Lung abscess as per harrison with clinical feature, management and dd
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive Harrison's-based answer. Here is the complete write-up:
Lung Abscess - Harrison's Principles of Internal Medicine (22nd Ed.)
Definition
Lung abscess represents necrosis and cavitation of the lung following microbial infection. Abscesses can be single or multiple but are usually marked by a single dominant cavity >2 cm in diameter.
Classification
| Type | Description |
|---|---|
| Primary (~80%) | Arises from aspiration; caused chiefly by anaerobes; no underlying pulmonary/systemic condition |
| Secondary (~20%) | Arises in setting of bronchial obstruction (foreign body, tumor) or systemic immunocompromise |
| Acute | Duration <4-6 weeks |
| Chronic | ~40% of cases; duration >4-6 weeks |
Etiology / Microbiology (Harrison's Table 132-1)
| Clinical Condition | Pathogens |
|---|---|
| Primary lung abscess (aspiration risk) | Anaerobes: Peptostreptococcus spp., Prevotella spp., Bacteroides spp., milleri group streptococci; microaerophilic streptococci |
| Secondary lung abscess (immunocompromise) | S. aureus, gram-negative rods (P. aeruginosa, Enterobacteriaceae), Nocardia, Aspergillus, Mucorales, Cryptococcus, Legionella, Rhodococcus equi, Pneumocystis jirovecii |
| Embolic lesions | S. aureus (from endocarditis), Fusobacterium necrophorum (Lemierre's syndrome) |
| Endemic infections | M. tuberculosis, M. avium, M. kansasii, Coccidioides spp., Histoplasma capsulatum, Blastomyces spp., parasites (E. histolytica, Paragonimus westermani, Strongyloides) |
| Miscellaneous | S. aureus post-influenza/viral infection, Actinomyces spp. |
Epidemiology & Risk Factors
- More common in middle-aged men
- Major risk factor: aspiration (the common pathway)
- High-risk groups:
- Altered mental status, alcoholism, drug overdose, seizures
- Bulbar dysfunction, prior cerebrovascular events, neuromuscular disease
- Esophageal dysmotility, strictures, or tumors
- Gastroesophageal reflux; recumbent position
- Gingivitis/periodontal disease - gingival crevices colonized by anaerobes serve as the bacterial nidus; lung abscess is considered extremely rare in edentulous patients
Pathogenesis
Primary abscesses: Anaerobes + microaerophilic streptococci from gingival crevices are aspirated into lung parenchyma. Over 7-14 days, bacteria produce parenchymal necrosis and cavitation. Extent depends on host-pathogen interaction. Polymicrobial anaerobic infections produce more extensive tissue necrosis via synergistic virulence factors.
Secondary abscesses: Bronchial obstruction (by malignancy/foreign body) leads to distal atelectasis and superinfection. In immunocompromised patients, pathogens such as Aspergillus or Mucorales cause angioinvasion with subsequent necrosis.
Lemierre's syndrome: A specific form caused by Fusobacterium necrophorum - oropharyngeal/tonsillar infection leads to thrombophlebitis of the internal jugular vein with septic emboli to the lungs.
