fontSize=7.5, textColor=WHITE,
alignment=TA_CENTER))]]
rows_data = []
for label, content in ex["steps"]:
is_answer = label in ("Answer", "Check", "Reverse check")
rows_data.append([
Paragraph(label, S["bold"]),
Paragraph(content, S["formulac"] if "Step" in label or is_answer
else S["body"]),
])
step_table = Table(rows_data, colWidths=[EX_W*0.32, EX_W*0.68])
step_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), ex["bg"]),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
# Highlight answer rows
("BACKGROUND", (0, len(rows_data)-2), (-1, len(rows_data)-2),
HexColor("#D5F5E3")),
]))
title_t = Table(
[[Paragraph(ex["title"], ParagraphStyle(
"et", fontName="Helvetica-Bold", fontSize=7.5,
textColor=WHITE, alignment=TA_CENTER))]],
colWidths=[EX_W],
style=TableStyle([
("BACKGROUND", (0,0),(-1,-1), ex["border"]),
("TOPPADDING", (0,0),(-1,-1), 4),
("BOTTOMPADDING", (0,0),(-1,-1), 4),
])
)
col_tables.append([title_t, Spacer(1, 1*mm), step_table])
# Three-column layout
three_col = Table(
[[col_tables[0][0], col_tables[1][0], col_tables[2][0]],
[Spacer(1, 1*mm), Spacer(1, 1*mm), Spacer(1, 1*mm)],
[col_tables[0][2], col_tables[1][2], col_tables[2][2]]],
colWidths=[EX_W + 2*mm, EX_W + 2*mm, EX_W + 2*mm],
style=TableStyle([
("VALIGN", (0,0),(-1,-1), "TOP"),
("LEFTPADDING", (0,0),(-1,-1), 0),
("RIGHTPADDING", (0,0),(-1,-1), 3*mm),
("TOPPADDING", (0,0),(-1,-1), 0),
("BOTTOMPADDING",(0,0),(-1,-1), 0),
])
)
story.append(three_col)
story.append(Spacer(1, 3*mm))
# ── SECTION 6: Common Pitfalls ────────────────────────────────────────
story.append(banner("SECTION 6 — COMMON CALCULATION ERRORS & SAFETY TIPS", MAROON))
story.append(Spacer(1, 2*mm))
pitfalls = [
("1", "Unit mismatch",
"Mixing mg and mcg without converting. Always convert to a single unit before calculating.",
RED),
("2", "Forgetting the x 60",
"Dose is in mcg/min but formula needs mcg/hr. Always multiply by 60 for time conversion.",
RED),
("3", "Using total ampoule volume, not mg",
"Stock says '5 mg/5 ml'. Concentration = 1 mg/ml, NOT 5 mg/ml. Divide dose by volume.",
RED),
("4", "Not rechecking concentration after dilution",
"If you add 250 mg to a 50 ml bag you already had 45 ml in, final volume is 50 ml — double check.",
ORANGE),
("5", "Running weight-based drugs without weight",
"Always confirm actual body weight (not estimated). For obese patients, clarify if ABW or IBW.",
ORANGE),
("6", "KCl undiluted IV push",
"FATAL. Potassium chloride must ALWAYS be diluted. Never bolus undiluted KCl.",
RED),
("7", "Forgetting pump minimum rate",
"Most pumps cannot reliably deliver <0.1 ml/hr. If calculated rate is below this, dilute further.",
ORANGE),
("8", "Not doing a reverse check",
"After calculating ml/hr, work backwards: ml/hr x conc / 60 / weight = should equal original dose.",
GREEN),
]
pitfall_hdr = [
Paragraph("#", S["hdr"]),
Paragraph("Error Type", S["hdr"]),
Paragraph("What Goes Wrong & How to Avoid It", S["hdr"]),
]
pitfall_rows = [pitfall_hdr]
for num, etype, desc, col in pitfalls:
sty = ParagraphStyle("ps", fontName="Helvetica-Bold", fontSize=7,
textColor=col, leading=9.5)
pitfall_rows.append([
Paragraph(num, S["boldc"]),
Paragraph(etype, sty),
Paragraph(desc, S["body"]),
])
total_w = W - 1.6*cm
p_table = Table(pitfall_rows,
colWidths=[total_w*0.04, total_w*0.18, total_w*0.78])
p_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), MAROON),
("ROWBACKGROUNDS",(0,1), (-1,-1), (WHITE, LRED)),
("GRID", (0,0), (-1,-1), 0.4, HexColor("#BFC9CA")),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("LINEBELOW", (0,0), (-1,0), 1, NAVY),
]))
story.append(p_table)
story.append(Spacer(1, 2*mm))
# ── REVERSE CHECK FORMULA ─────────────────────────────────────────────
rev_table = Table(
[[Paragraph(
"REVERSE CHECK (always verify your answer): "
"Dose = ml/hr x Concentration (mcg/ml) / 60 / Weight (kg) = should equal prescribed dose",
ParagraphStyle("rc", fontName="Courier-Bold", fontSize=8,
textColor=NAVY, alignment=TA_CENTER)
)]],
colWidths=[W - 1.6*cm],
style=TableStyle([
("BACKGROUND", (0,0),(-1,-1), LYELLOW),
("TOPPADDING", (0,0),(-1,-1), 5),
("BOTTOMPADDING", (0,0),(-1,-1), 5),
("BOX", (0,0),(-1,-1), 1.2, GOLD),
])
)
story.append(rev_table)
story.append(Spacer(1, 1.5*mm))
# Footer
story.append(HRFlowable(width=W-1.6*cm, thickness=0.5, color=colors.grey))
