Visual acuity
Reading File
Finding Sources
Searching the Web
visual acuity definition measurement clinical testing
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of visual acuity drawn from multiple authoritative textbooks.
Visual Acuity
Definition
Visual acuity (VA) is the ability of the eye to resolve fine spatial detail - specifically, the minimum angle of separation (subtended at the nodal point of the eye) between two objects that allows them to be perceived as distinct. It is the standard measure of the clarity of central (foveal) vision.
- Kanski's Clinical Ophthalmology, 10th Ed.
Physiological Basis
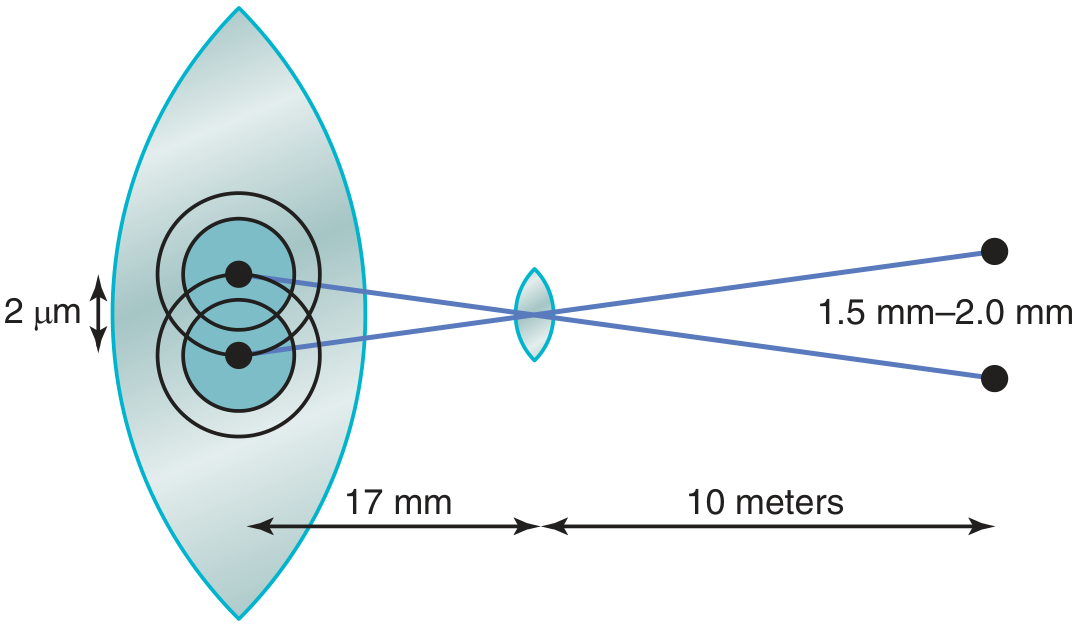
The resolving power of the eye is limited by the optics of the lens system and the density of photoreceptors in the fovea.
- Light from a point source, even when perfectly focused, forms a retinal spot of about 11 micrometers in diameter (due to optical imperfections).
- Foveal cones average 1.5 micrometers in diameter, and two separate points can be distinguished when their centers are at least ~2 micrometers apart on the retina.
- Normal VA corresponds to a minimum separable angle of approximately 25 seconds of arc - meaning two bright pinpoints 10 meters away can just be resolved if they are 1.5-2.0 mm apart.
-
The fovea is less than 0.5 mm in diameter; maximum VA exists within less than 2 degrees of the visual field. VA drops more than 10-fold as you move to the retinal periphery, because more rods and cones converge onto each optic nerve fiber in peripheral regions.
-
In the fovea, each cone synapses on a single bipolar cell, which synapses on a single ganglion cell - providing a direct, high-fidelity pathway to the brain.
-
Guyton & Hall Medical Physiology; Ganong's Review of Medical Physiology
Clinical Notation (Snellen Fraction)
The Snellen fraction expresses VA as a ratio of two distances:
Numerator = testing distance (usually 20 feet or 6 meters) Denominator = distance at which a person with normal vision can read that line
| Notation | Meaning |
|---|---|
| 20/20 (6/6) | Normal - reads at 20 ft what a normal person reads at 20 ft |
| 20/40 (6/12) | Reads at 20 ft what a normal person reads at 40 ft |
| 20/200 (6/60) | Reads at 20 ft what a normal person reads at 200 ft (legal blindness threshold in USA) |
Normal corrected VA in young adults is often better than 6/6. Best-corrected VA (BCVA) is the level achieved with optimal refractive correction.