Clinical Features
Symptoms
- Subacute presentation typical - symptoms develop over days to weeks
- Cough - initially non-productive, later productive
- Foul-smelling / putrid sputum - hallmark feature indicating anaerobic infection
- Pleuritic chest pain
- Fever and chills
- Night sweats
- Hemoptysis - can occur, rarely massive
- Weight loss and fatigue (especially chronic cases)
- Dyspnea
Signs
- Fever (high-grade, often >39°C)
- Tachycardia, tachypnea
- Dullness to percussion over involved area
- Bronchial or amphoric breath sounds over the cavity
- Decreased breath sounds, crackles
- Clubbing may be present in chronic cases
- Signs of periodontal disease / poor dentition commonly present
- Altered mental status in high-risk (aspirating) patients
CT Scan Image (Harrison's Fig. 132-1)
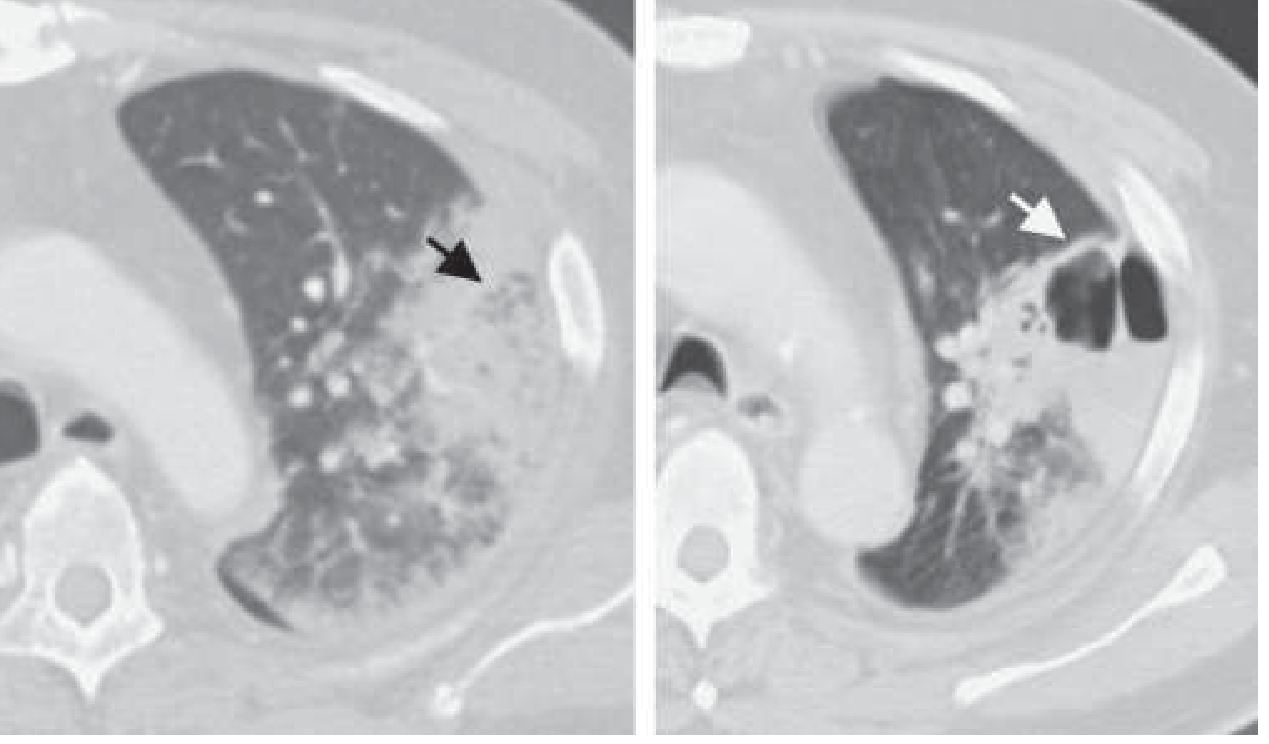
Left panel: Early consolidation (black arrow). Right panel: Follow-up CT after treatment showing cavitation with air-fluid level (white arrow), classic for lung abscess.
Diagnosis
Laboratory
- CBC: Leukocytosis with left shift; leukopenia may suggest immunocompromise or overwhelming sepsis
- Elevated ESR, CRP
- Blood cultures (positive in ~15% of cases; more likely in secondary/embolic abscesses)
- HIV testing in appropriate patients
- Serum LDH may be elevated
Imaging
- CXR: Thick-walled cavity, often with air-fluid level; predilection for posterior segments of upper lobes and superior segments of lower lobes (gravity-dependent zones in recumbent patients)
- CT chest (preferred): Better defines cavity wall thickness, identifies satellite lesions, distinguishes abscess from empyema, detects endobronchial obstruction. Abscesses have thick irregular walls, surrounded by consolidation. CT is critical for ruling out underlying malignancy.