story.append(Spacer(1, 1*mm))
story.append(Paragraph(
"For educational purposes only. Not a substitute for clinical judgment, "
"institutional protocols, or pharmacist advice. "
"Doses and concentrations may vary by institution — always verify locally.",
S["footer"]))
# ── MAIN ─────────────────────────────────────────────────────────────────────
def main():
out = "/home/daytona/workspace/iv-infusion-ref/IV_Infusion_Reference.pdf"
doc = SimpleDocTemplate(
out,
pagesize=landscape(A4),
leftMargin=0.8*cm,
rightMargin=0.8*cm,
topMargin=0.8*cm,
bottomMargin=1.1*cm,
title="IV Infusion Calculations Reference",
author="Orris Medical Education",
subject="IV Drug Infusion Calculations",
)
story = []
page1_formulas(story)
page2_drugs(story)
page3_worked(story)
doc.build(story, onFirstPage=page_deco, onLaterPages=page_deco)
print(f"Done: {out}")
if __name__ == "__main__":
main()
cd /home/daytona/workspace/iv-infusion-ref && python3 generate_iv_reference.py 2>&1
ls -lh /home/daytona/workspace/iv-infusion-ref/IV_Infusion_Reference.pdf
IV Infusion Reference
PDF Document · PDF
Page 1 - Formulas & Conversions
- 8 Master Formulas in two color-coded columns (teal + dark blue): ml/hr from mcg/kg/min, mcg/min, mg/hr, units/hr, concentration, reverse-check, drop rate, and infusion time
- Unit Conversions table - double-sided: weight conversions (mg/mcg/g/ng) on one side, time and rate conversions on the other (mcg/min → hr, % solutions → mg/ml, etc.)
- Gravity Drip Rate lookup table - drop rates (drops/min) for 6 volumes (50-1000 ml) across 6 time periods, color-coded red (>60 drops/min, hard to count) and green (≤30 drops/min, easy)
Page 2 - Drug Reference Table (18 drugs)
- Vasopressors/Inotropes (red): Noradrenaline, Adrenaline, Dopamine, Dobutamine, Vasopressin
- Antiarrhythmics (purple): Amiodarone, Lignocaine
- Anticoagulants (orange): Unfractionated Heparin
- Sedation/Analgesia (teal): Morphine, Fentanyl, Midazolam, Propofol
- Vasodilators (blue): GTN, Labetalol
- Electrolytes/Others (green): KCl, Insulin, Magnesium Sulphate, Oxytocin
Page 3 - Worked Examples & Safety
- 3 side-by-side worked examples: weight-based (dobutamine), non-weight-based (GTN), and units/hr (heparin) - all with full step-by-step
- 8 Common Calculation Errors with explanations (KCl undiluted bolus highlighted as FATAL)
- Reverse-check formula banner for verifying any answer
What will be your best recommendations for NCLEX study
NCLEX study recommendations 2025 Next Generation NCLEX passing strategies
Best NCLEX Study Recommendations (2025-2026)
First, Understand What NCLEX Tests
1. Understand the NGN Format First
| Item Type | What It Tests | Notes |
|---|---|---|
| Multiple choice (single answer) | Core knowledge | Still the most common |
| Select All That Apply (SATA) | Recognizing multiple correct facts | Better to underselect than guess |
| Extended drag-and-drop | Prioritization, ordering | Read all options first |
| Matrix/Grid questions | Multiple decisions in one scenario | Very common in NGN |
| Bow-tie items | Linking conditions > actions > outcomes | Requires full clinical reasoning |
| Cloze/drop-down | Fill-in-the-blank from a dropdown | Tests precision |
| Extended case studies (6-item sets) | Unfolding patient scenarios | Unique to NGN - very high yield |
2. Master the 4 Clinical Judgment Frameworks
A. Maslow's Hierarchy (for single-patient prioritization)
- Airway/Breathing/Circulation always beats pain, anxiety, or education
B. ABCs (Airway, Breathing, Circulation)
C. Assess Before Act
"The patient is anxious" → assess first "The patient is apneic" → act now
D. Maslow vs Safety Conflict
3. The Right Study Plan Structure
Phase 1 - Content Foundation (Weeks 1-3)
- Fundamentals - most tested across all categories
- Pharmacology - medications appear in nearly every question
- Med-Surg - cardiovascular, respiratory, neuro, renal
- Mental Health - therapeutic communication, crisis, medications
- OB/Maternal - fetal heart monitoring, postpartum complications
- Pediatrics - growth/development, age-specific vitals
Phase 2 - Question Practice (Weeks 3-6)
- Do minimum 75-100 questions per day
- Target 70% accuracy before scheduling your exam
- Read every rationale - even for questions you got right. Understanding why matters more than the answer.
