Cavernous sinus essential anatomy and cavernous sinus thrombosis emphasizing ophthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"cavernous sinus thrombosis" AND ophthalmology
Searching Images
cavernous sinus anatomy cranial nerves contents
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Searching Images
cavernous sinus thrombosis proptosis chemosis clinical
Loading Image
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks and excellent clinical/anatomical images. Let me compose the comprehensive answer.
Cavernous Sinus: Essential Anatomy & Cavernous Sinus Thrombosis (Ophthalmic Focus)
PART I — ESSENTIAL ANATOMY
Location and Structure
The cavernous sinuses are paired trabeculated dural venous chambers situated at the base of the skull, one on each side of the pituitary fossa, immediately above the midline sphenoid sinus. Each sinus is bounded:
- Medially: by the pituitary fossa / sphenoid bone
- Superiorly: free dural edge with the diaphragma sellae
- Inferiorly: the floor of the middle cranial fossa
- Posteriorly: connects to the petrosal sinuses (superior and inferior)
- Anteriorly: receives the superior ophthalmic vein
The two sinuses communicate across the midline via the intercavernous (circular) sinuses anterior and posterior to the pituitary — a fact of major clinical importance, as infection can cross within 24–48 hours.
— Goldman-Cecil Medicine; Localization in Clinical Neurology, 8e
Intracavernous Contents
| Structure | Position within Sinus |
|---|---|
| Internal carotid artery (ICA) | Runs through the venous blood of the sinus (not just the wall) — S-shaped cavernous segment |
| CN VI (Abducens) | Runs freely within the sinus, medial to CN III/IV — most susceptible to elevated pressure |
| CN III (Oculomotor) | Lateral wall, superior compartment |
| CN IV (Trochlear) | Lateral wall, between CN III and V1 |
| CN V1 (Ophthalmic div.) | Lateral wall, inferior to CN IV |
| CN V2 (Maxillary div.) | Lateral wall, most inferior — exits via foramen rotundum |
| Sympathetic plexus | Runs with the ICA within the sinus |
Key point: CN III, IV, V1, and V2 lie in the lateral dural wall of the sinus. CN VI and the ICA lie within the venous space itself. The mandibular division (V3) does NOT traverse the cavernous sinus — it exits directly via foramen ovale. — Localization in Clinical Neurology, 8e
Cadaveric dissection showing the cavernous sinus contents:
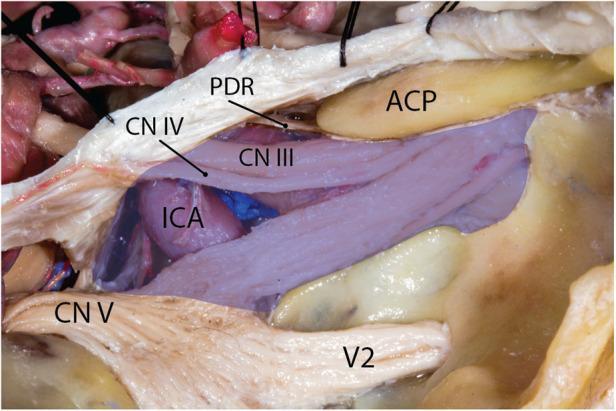
High-magnification cadaveric dissection of the cavernous sinus. Blue overlay = venous space. ICA = internal carotid artery; CN III = oculomotor nerve (superior lateral wall); CN IV = trochlear nerve; CN V and V2 = trigeminal branches; ACP = anterior clinoid process; PDR = proximal dural ring.
Endoscopic transpterygoid view (surgical anatomy):
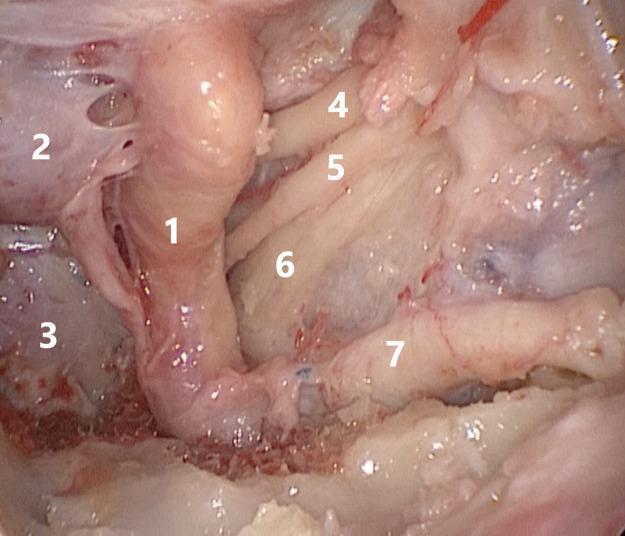
Transnasal transpterygoid endoscopic view. From superior to inferior on the lateral wall: oculomotor (4), abducens (5), V1 (6), V2 (7). The ICA (1) is the central structure.