- Classic location: Right lower lobe > right upper lobe posterior segment > left lower lobe (gravity-dependent aspiration)
Microbiological Workup
- Sputum Gram stain and culture (including anaerobic cultures, AFB, fungal stains)
- Bronchoscopy with BAL - recommended, especially in: immunocompromised patients, failure to respond to empirical therapy, suspicion of endobronchial obstruction, or need to rule out malignancy
- BAL specimens should be sent for aerobic, anaerobic (if feasible), mycobacterial, fungal, Nocardia cultures
- CT-guided biopsy of cavity wall if malignancy suspected
- Blood cultures x2
- Thoracentesis if pleural effusion/empyema present
Management
Antibiotic Therapy
Empirical therapy for primary lung abscess (aspiration/anaerobes):
Harrison's recommends coverage directed against anaerobes and microaerophilic streptococci:
| Antibiotic | Notes |
|---|---|
| Amoxicillin-clavulanate (oral) | Good first choice; covers anaerobes + streptococci |
| Clindamycin | Historically the gold standard for anaerobes; IV then oral step-down |
| Beta-lactam/beta-lactamase inhibitor (IV: piperacillin-tazobactam, ampicillin-sulbactam) | For hospitalized patients |
| Metronidazole | NOT used alone - inadequate coverage for microaerophilic streptococci; use in combination |
| Carbapenems (imipenem, meropenem) | Reserve for severely ill or resistant cases |
For secondary abscesses, broaden coverage based on organism (e.g., anti-pseudomonal agents, anti-fungals for mold infections, anti-TB for mycobacteria).
Duration: Typically 3-6 weeks minimum; continue until cavity has resolved or shows marked improvement on imaging. Chronic abscesses may require even longer courses (up to several months).
Drainage
- Postural drainage / chest physiotherapy - important adjunct; position patient to drain dependent segments
- Bronchoscopic drainage - can be used to facilitate drainage and obtain cultures; generally not first-line but useful in non-resolving cases
- Percutaneous catheter drainage - indicated when:
- Abscess fails to respond to antibiotics after 4-6 weeks
- Large abscess (>6-8 cm)
- Communication with pleural space
- Immunocompromised host
- CT-guided; effective in selected patients
- Surgical resection (lobectomy) - reserved for:
- Failure of medical therapy and percutaneous drainage
- Massive hemoptysis
- Underlying malignancy
- Suspected drug-resistant organisms requiring tissue diagnosis
- Rare in the antibiotic era; carries significant morbidity
Supportive Care
- Adequate nutrition (often need supplemental nutrition in chronic cases)
- Bronchodilators if bronchospasm present
- Avoid bronchoscopy early if concern for cavity rupture
- Treat underlying conditions (periodontal disease, GER, etc.)
When to Reassess / Escalate
Harrison's emphasizes that ~85-90% of primary lung abscesses respond to antibiotics alone. Failure to improve after 4-6 weeks of appropriate therapy should prompt:
- Repeat imaging
- Bronchoscopy to rule out obstruction or malignancy
- Review of microbiology; culture-directed therapy
- Consideration of percutaneous or surgical drainage
Differential Diagnosis
Harrison's identifies the following conditions that must be excluded when a cavitary lung lesion is found:
| Category | Conditions |
|---|---|
| Infectious | Necrotizing pneumonia (Klebsiella, S. aureus, Streptococcus pyogenes), tuberculosis and non-tuberculous mycobacteria, endemic fungi (Coccidioides, Histoplasma, Blastomyces), invasive aspergillosis/mucormycosis, paragonimiasis, amoebic abscess (right lower lobe, may communicate with liver) |
| Malignancy | Primary lung carcinoma (squamous cell especially - cavitates with thick irregular walls), metastatic disease (cavitating mets), lymphoma |
| Inflammatory/Vasculitic | Granulomatosis with polyangiitis (GPA/Wegener's) - cavitating nodules; rheumatoid arthritis - necrobiotic nodules |
| Cystic/Structural | Infected pulmonary cyst or bulla, bronchogenic cyst, sequestration |
| Other | Cavitary infarct (pulmonary embolism), empyema with bronchopleural fistula (air-fluid level crossing pleural fissure - distinguished on CT), hydatid cyst (Echinococcus) |
Key distinguishing features:
- Thin-walled cavity - favors cyst, bulla, or resolved infarct
- Thick irregular wall - favors malignancy or active infection
- Air-fluid level - strongly supports abscess
- Location in dependent zones - strongly supports aspiration-related abscess
- Satellite lesions, lymphadenopathy - may suggest malignancy or TB
- Foul sputum + periodontal disease - virtually pathognomonic of anaerobic lung abscess
Complications
- Hemoptysis (can be massive/life-threatening)
- Bronchopleural fistula
- Empyema thoracis
- Mediastinitis (rare, very serious)
- Septicemia / metastatic infection
- Amyloidosis (rare, chronic cases)
Prognosis
- Primary lung abscess with anaerobes: excellent - ~85-90% cure with antibiotics alone
- Poor prognostic factors:
- Secondary abscess (underlying malignancy, immunocompromise)
- Cavity >6 cm
- Aerobic gram-negative or S. aureus causative organisms
- Age extremes
- Delayed diagnosis and treatment
- Obstruction from malignancy
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 132 - Lung Abscess (Baron RM, Baron BW, Barshak MB)
Liver abscess
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have excellent comprehensive content from Harrison's on both pyogenic and amebic liver abscesses. Let me compile the full detailed answer:
Liver Abscess - Harrison's Principles of Internal Medicine (22nd Ed.)