Phase 3 - Full CAT Simulations (Final 2 weeks)
- Do 2-3 full-length timed CAT (Computer Adaptive Test) simulations
- Identify your weak categories from analytics
- Final week: targeted review of weak areas only - do not re-study everything
4. Best Study Resources (Ranked by Evidence & Community Consensus)
Question Banks (Most Important)
| Resource | Questions | Best For |
|---|---|---|
| UWorld | 5,000+ (750+ NGN) | Top-rated rationales, harder than real NCLEX = good prep |
| NCSBN Learning Extension | Official source | Most authentic NGN question format |
| Kaplan QBank | 3,800+ | Decision tree strategy, strong elimination practice |
| BoardVitals | 3,000+ | Good for NGN-specific item types |
| SimpleNursing | 1,200+ | Best for visual/auditory learners |
Video Resources
- Mark Klimek (free on YouTube) - legendary for pharmacology, prioritization, and acid-base. Must-watch.
- Dr Sharon NCLEX (YouTube) - 3 playlists: prioritization, fundamentals, and the "Bluebook." Highly recommended by the NCLEX community.
- Simple Nursing (Nurse Mike) - animated, easy to retain for visual learners
Books
- Saunders Comprehensive Review (Silvestri) - best single reference book, aligns to NCLEX client needs categories
- Prioritization, Delegation and Assignment (LaCharity) - best book specifically for NGN clinical judgment questions
- NCSBN NGN Quick Reference Guide - free PDF from the official source
5. Test-Taking Strategies That Actually Work
The "Worst Consequence" Rule
The "Unexpected Finding" Rule
Eliminate First, Then Choose
- Cross out clearly wrong answers first (reduces to 2 options in most cases)
- Between 2 remaining: pick the one more specific to this patient, not general
SATA Strategy
- Better to get 2/4 correct than guess on all 4 and get 0
Delegation Rules (high-yield for NCLEX)
| Delegate to RN | Delegate to LPN/LVN | Delegate to CNA/PCT |
|---|---|---|
| Initial assessment | Stable, chronic conditions | ADLs (bathing, feeding) |
| Teaching | Routine medications (oral) | Vital signs (stable patients) |
| Unstable patients | Wound care (routine) | Ambulation (stable patients) |
| IV push medications | Catheter insertion | Collecting specimens |
| Care plan changes | NG tube care | Repositioning |
6. High-Yield Content You Cannot Skip
| Topic | Why High-Yield |
|---|---|
| Acid-base imbalances | Appears in respiratory, renal, OB, and pharmacology questions |
| Fluid & electrolytes | Hypo/hyperkalemia, sodium, calcium - tied to ECG changes |
| Sepsis & SIRS | Priority interventions, sepsis bundle |
| Therapeutic communication | Mental health + every single patient interaction question |
| Infection control | Isolation precautions, PPE selection - tested constantly |
| Lab values | Critical highs/lows you must act on immediately |
| Medication safety | 5 rights, high-alert meds (insulin, heparin, digoxin, warfarin) |
| Post-op complications | Hemorrhage, atelectasis, DVT, paralytic ileus |
| Prioritization frameworks | Every question is a prioritization question |
7. Critical Lab Values to Memorize
| Lab | Critical Low | Critical High | Action |
|---|---|---|---|
| K+ (Potassium) | <3.0 mEq/L | >6.0 mEq/L | ECG changes - notify immediately |
| Na+ (Sodium) | <120 mEq/L | >160 mEq/L | Seizure risk |
| Glucose | <50 mg/dL | >500 mg/dL | Hypoglycemia protocol / DKA |
| Hgb | <7 g/dL | - | Transfusion threshold |
| INR | - | >3.5 (non-therapeutic) | Bleeding risk |
| Digoxin | - | >2 ng/ml | Toxicity - hold dose |
| Lithium | - | >1.5 mEq/L | Toxicity - hold dose |
| pH (blood) | <7.35 | >7.45 | Acidosis / Alkalosis |
| O2 Sat | <90% | - | Supplemental O2 immediately |