Venous Drainage (Why CST Spreads the Way It Does)
The cavernous sinus drains:
- Anteriorly: superior and inferior ophthalmic veins (from orbit and face)
- Posteriorly: superior and inferior petrosal sinuses → sigmoid sinus / jugular vein
- Contralaterally: intercavernous sinuses around the pituitary
Inflow comes from the ophthalmic veins, sphenoparietal sinus, middle cerebral vein, and deep sylvian vein. All these tributaries are valveless, permitting retrograde spread of infection from the orbit, face, sinuses, and dentition.
Cavernous Sinus Syndrome (Localization Pearl)
A lesion confined to the cavernous sinus produces:
- Total ipsilateral ophthalmoplegia (CN III, IV, VI)
- Pain/paresthesia in V1 and V2 distribution (forehead, cheek, upper teeth)
- Oculosympathetic paresis (partial Horner — ptosis + miosis, no anhidrosis, since the postganglionic fibers leave with the ICA)
- No V3 involvement (distinguishes cavernous sinus from middle cranial fossa lesion)
- No anhidrosis (sympathetic sudomotor fibers travel with the external carotid, not the ICA)
Laterally placed lesions typically present first with CN VI palsy (medial location in the sinus); lesions expanding from the sella present first with CN III palsy.
— Localization in Clinical Neurology, 8e; Bradley and Daroff's Neurology in Clinical Practice
Cavernous Sinus vs. Superior Orbital Fissure vs. Orbital Apex
| Feature | Cavernous Sinus | Superior Orbital Fissure | Orbital Apex |
|---|---|---|---|
| CN II (optic) | ✗ Spared | ✗ Usually spared | ✓ Involved → blindness |
| CN III, IV, VI | ✓ | ✓ | ✓ |
| V1 | ✓ | ✓ | ✓ |
| V2 | ✓ | ✗ Spared | ✗ Spared |
| Proptosis | Variable | Variable | Variable |
| Oculosympathetics | ✓ (no anhidrosis) | ✓ | ✓ |
These three syndromes are clinically indistinguishable without neuroimaging; V2 involvement points to the cavernous sinus. — Localization in Clinical Neurology, 8e
PART II — CAVERNOUS SINUS THROMBOSIS (CST)
Definition and Epidemiology
CST is thrombosis within the cavernous sinus, most often septic (infectious). It carries a mortality of ~20% even with treatment; up to 100% if untreated. It is one of the few true neuro-ophthalmic emergencies. — Kanski's Clinical Ophthalmology, 10e
Pathogenesis and Sources of Infection
The infection reaches the cavernous sinus via retrograde thrombophlebitis through the valveless ophthalmic and emissary veins:
| Source | Route |
|---|---|
| Paranasal sinusitis (sphenoid, ethmoid most dangerous; frontal) | Direct extension or emissary veins |
| Orbital/periorbital cellulitis | Superior ophthalmic vein → cavernous sinus |
| Dental infection (upper dentition esp.) | Facial/pterygoid plexus → cavernous sinus |
| Skin infections (mid-face "danger triangle") | Angular/facial veins → superior ophthalmic vein |
| Otitis / mastoiditis | Petrosal sinuses |
Most common organism: Staphylococcus aureus (including MRSA). Streptococci, gram-negative bacilli, and anaerobes (in sinusitis) are less common. Mucormycosis and Aspergillus must be considered in diabetics and immunosuppressed patients — these can mimic CST radiologically and clinically. — Adams and Victor's Neurology, 12e; Goldman-Cecil Medicine
Ophthalmic Manifestations — Core of the Clinical Picture
Because the ophthalmic veins drain directly into the cavernous sinus, the eye is the primary window for diagnosing CST.