Liver abscess is a focal collection of pus within the hepatic parenchyma. There are two major types: pyogenic (bacterial) liver abscess and amebic liver abscess. Their distinction is clinically important as management differs significantly.
PYOGENIC LIVER ABSCESS
Etiology & Pathogenesis
Pyogenic liver abscesses arise from bacterial seeding of the liver via several routes:
| Route | Source | Common Organisms |
|---|---|---|
| Portal vein (most common) | Intraabdominal infection (appendicitis, diverticulitis, IBD, perforated viscus) | Mixed aerobic/anaerobic (Enterobacteriaceae, B. fragilis, streptococci) |
| Biliary tract (ascending cholangitis) | Biliary obstruction - stones, strictures, malignancy, post-ERCP | E. coli, Klebsiella, Enterococci, anaerobes |
| Direct extension | Adjacent hepatic or subphrenic infection | Variable |
| Hepatic artery (bacteremia) | Systemic sepsis, endocarditis | S. aureus, streptococci |
| Cryptogenic (~50%) | No identifiable source | Klebsiella pneumoniae (hypervirulent strain - hvKp) |
Special note on hvKp (Hypervirulent Klebsiella pneumoniae): Harrison's highlights this as an emerging distinct entity. hvKp causes community-acquired monomicrobial pyogenic liver abscess predominantly in younger, previously healthy individuals - especially those of Asian ethnicity and diabetics. It spreads metastatically and can cause endophthalmitis, meningitis, splenic/brain abscess, and necrotizing fasciitis. Most cases reported from the Asian Pacific Rim. MDR/XDR variants combining hvKp virulence with carbapenemase/ESBL resistance are an emerging threat.
Abscess pathogenesis (Harrison's Ch. 135): Bacteroides fragilis is the most frequently isolated anaerobe. Its capsular polysaccharide complex (with zwitterionic polysaccharides including PSA) evokes host T-lymphocyte and macrophage responses that localize bacteria into abscesses. PMNs, complement, and fibrinogen also participate. The abscess acts as both a disease state and a host containment mechanism.
Clinical Features of Pyogenic Liver Abscess
Symptoms:
- Fever (hectic, with chills/rigors) - most consistent finding
- Right upper quadrant (RUQ) pain - dull or colicky; may radiate to right shoulder
- Nausea and vomiting
- Anorexia and weight loss
- Malaise and fatigue
- Symptoms of underlying source (appendicitis, cholangitis, etc.)
Signs:
- Hepatomegaly - tender
- RUQ tenderness on palpation
- Jaundice - in biliary source or large abscesses compressing bile ducts (~25%)
- High fever (>38.5°C)
- Reduced breath sounds at right base (reactive pleural effusion)
- Rarely: palpable mass
Lab findings:
- Leukocytosis with left shift
- Elevated alkaline phosphatase (most sensitive LFT - elevated in ~90%)
- Elevated bilirubin, elevated transaminases (moderate)
- Elevated ESR, CRP
- Hypoalbuminemia (chronic/severe cases)
- Blood cultures positive in ~50% of cases
Diagnosis of Pyogenic Liver Abscess
Imaging:
- Ultrasound - first-line; shows hypoechoic lesion; can guide drainage; sensitivity ~85%
- CT abdomen with contrast - gold standard; shows ring-enhancing hypodense lesion with surrounding hepatic edema; better for small lesions; identifies source (biliary/appendix)
- MRI - useful for complex cases
- CXR - elevated right hemidiaphragm, right pleural effusion, atelectasis
Microbiologic workup:
- Blood cultures (aerobic + anaerobic) x2 before antibiotics
- Abscess aspirate: Gram stain + aerobic, anaerobic, AFB, fungal cultures
- Serology for E. histolytica to exclude amebic abscess
Management of Pyogenic Liver Abscess
1. Antibiotics
Empirical therapy must cover gram-negatives (Enterobacteriaceae), anaerobes, and enterococci:
| Regimen | Agents |
|---|---|
| Standard empirical | Piperacillin-tazobactam OR ampicillin-sulbactam |
| Alternative | Metronidazole + third-generation cephalosporin (ceftriaxone) |
| Carbapenem | Meropenem/imipenem - for severe/MDR cases |
| If hvKp suspected | Ceftriaxone (usually susceptible); adjust if resistant |
- Transition to oral therapy after clinical improvement
- Duration: typically 4-6 weeks total (longer for large or multiple abscesses)
- Treat underlying source simultaneously (biliary drainage, appendectomy, etc.)