8. Study Schedule Template (8-Week Plan)
| Week | Focus | Daily Goal |
|---|---|---|
| 1 | Fundamentals + Infection Control | 50 Q + 2 hrs content |
| 2 | Pharmacology (high-alert meds) | 75 Q + 2 hrs content |
| 3 | Cardio-Respiratory Med-Surg | 75 Q + 2 hrs content |
| 4 | Neuro, Renal, Endocrine | 75 Q + 1.5 hrs content |
| 5 | OB/Maternal + Pediatrics | 100 Q + 1.5 hrs content |
| 6 | Mental Health + Delegation | 100 Q + NGN practice |
| 7 | Full CAT simulations x2 | 150 Q timed simulations |
| 8 | Weak areas only + Rest | 75 Q targeted review |
9. The Day Before & Exam Day
- Do not study the day before - light review at most. Your brain needs consolidation time.
- Sleep 7-8 hours - sleep is when memory consolidates.
- Eat a full breakfast with protein.
- Arrive early - know your testing center route in advance.
- During the exam: if a question feels impossible, use your frameworks (ABC, Maslow, safety) rather than guessing blindly.
- Don't count questions - the CAT stops anywhere from 85 to 145 questions for NCLEX-RN. More questions does not mean you are failing.
10. Mindset: The One Thing That Separates Passers
"This is a safety exam. Think like a nurse, not a student."
Find all the available mnemonics for NCLEX prep
NCLEX nursing mnemonics complete list 2025 clinical judgment prioritization
https://goodnurse.com/article/189/the-best-nursing-mnemonics…
nursing mnemonics pharmacology electrolytes acid base mental health NCLEX complete
NCLEX Nursing Mnemonics - The Complete Master Reference
Over 100 mnemonics organized by category. Bookmark this page.
CATEGORY 1 - NURSING PROCESS & CLINICAL FRAMEWORKS
ADPIE - The Nursing Process
Assessment → Diagnosis → Planning → Implementation → Evaluation
ABCs - Physiological Priority Order
Airway → Breathing → Circulation
MASLOW - Hierarchy for Prioritization
Meals (physiological) → Safety → Affection (love/belonging) → Looks (esteem) → Own potential (self-actualization) → Winning (reaching full potential)
SBAR - Communication Framework
Situation → Background → Assessment → Recommendation
SAMPLE - Patient History Taking
Signs & symptoms → Allergies → Medications → Past medical history → Last meal → Events leading to this visit
OLDCARTS - Pain/Symptom Assessment
Onset → Location → Duration → Character → Aggravating factors → Relieving factors → Timing → Severity
PQRST - Pain Assessment (Alternative)
Provocative/Palliative → Quality → Radiation → Severity → Timing
PIE - Nursing Documentation
Problem → Intervention → Evaluation
CATEGORY 2 - PRIORITIZATION & DELEGATION
CURE - What RNs Cannot Delegate
Complex assessments → Unstable patients → Reaching diagnoses → Education (initial)
D-A-N-C-E - Delegation Rules
Do not delegate initial assessments Avoid delegating unstable patients No invasive procedures to CNAs Check the 5 rights of delegation Evaluate after delegating
5 Rights of Delegation
Right task → Right circumstance → Right person → Right direction/communication → Right supervision
CAN DO - What CNAs Can Do
Clean dressings (non-sterile, routine) → Ambulation (stable patients) → Normal vital signs (stable) → Dressing assistance (ADLs) → Oral hygiene, feeding (non-tube)
CATEGORY 3 - PHARMACOLOGY
Drug Class Name Endings (Suffix Mnemonics)
| Suffix | Drug Class | Memory Hook |
|---|---|---|
| -pril | ACE inhibitors | "APRIL cough" - causes dry cough + hyperkalemia |
| -sartan | ARBs | "S-ARTAN skips the cough" - same as ACE but no cough |
| -lol | Beta-blockers | "LOL slows the heart" - bradycardia, low BP |
| -dipine | Calcium channel blockers | "DIP in the heart rate" |