1. Venous Obstruction Signs (Orbital Congestion)
| Sign | Mechanism |
|---|---|
| Proptosis (exophthalmos) | Obstruction of ophthalmic vein outflow → orbital venous congestion |
| Periorbital/eyelid edema | Same — often extreme, "board-like" firmness |
| Chemosis (conjunctival edema) | Venous congestion of conjunctival vasculature |
| Dilated, tortuous conjunctival/episcleral vessels | Elevated episcleral venous pressure |
| Forehead/facial edema | Extension of venous obstruction |
Clinical photograph — CST presenting with right periorbital edema and ptosis:

2. Cranial Nerve Palsies (Direct Neural Involvement)
CN VI palsy is typically the earliest and most common cranial nerve sign because the abducens nerve runs freely within the venous sinus and has no dural protection:
| Nerve | Deficit |
|---|---|
| CN VI (abducens) | Lateral gaze palsy → horizontal diplopia; the eye is deviated medially |
| CN III (oculomotor) | Ptosis, "down and out" eye, dilated unreactive pupil (pupil involved early in compressive/inflammatory lesions, unlike ischemic CN III palsy) |
| CN IV (trochlear) | Vertical/torsional diplopia (difficult to isolate clinically in context of full ophthalmoplegia) |
| CN V1 | Decreased corneal sensation, forehead hypoesthesia/pain |
| CN V2 | Cheek and upper lip sensory loss |
| Sympathetic | Oculosympathetic paresis: partial ptosis + miosis (without anhidrosis) |
The combination of painful ophthalmoplegia + proptosis + chemosis + fever is essentially pathognomonic for CST until proven otherwise. — Adams and Victor's Neurology, 12e
3. Fundoscopic / Posterior Segment Signs
| Finding | Mechanism |
|---|---|
| Papilledema | Raised intracranial pressure ± direct optic nerve congestion |
| Retinal vein engorgement | Increased venous backpressure |
| Retinal hemorrhages | Venous outflow obstruction |
| Visual loss | Retrobulbar optic neuropathy (ischemia/infarction of retroorbital optic nerve) — often irreversible |
| Central retinal vein occlusion | Elevated episcleral/orbital venous pressure |
Visual loss from retrobulbar optic neuropathy in CST tends to be permanent even after treatment — the cranial nerve palsies generally recover, but vision often does not. — Adams and Victor's Neurology, 12e
4. Bilateralization — The Diagnostic Red Flag
Unlike orbital cellulitis, CST characteristically spreads to the contralateral eye within 24–48 hours via the intercavernous sinuses. Bilateral proptosis and ophthalmoplegia developing over 1–2 days is virtually diagnostic of CST and distinguishes it from unilateral orbital processes. — Adams and Victor's Neurology, 12e; Kanski's Ophthalmology, 10e
Full Clinical Syndrome
Systemic: high spiking fever, rigors, malaise, septicemia, headache (often severe frontal/retro-orbital), photophobia, nausea/vomiting, altered consciousness (in severe cases)
Local: sequential involvement of orbital structures, cranial nerve palsies, and fundus changes as described above
Posterior spread: thrombus extension to petrosal sinuses → CN VI and facial (CN VII) involvement without orbital signs. Extension to meninges → meningitis; to brain parenchyma → septic emboli, cerebral abscess.
MRI and Imaging Composite — CST with Bilateral Involvement:
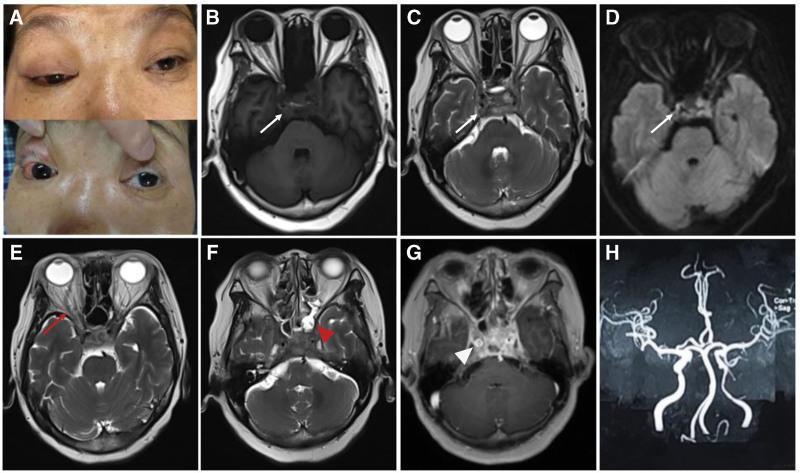
Bilateral CST. A: Bilateral ptosis and right proptosis. B–D: Mixed T1/T2 signal within both cavernous sinuses = thrombus. E: Enlarged superior ophthalmic vein. F: Sphenoid/ethmoid sinusitis (infectious source). G: Cavernous sinus expansion with ring enhancement. H: Left intracavernous ICA stenosis on MRA.
Superior Ophthalmic Vein Thrombosis (SOVT) — The Ophthalmologic Precursor
SOVT often precedes or accompanies CST and presents with the same orbital signs. MRI/CT shows dilatation and non-enhancement of the superior ophthalmic vein — this is a key early imaging sign and should prompt urgent CST workup.