Testing Methods
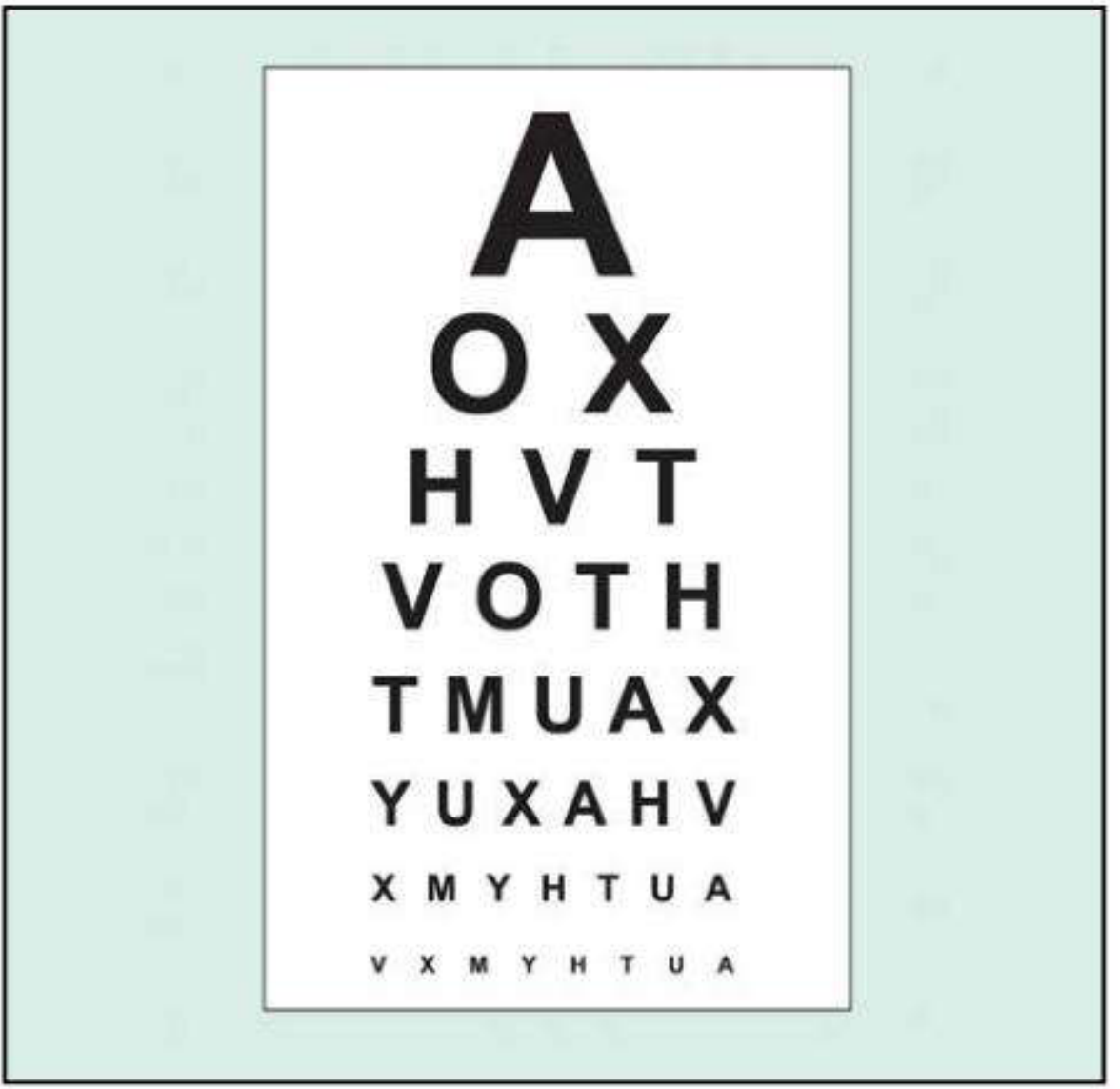
Snellen Chart (Standard)
The most widely used method. The patient reads progressively smaller black optotypes (letters/symbols) on a white chart from a standard distance of 20 feet (6 m).
Protocol:
- Test the eye with worse vision first; occlude the other eye.
- Test with the patient's habitual refractive correction (glasses/contact lenses).
- Push the patient to read every possible letter.
- Record unaided and best-corrected VA separately.
- Binocular VA is usually superior to the better monocular VA.
Pinhole Test
A pinhole aperture (~1 mm diameter) compensates for the effect of refractive error. If VA improves with a pinhole, the deficit is likely refractive (correctable). Note: pinhole VA can be paradoxically worse in macular disease or posterior lens opacities.
Near Vision Card
Used when testing at 20 feet is impractical; held at 14 inches (35 cm). Useful for quick screening in non-ophthalmology settings.
Grading Very Poor VA
When VA is below the range of standard Snellen charts, the following hierarchy is used:
| Grade | Abbreviation | Meaning |
|---|---|---|
| Counting fingers | CF | Patient counts fingers held up at specified distance (usually 1 m) |
| Hand movements | HM | Patient detects whether examiner's hand is moving |
| Perception of light | PL | Patient detects only light (e.g., pen torch), no shapes |
| No perception of light | NPL | Complete blindness |
- Kanski's Clinical Ophthalmology, 10th Ed.
Testing in Preverbal Children
Standard charts cannot be used in infants/toddlers. Alternatives include:
-
Fixation and following behavior - using a face or bright target; tests visual alertness.
-
Occlusion preference - strong objection to occluding one eye suggests poorer acuity in the other eye.
-
Rotation test - brisk rotation of the child; presence of nystagmus and post-rotation suppression indicates functional vision.
-
Preferential looking tests (PLT) - Teller acuity cards, Keeler cards, or Cardiff acuity cards. Based on the infant's preference to look at patterned stimuli over homogeneous fields. Assesses resolution VA (grating acuity), which may overestimate VA in amblyopia.
-
Pattern visual evoked potentials (VEP) - objective measure of spatial acuity; more commonly used for diagnosing optic neuropathy.
-
For children older than ~42 months: standard wall charts (Snellen, tumbling E, HOTV charts) can be used.
-
Kanski's Clinical Ophthalmology, 10th Ed.; Textbook of Family Medicine, 9th Ed.
Clinical Relevance
- Amblyopia screening: Measuring VA (or fixation preference) of each eye separately is the best way to detect visual loss from amblyopia.
- Legal blindness: VA of 20/200 or worse in the better eye (with correction) meets the US legal definition.
- Driving standards: Many jurisdictions require minimum VA (commonly 20/40 or better) for licensure.
- Disease monitoring: VA is a primary outcome measure in conditions like macular degeneration, diabetic retinopathy, glaucoma, and optic neuritis.
- Neurological assessment: Sudden change in VA is a red flag for optic nerve, chiasmal, or cortical pathway disease.
This is a shared conversation. Sign in to Orris to start your own chat.