| -statin | Statins | "STATIN Saves The Arteries" - monitor for myopathy |
| -prazole | Proton pump inhibitors | "PRAZOLE for the acid hole" - GERD/ulcers |
| -floxacin | Fluoroquinolones | "FLOX flops tendons" - tendon rupture risk |
| -azole | Antifungals | "AZOLE for the fungus hole" - monitor liver enzymes |
| -mycin/-micin | Aminoglycosides | "My-TOXIN" - nephrotoxic + ototoxic |
| -cillin | Penicillins | Check allergy - cross-reactive with cephalosporins |
| -olol | Beta-blockers | Same as -lol |
| -thiazide | Thiazide diuretics | "THIAZIDE Thirsty" - monitor potassium (wastes K+) |
| -pine | Calcium channel blockers | Peripheral edema side effect |
| -gliptin | DPP-4 inhibitors | Diabetes - pancreatitis risk |
| -mab | Monoclonal antibodies | Biologic agents - infection risk |
| -kinase | Thrombolytics | "Break the CLOT" - bleeding risk |
MONA - Acute MI Management
Morphine → Oxygen → Nitroglycerine → Aspirin
LEAN - Emergency Medications
Lidocaine → Epinephrine → Atropine → Naloxone
IDEA - Bradycardia Treatment
IV access → Drug (Atropine) → External pacing → Advanced interventions (permanent pacemaker)
MADD DOG - Pulmonary Edema Treatment
Morphine → AminoPhylline → Diuretics → Digoxin → Oxygen → Gases (ABG monitoring)
The 3 "Dig" Signs - Digoxin Toxicity
Digoxin toxicity = Diaphoresis, IGG (nausea/vomiting), Green-yellow halos in vision
HIGH ALERT Medications - "PINCH"
Potassium chloride → Insulin → Narcotic opioids → Chemotherapy → Heparin
Anticoagulant Antidotes
"Heparin Hates Protamine" - Heparin antidote = Protamine sulfate "Warfarin Wants Vitamin K" - Warfarin antidote = Vitamin K (+ FFP for urgent reversal) "Dabigatran Demands Idarucizumab" - Dabigatran antidote = Idarucizumab
Insulin Types - "RIANT" Onset Order (Fastest to Slowest)
Rapid-acting (Lispro/Aspart) → Intermediate (NPH) → A... → N... → Time (Glargine = no peak)
Lithium Toxicity - "FINE ARTS"
Facial twitching → Incoordination → Nausea/vomiting → Encephalopathy → Ataxia → Reflex changes → Tremors → Seizures
Warfarin Food Interactions - "KALE"
Foods high in K-vitamin = Avoid consistency changes Leafy greens, Evening primrose are high in Vitamin K - avoid drastic changes
CATEGORY 4 - ELECTROLYTES & FLUID BALANCE
PISO - Where Electrolytes Live
Potassium Inside → Sodium Outside (the cell)
MURDER - Signs of HYPERkalemia (High K+)
Muscle weakness → Urine (oliguria/anuria) → Respiratory distress → Decreased cardiac contractility → ECG changes (peaked T waves → wide QRS → sine wave) → Reflexes decreased
A SIC WALT - Signs of HYPOkalemia (Low K+)
Alkalosis → Skeletal muscle weakness → Ileus (decreased bowel sounds) → Constipation → Weak pulse → Arrhythmias → Lethargy → Thready pulse
6 L's of HYPOkalemia
Lethargy → Leg cramps → Lax muscles (weakness) → Low, shallow respirations → Loss of bowel sounds → Lots of U-waves on ECG
FRIED SALT - Signs of HYPERnatremia (High Na+)
Fever → Restlessness → Increased fluid retention → Edema → Decreased urination → Skin flushed → Agitation → Low-grade fever → Thirst (intense)
SALT LOSS - Signs of HYPOnatremia (Low Na+)
Seizures → Anorexia → Lethargy → Thyroid issues (rule out) → Low Na+ → Overload of free water → Stupor/confusion → Sodium replacement needed
BACK ME - Signs of HYPERcalcemia (High Ca2+)
Bone pain → Anorexia → Constipation → Kidney stones → Muscle weakness → ECG changes (short QT)
CATS - Signs of HYPOcalcemia (Low Ca2+)
Convulsions → Arrhythmias → Tetany → Spasms (Chvostek's & Trousseau's signs)
MAG Is Just LOW - HYPERmagnesemia Effects
Muscle weakness → Arrhythmias → GI symptoms → Is → Just → Loss of reflexes (early warning) → Obtunded → Weakness/respiratory arrest