SOVT progressing to CST — before and after treatment:
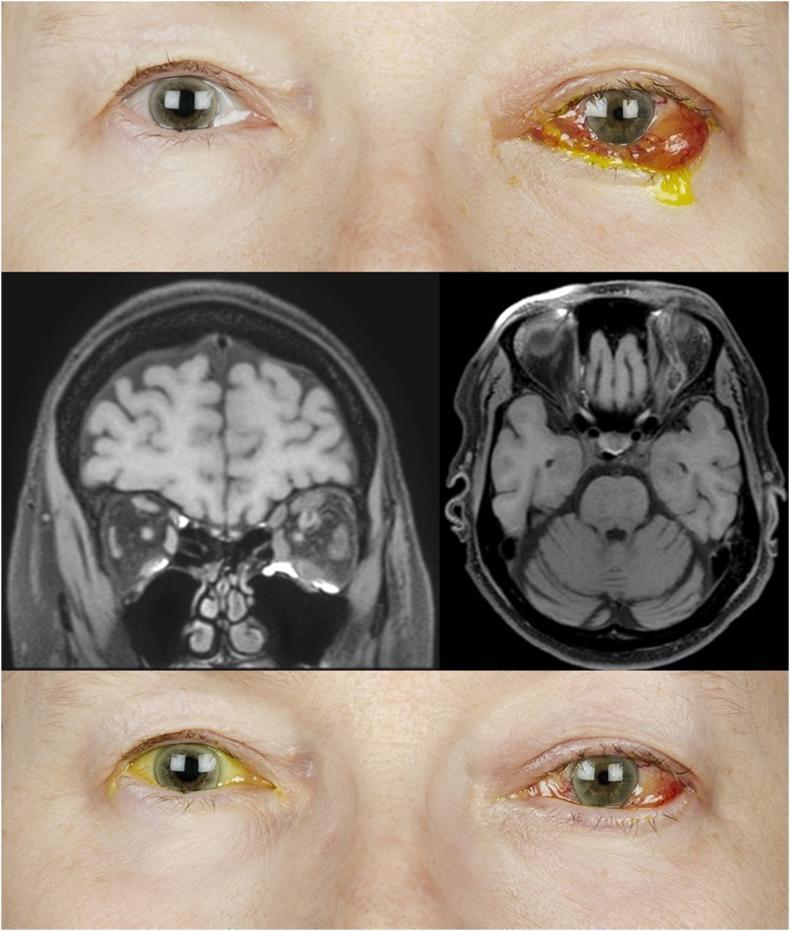
Superior ophthalmic vein thrombosis as harbinger of CST. Left eye: total ptosis, hemorrhagic chemosis, purulent discharge at presentation (top). MRI: enlarged SOV, extraocular muscle swelling (middle). Significant resolution after treatment at 3 weeks (bottom).
Chandler-Hubert Classification (Orbital Spread of Sinus Infection)
CST represents the most severe (Type V) complication in this widely used classification:
| Type | Stage |
|---|---|
| I | Preseptal (periorbital) cellulitis |
| II | Orbital (post-septal) cellulitis |
| III | Subperiosteal abscess |
| IV | Orbital abscess |
| V | Cavernous sinus thrombosis |
— Kanski's Clinical Ophthalmology, 10e
Diagnosis
MRI with gadolinium + MR Venography is the gold standard:
- Loss of normal flow void in the cavernous sinus
- Heterogeneous signal from the sinus (thrombus)
- Hyperintense signal on T1 in thrombosed segments
- Deformity or narrowing of the intracavernous ICA
- Enlarged superior ophthalmic vein (key early sign)
- Sinus opacification (source identification)
CT with contrast is useful when MRI is unavailable (subtle enhancement changes in the sinus, filling defect). MR Angiography demonstrates ICA narrowing/compression. CSF is typically normal unless meningitis or empyema coexists. — Goldman-Cecil Medicine
Blood cultures are positive in ~70% of septic CST cases. CBC, ESR, CRP, and specific sinus cultures guide antibiotic selection.