2. Drainage
Percutaneous drainage (CT or US-guided) - mainstay of treatment:
- Indicated for most pyogenic abscesses >3-4 cm
- Needle aspiration (single or repeated) - suitable for smaller lesions (<5 cm)
- Catheter drainage - for large (>5 cm) or multiloculated abscesses; left in situ until output minimal
Surgical drainage - indications:
- Failed percutaneous drainage
- Ruptured abscess with peritonitis
- Multiple lesions not amenable to percutaneous approach
- Need to address underlying surgical source (perforated viscus, etc.)
3. Treat Underlying Cause
- Biliary: ERCP with sphincterotomy/stenting, cholecystectomy
- Appendicular: appendectomy
- Diverticular: colectomy if needed
AMEBIC LIVER ABSCESS
Etiology & Epidemiology
- Caused by Entamoeba histolytica (not E. dispar which is non-pathogenic)
- Most common extraintestinal manifestation of amebiasis
- Predominantly affects men aged 30-60 years - 10-12x more common than in women of same age (testosterone increases susceptibility via modulation of NK T-cell IFN-γ secretion)
- Travelers to endemic areas: 95% develop amebic liver abscess within 5 months of returning
- Endemic areas: South Asia, Sub-Saharan Africa, Central/South America, Mexico
Pathogenesis
- Ingestion of E. histolytica cysts via fecal-oral route
- Cysts excyst in intestine → trophozoites colonize colon
- Trophozoites invade colonic mucosa → portal venous invasion
- E. histolytica is resistant to complement-mediated lysis (survives in bloodstream)
- In liver: acute neutrophilic infiltrate → neutrophils lysed by amebae (neutrophil toxins contribute to hepatocyte necrosis)
- Liver parenchyma replaced by necrotic material - classically described as "anchovy paste" (reddish-brown, bacteriologically sterile fluid, composed of granular debris with few cells)
- Amebae tend to be found near the capsule of the abscess (not centrally)
Clinical Features of Amebic Liver Abscess
Symptoms:
- Fever - present in most patients (>38.5°C)
- RUQ pain - dull or pleuritic, may radiate to the right shoulder
- Younger patients: acute presentation (<10 days' symptoms)
- Older patients from endemic areas: subacute/chronic course (up to 6 months) with weight loss and hepatomegaly; only ~1/3 febrile in chronic presentation
- Diarrhea - present in <1/3 of patients (colon is primary infection site but active diarrhea is often absent)
- Anorexia, malaise
- 10-15% present with fever alone → amebic liver abscess must be in differential for fever of unknown origin (FUO)
Signs:
- Point tenderness over the liver - characteristic
- Right-sided pleural effusion - common
- Hepatomegaly
- Jaundice - rare (differentiates from pyogenic in which jaundice is more common)
- Generally less toxic-appearing than pyogenic liver abscess
Key differentiating features: Amebic vs. Pyogenic
| Feature | Amebic | Pyogenic |
|---|---|---|
| Age/sex | Men 20-50 yrs | Any age |
| Endemic area | Yes (travel history) | No specific geography |
| Number of lesions | Usually single, right lobe | Often single, can be multiple |
| Jaundice | Rare | ~25% |
| Blood cultures | Negative | Positive ~50% |
| Stool parasites | <1/3 | Not applicable |
| Serology | Positive >90% | Negative |
| Aspirate | Anchovy-paste; sterile | Purulent; organisms on Gram stain |
| Response to metronidazole | Dramatic (72h) | No response |
Complications of Amebic Liver Abscess
- Pleuropulmonary involvement - most frequent complication (20-30%):
- Sterile effusions (resolve with medical therapy)
- Contiguous spread from liver
- Rupture into pleural space (requires drainage)
- Hepatobronchial fistula - cough productive of large amounts of necrotic material ("anchovy paste sputum"); carries good prognosis
- Rupture into peritoneum - may be indolent or acute abdomen; requires percutaneous catheter drainage + medical therapy
- Pericardial rupture (left lobe abscess) - gravest prognosis; requires surgical drainage; can occur even during active medical therapy