TWITCHES & TORSADES - HYPOmagnesemia
Twitching → Torsades de pointes (fatal arrhythmia)
RIFLE - Acute Kidney Injury Staging
Risk → Injury → Failure → Loss (>4 weeks) → End-stage renal disease
WEIGHS - Dialysis Assessment
Weight (daily) → Electrolytes → Intake & output → Grafts/fistula check → Hypotension risk → Symptoms of fluid overload
CATEGORY 5 - ACID-BASE BALANCE
ROME - Interpreting ABGs
Respiratory Opposite → Metabolic Equal
- Respiratory disorders: pH and PaCO2 move in OPPOSITE directions
- Metabolic disorders: pH and HCO3 move in the SAME direction
TICS - Metabolic Acidosis Causes
Toxins (aspirin, methanol, ethanol overdose) → Insulin lack (DKA) → Chronic kidney disease → Shock (lactic acidosis)
MUDPILES - Anion Gap Metabolic Acidosis
Methanol → Uremia → DKA → Propylene glycol → Infection/sepsis → Lactic acidosis → Ethylene glycol → Salicylates
DARE - Respiratory Acidosis Causes
Drugs (opioids, sedatives) → Airway obstruction → Respiratory muscle failure → Emphysema/COPD
LOBE - Respiratory Alkalosis Causes
Liver failure → Oxygen (hypoxia compensation) → Brain injury → Emotional (anxiety, hyperventilation)
CATEGORY 6 - CARDIOVASCULAR & RESPIRATORY
CHEST PAIN - Cardiac Assessment
Character → History → ECG changes → ST changes → Time of onset → Precipitating factors → Associated symptoms → Intensity (0-10) → Nitro response
FAST - Stroke Recognition
Facial drooping → Arm weakness → Speech difficulty → Time to call emergency
Balance → Eyes (vision changes) → Face → Arm → Speech → Time
PLEASE READ HIS TEXT - Cor Pulmonale Signs
Pitting edema → Right ventricle hypertrophy → Elevated JVP → Ascites → Signs of hypoxia → Exertional dyspnea → Respiratory changes → Edema (peripheral) → Ankle swelling → Distended neck veins → Hepatomegaly → Increased CVP → Split S2 → Tachycardia → Exercise intolerance → Xertional fatigue
3 Ps of Diabetes (Hyperglycemia) - HYPERglycemia
Polyuria → Polydipsia → Polyphagia
"Hot and Dry = Sugar High, Cold and Clammy = Need Some Candy"
- Hyperglycemia: Hot, dry, flushed skin (dehydrated)
- Hypoglycemia: Cool, clammy, diaphoretic (adrenergic response)
WILLIAM MARROW - Bundle Branch Blocks (ECG)
WiLLiaM = LBBB: W pattern in V1, M pattern in V6 MaRRoW = RBBB: M pattern in V1, W pattern in V6
VEAL CHOP - Fetal Heart Rate Monitoring
Variable decelerations = Cord compression Early decelerations = Head compression Accelerations = OK (good sign) Late decelerations = Placental insufficiency (EMERGENCY - turn patient, O2, call MD)
CATEGORY 7 - MUSCULOSKELETAL & NEURO
5 Ps of Compartment Syndrome
Pain (severe, out of proportion) → Pallor → Pulselessness → Parasthesia → Paralysis
Extra: 6th P = Pressure (palpable tenseness over the compartment)
PRICE/PRICEM - Musculoskeletal Injury Treatment
Protection → Rest → Ice → Compression → Elevation → Medication (analgesics)
GLASCOW - Neuro Assessment Components
Eye opening (1-4) + Verbal response (1-5) + Motor response (1-6) = Total 3-15
AEIOU TIPS - Causes of Altered Mental Status
Alcohol/Drugs → Epilepsy (post-ictal) → Infection (meningitis, sepsis) → Overdose → Uremia (renal failure) → Trauma → Insulin (hypo/hyperglycemia) → Psychiatric → Stroke/Structural
PERRLA - Eye Assessment
Pupils Equal Round Reactive to Light and Accommodation
CNOT - Cranial Nerves by Number (alternative to long lists)
"On Old Olympus Towering Tops A Finn And German Viewed Some Hops" Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Acoustic (Vestibulocochlear), Glossopharyngeal, Vagus, Spinal accessory, Hypoglossal
CATEGORY 8 - GI & HEPATIC
FFFFF - Gallstone Risk Factors (Cholelithiasis)
Female → Fat → Forty → Fertile → Fair-skinned (or Family history)