Differential Diagnosis (Ophthalmologic)
| Condition | Distinguishing Features |
|---|---|
| Orbital cellulitis | Unilateral; no bilateralization; no cranial nerve palsies (usually); no septicemia |
| Tolosa-Hunt syndrome | Painful ophthalmoplegia but no fever, no proptosis/chemosis; steroid-responsive; recurrent |
| Carotid-cavernous fistula | Pulsatile proptosis; bruit; arterialized conjunctival vessels; no fever |
| Orbital pseudotumor (IgG4) | Steroid-responsive; no systemic infection |
| Mucormycosis | Diabetic/immunocompromised; black eschar on palate/nasal mucosa; rapid progression |
| Pituitary apoplexy | Sudden onset; bilateral CN III; no fever; CT/MRI shows hemorrhagic pituitary |
| Sphenoid wing meningioma | Chronic, no infection, enhancing mass on MRI |
Treatment
1. Antibiotics (Primary)
- IV antibiotics directed at S. aureus (including MRSA coverage: vancomycin) + gram-negative cover (cefepime or piperacillin-tazobactam)
- If fungal (mucormycosis/Aspergillus) suspected: amphotericin B urgently
- Duration: several weeks (IV), then oral step-down
- Consult Infectious Disease
2. Anticoagulation (Controversial but Commonly Used)
- Heparin → warfarin for septic CST is used in clinical practice to limit thrombosis extension and improve recanalization
- Benefit not proven in RCTs; risk of hemorrhage must be weighed
- Aseptic CST: systemic anticoagulation with heparin or aspirin 325 mg daily — Wills Eye Manual
3. Surgical
- Drainage of the primary infectious source (sinus surgery, orbital abscess drainage)
4. Ophthalmic-Specific Management
| Problem | Management |
|---|---|
| Exposure keratopathy (lagophthalmos from CN VII involvement or extreme proptosis) | Preservative-free lubricating drops/ointment, taping, moisture chambers |
| Secondary glaucoma (elevated episcleral venous pressure) | Manage as open-angle glaucoma (avoid miotics); see POAG protocol |
| Corneal anesthesia (V1 involvement) | Aggressive ocular surface protection, consider tarsorrhaphy |
| Visual loss monitoring | Serial VA, fundoscopy, visual fields |
5. Steroids
- Controversial in septic CST; can reduce cranial nerve inflammation but may worsen infection
- Clearly indicated in Tolosa-Hunt syndrome (prednisone 80–100 mg/day, slow taper); improvement within 72 hours is diagnostic
— Wills Eye Manual; Kanski's Clinical Ophthalmology, 10e; Adams and Victor's Neurology, 12e
Prognosis
| Outcome | Comment |
|---|---|
| Mortality (treated) | ~20–30% (KJ Lee); 20% (Goldman-Cecil) |
| Mortality (untreated) | Up to 100% |
| Cranial nerve palsies | Usually resolve to a large extent with treatment |
| Visual loss | Often permanent — retrobulbar optic neuropathy leaves residual deficit even with successful treatment |
| Bilateral blindness | Can occur from bilateral ICA involvement or bilateral optic neuropathy |
Recent Literature
Three recent reviews (2023–2024) are relevant:
- Long B, Field SM, Singh M. "High risk and low prevalence diseases: Cavernous sinus thrombosis." Am J Emerg Med. 2024 Sep. [PMID: 38959601] — Comprehensive emergency medicine review emphasizing diagnostic pitfalls and management.
- Pelletier J et al. "High risk and low prevalence diseases: Orbital cellulitis." Am J Emerg Med. 2023 Jun. [PMID: 36893591] — Reviews the spectrum from orbital cellulitis to CST, Chandler classification, and emergent management.
- Maniaci A et al. "Ocular Manifestations of Pediatric Rhinosinusitis." Diseases. 2024 Oct. [PMID: 39452482] — Focuses on the rhinosinusitis → CST pathway and ophthalmic outcomes, including pediatric-specific considerations.
Summary: Ophthalmologic Key Points
- CN VI palsy is the earliest and most sensitive sign of cavernous sinus involvement — any painful lateral gaze palsy warrants urgent CST workup
- Bilateralization within 24–48 hours is the hallmark distinguishing CST from orbital cellulitis
- The superior ophthalmic vein is the highway of infection: dilated, non-enhancing SOV on MRI is an early imaging sign
- Retrobulbar optic neuropathy with visual loss is often irreversible — do not delay treatment
- Exposure keratopathy and secondary glaucoma are direct ophthalmic complications requiring concurrent management
- MRI + MR venography is the imaging of choice; loss of flow void and heterogeneous cavernous sinus signal confirm the diagnosis
- Mortality without treatment approaches 100%; diagnosis must be made rapidly on clinical + imaging grounds
Sources: Kanski's Clinical Ophthalmology 10e; Wills Eye Manual; Adams and Victor's Principles of Neurology 12e; Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology 8e; Goldman-Cecil Medicine; KJ Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.