- Genitourinary involvement - direct extension or hematogenous spread; painful genital ulcers
- Cerebral amebiasis - <0.1% of cases
Diagnosis of Amebic Liver Abscess
Laboratory:
- Leukocytosis >10,000/μL in ~75% (especially acute presentations)
- Elevated alkaline phosphatase, mild transaminase elevation
- Elevated ESR, CRP
- Mild normochromic anemia
Stool examination:
- Wet mounts + iodine-stained concentrates + trichrome stain → confirms diagnosis in 75-95% if cysts/trophozoites found
- Examine at least 3 fresh stool specimens (trophozoites die quickly)
- Hematophagous trophozoites (containing ingested RBCs) are diagnostic
Serology (most useful):
- Indirect hemagglutination (IHA), ELISA, immunodiffusion - positive in >90% of patients with liver abscess
- Results revert to negative within 6-12 months - positive serology = active disease in the appropriate clinical context
- In highly endemic areas, serology less useful (prior exposure common)
- Specific antigen-detection tests (TechLab E. histolytica II) - can distinguish E. histolytica from E. dispar
- PCR available in some centres
Imaging:
- Ultrasound - first-line; amebic abscess typically is a single, round, hypoechoic lesion in the right lobe; no internal echoes
- CT/MRI - homogeneous round/oval lesion, well-defined walls; right lobe predilection
Aspiration (not routine for amebic abscess):
Indications for aspiration per Harrison's:
- Need to rule out pyogenic abscess, especially with multiple lesions
- Lack of clinical response to metronidazole within 3-5 days
- Left lobe abscess (risk of pericardial rupture)
- Imminent rupture (large abscess, bulging)
Management of Amebic Liver Abscess
Drug Therapy
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Metronidazole (drug of choice) | 750 mg PO/IV TID | 5-10 days | >90% respond with fever/pain reduction within 72h |
| Tinidazole (alternative) | 2 g PO once daily | 3-5 days | Also effective; longer-acting |
| Ornidazole | 2 g PO once | Single dose | Not available in USA |
Always follow with a luminal agent (to eradicate intestinal cysts and prevent transmission):
- Iodoquinol 650 mg TID x 20 days, OR
- Paromomycin 500 mg TID x 10 days
Metronidazole alone does not eradicate cysts → risk of relapse and spread.
Aspiration/Drainage
- Usually NOT required for uncomplicated amebic liver abscess (responds to metronidazole)
- Indications (as above): rule out pyogenic, no response in 3-5 days, left lobe, imminent rupture
- Pericardial rupture → surgical drainage required
Prognosis
- Mortality <1% with early diagnosis and metronidazole therapy
- Amebic liver abscess rarely recurs
Differential Diagnosis of Liver Abscess
| Condition | Distinguishing features |
|---|---|
| Hepatocellular carcinoma | Alpha-fetoprotein elevated; arterial enhancement on CT; no fever initially; HBV/HCV history |
| Metastatic liver disease | Multiple lesions; known primary malignancy; no fever; CEA/CA19-9 elevated |
| Echinococcal (hydatid) cyst | "Daughter cysts" on imaging; peripheral calcification; eosinophilia; Casoni test; serology for Echinococcus |
| Cholangiocarcinoma | Ductal lesion; biliary dilation; tumor markers |
| Simple hepatic cyst | Thin walls, no enhancement, no fever, no symptoms |
| Hepatic hemangioma | Peripheral nodular enhancement on CT; "fill-in" pattern on delayed phase |
| Biliary cystadenoma/carcinoma | Multiloculated cystic lesion; no fever |
| Infected biloma | Post-traumatic or post-procedural; bile on aspiration |
| Candidal liver abscess | Immunocompromised host; "bull's-eye/target" lesion on CT; antifungal therapy |
| Schistosomiasis | Periportal fibrosis ("pipe-stem"); serology; travel history; eosinophilia |
Sources: Harrison's Principles of Internal Medicine 22nd Ed. (2025) - Ch. 135 (Intraabdominal Abscesses), Ch. 166 (Klebsiella), Ch. 230 (Amebiasis/Amebic Liver Abscess)
This is a shared conversation. Sign in to Orris to start your own chat.