BRAT Diet - Post-GI illness
Bananas → Rice → Applesauce → Toast
CRAP - Crohn's Disease Features
Cobblestone appearance → Right lower quadrant pain → All layers of bowel affected (transmural) → Perianal fistulas/skip lesions
PUSH - Ulcerative Colitis Features
Pseudopolyps → Ulcers → Superficial mucosa only → Hemorrhage/bloody diarrhea
CATEGORY 9 - MATERNITY & OB
BUBBLE - Postpartum Assessment
Breasts → Uterus → Bowel → Bladder → Lochia → Episiotomy/incision/extremities
HELLP - Severe Preeclampsia Complication
Hemolysis → Elevated Liver enzymes → Low Platelets
TORCH - Congenital Infections
Toxoplasmosis → Other (syphilis, HIV, Zika, parvovirus) → Rubella → Cytomegalovirus (CMV) → Herpes simplex
TRAMP - Postpartum Hemorrhage Causes
Tone (uterine atony - #1 cause) → Retained tissue (placenta) → Atonic uterus → Maternal coagulopathy → Placenta previa/accreta
APGAR - Newborn Assessment (at 1 and 5 minutes)
Appearance (color) → Pulse (heart rate) → Grimace (reflex irritability) → Activity (muscle tone) → Respiration
COAT - OB Complications Requiring Immediate Action
Cord prolapse → Obstructed labor → Abruption (placental) → Transverse lie
CATEGORY 10 - PEDIATRICS
FACES/FLACC - Pediatric Pain Assessment
Face → Legs → Activity → Cry → Consolability (scored 0-2 each, total 0-10)
BLOCK 6 at 2 - Developmental Milestone
Child can stack a tower of 6 blocks by age 2 years
- 3-4 months: social smile
- 6 months: sits with support
- 9 months: pincer grasp
- 12 months: walks, says "mama/dada"
- 18 months: 10-word vocabulary
- 2 years: 2-word phrases, runs
SAVE A CHILD - Pediatric Emergency Priorities
Size (use weight-based dosing) → Airway (proportionally larger head = sniffing position) → Vein access → Epiglottis (larger, floppy) → Anxiety management → Cold (hypothermia risk) → Heart rate is key (not BP) → Infection (immature immunity) → Liver (immature metabolism) → Development (use age-appropriate communication)
CATEGORY 11 - MENTAL HEALTH & PSYCHIATRIC NURSING
DIG FAST - Signs of Mania (Bipolar I)
Distractibility → Impulsivity → Grandiosity → Flight of ideas → Activity increased → Sleep decreased → Talkativeness (pressured speech)
SAD PERSONS - Suicide Risk Assessment
Sex (male higher completion risk) → Age (elderly + adolescent) → Depression → Previous attempt (#1 predictor) → Ethanol/substance use → Rational thinking loss → Social support lacking → Organized plan → No spouse/partner → Sickness (chronic illness)
5 A's of Alzheimer's Disease
Amnesia (memory loss) → Aphasia (language) → Apraxia (motor skills) → Agnosia (recognition) → Attentional deficits (executive function)
BATTED - Risk Factors for Elder Abuse
Bedbound → Alcohol/substance abuse (caregiver) → Threats observed → Trauma signs → External control (isolated) → Dependence (financial/physical)
TRAP - Therapeutic Communication Blocks (What NOT to do)
Threatening → Reassuring falsely → Advising → Probing
HALT - Non-therapeutic communication patterns
Hiding behind routine → Avoiding the patient's problem → Lecturing/moralizing → Telling what they should feel
CATEGORY 12 - INFECTION CONTROL & ISOLATION
MTV - Airborne Precautions
Measles → Tuberculosis (TB) → Varicella (chickenpox)
SPIDERMAN - Droplet Precautions
Scarlet fever → Pertussis (whooping cough) → Influenza → Diphtheria → Epiglottitis → Rubella → Adenovirus → Mumps → Adrenal plague (pneumonic) → Neisseria meningitidis
MRS WEE - Contact Precautions
MRSA → RSV → Skin infections (impetigo, scabies) → Wounds (draining) → Enteric infections (C. diff) → Ebola
DONNING & DOFFING Order
Gown → Mask/respirator → Goggles/face shield → Gloves
Gloves → Goggles → Gown → Mask
CATEGORY 13 - ENDOCRINE & CANCER
3 Ps - Diabetes Hyperglycemia
Polyuria (excess urination) → Polydipsia (excess thirst) → Polyphagia (excess hunger)
DKA vs HHS (Hyperosmolar Hyperglycemic State)
DKA: BOTH Type 1 and Type 2, acidosis, ketones, glucose usually >250 HHS: Type 2 mainly, NO acidosis, NO ketones, glucose >600 (very high)
CAUTION - Cancer Warning Signs
Change in bowel/bladder habits → Asore that doesn't heal → Unusual bleeding/discharge → Thickening/lump in breast or elsewhere → Indigestion or difficulty swallowing → Obvious change in a wart or mole → Nagging cough or hoarseness
FAME - Infective Endocarditis Signs
Fever → Anemia → Murmur (new or changing) → Embolism (Janeway lesions, Osler nodes, splinter hemorrhages)
CATEGORY 14 - RESPIRATORY
4 Ds of Epiglottitis (Pediatric Emergency)
Drooling → Dysphagia → Dysphonia (muffled "hot potato" voice) → Distress (tripod position)
COPD Nursing Tips - "Pink Puffer vs Blue Bloater"
Pink Puffer = Emphysema (barrel chest, pursed-lip breathing, uses accessory muscles, thin) Blue Bloater = Chronic Bronchitis (cyanosis, productive cough, obese, edema)
ASTHMA Attack - "SABA First"
Short-Acting Beta Agonist (albuterol) first in acute attack, then assess response
CATEGORY 15 - MISC / HIGH-YIELD
5 Rights of Medication Administration
Right patient → Right drug → Right dose → Right route → Right time
"Clouds Over Grass, Smoke Over Fire" - ECG Lead Placement
White (clouds) over Green (grass) = White lead above Green lead Black (smoke) over Red (fire) = Black lead above Red lead Brown goes on the stomach (precordial leads)
PRICE - Fracture/Sprain First Aid
Protection → Rest → Ice → Compression → Elevation
THINK - Before Intervening
Therapeutic? → Harmful? → Informed consent? → Nurse competent? → Keep patient safe?
Quick Master Index
| Mnemonic | Topic |
|---|---|
| ABCs | Physiological prioritization |
| ADPIE | Nursing process |
| APGAR | Newborn scoring |
| A SIC WALT | Hypokalemia signs |
| AEIOU TIPS | Altered mental status |
| BACK ME | Hypercalcemia |
| BE-FAST | Stroke recognition |
| BLOCK 6 at 2 | Developmental milestone |
| BUBBLE | Postpartum assessment |
| CAUTION | Cancer warning signs |
| CATS | Hypocalcemia |
| COPD Pink/Blue | Emphysema vs bronchitis |
| DARE | Respiratory acidosis causes |
| DIG FAST | Mania signs |
| DKA vs HHS | Diabetic emergencies |
| DONNING/DOFFING | PPE order |
| FAME | Endocarditis |
| FAST/BE-FAST | Stroke |
| FFFFF | Gallstone risk |
| FRIED SALT | Hypernatremia |
| HELLP | Preeclampsia |
| Hot/Dry - Cold/Clammy | Hyper/hypoglycemia |
| IDEA | Bradycardia treatment |
| LEAN | ET tube emergency meds |
| LOBE | Respiratory alkalosis |
| MADD DOG | Pulmonary edema |
| MAG Is Just LOW | Hypermagnesemia |
| Maslow | Prioritization hierarchy |
| MONA | Acute MI care |
| MRS WEE | Contact precautions |
| MUDPILES | Anion gap acidosis |
| MURDER | Hyperkalemia |
| MTV | Airborne precautions |
| OLDCARTS | Symptom assessment |
| PERRLA | Pupil assessment |
| PINCH | High-alert medications |
| PISO | Electrolyte location |
| PQRST | Pain assessment |
| PRICE | Fracture first aid |
| ROME | ABG interpretation |
| SAD PERSONS | Suicide risk |
| SALT LOSS | Hyponatremia |
| SAMPLE | History taking |
| SBAR | Communication |
| SPIDERMAN | Droplet precautions |
| TICS | Metabolic acidosis causes |
| TORCH | Congenital infections |
| TRAMP | PPH causes |
| TRAP | Bad communication |
| VEAL CHOP | Fetal heart decelerations |
| WILLIAM MARROW | Bundle branch blocks |
| 5 P's | Compartment syndrome |
| 5 Rights | Medication safety |
| 6 L's | Hypokalemia |