High tibial osteotomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"high tibial osteotomy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from the textbooks. Let me compile the full answer.
High Tibial Osteotomy (HTO)
Definition & Rationale
High tibial osteotomy is a joint-preserving procedure that corrects varus (or rarely valgus) malalignment of the knee by osteotomizing the proximal tibia to shift the mechanical axis away from the diseased compartment. The procedure exploits the fact that medial compartment overload in a varus knee accelerates cartilage degeneration — by redirecting the weight-bearing line laterally, it unloads the worn compartment and reduces pain while preserving the native joint.
The AAOS Evidence-Based Guideline for Management of Knee Osteoarthritis rates HTO as "may be helpful" in properly indicated patients with unicompartmental knee OA. — Miller's Review of Orthopaedics 9th Ed.
Indications
- Varus knee malalignment with medial compartment overload (medial proximal tibial angle [mPTA] <90°)
- Isolated medial compartment arthritis (other two compartments free of disease)
- Pain clinically localised to the medial compartment
- Young, active, well-motivated patient — typically ideal candidate is <45–65 years (arthroplasty less appropriate)
- May be combined with osteochondral resurfacing (MACI/OAT), meniscal repair, or ligament reconstruction — corrective osteotomy is required before or simultaneously with cartilage restoration to prevent graft failure from mechanical overload
- PCL insufficiency with posterior tibial slope: a biplanar HTO can address combined malalignment and PCL insufficiency by altering slope
- Spontaneous osteonecrosis of the knee (SONK): proximal tibial osteotomy is an option for joint preservation in younger patients before subchondral collapse
Contraindications
| Contraindication | Notes |
|---|---|
| Severe OA (stage III–IV) | Multi-compartment disease → arthroplasty preferred |
| Knee flexion <90° (minimum needed) | Predicts poor outcome |
| Flexion contracture >10° | |
| Inflammatory arthritis | Absolute contraindication |
| Varus thrust gait | Indicates lateral capsulo-ligamentous stretch-out |
| Femoro-tibial subluxation >1 cm | Permanently altered kinematics |
| Medial compartment bone loss | |
| Lateral compartment joint narrowing on valgus stress radiograph | |
| Age >65 years | Relative; arthroplasty usually preferred |
| Limited ROM <120° | As per Miller's |
Note: ACL deficiency alone is not a contraindication if all other criteria are met.
Preoperative Planning
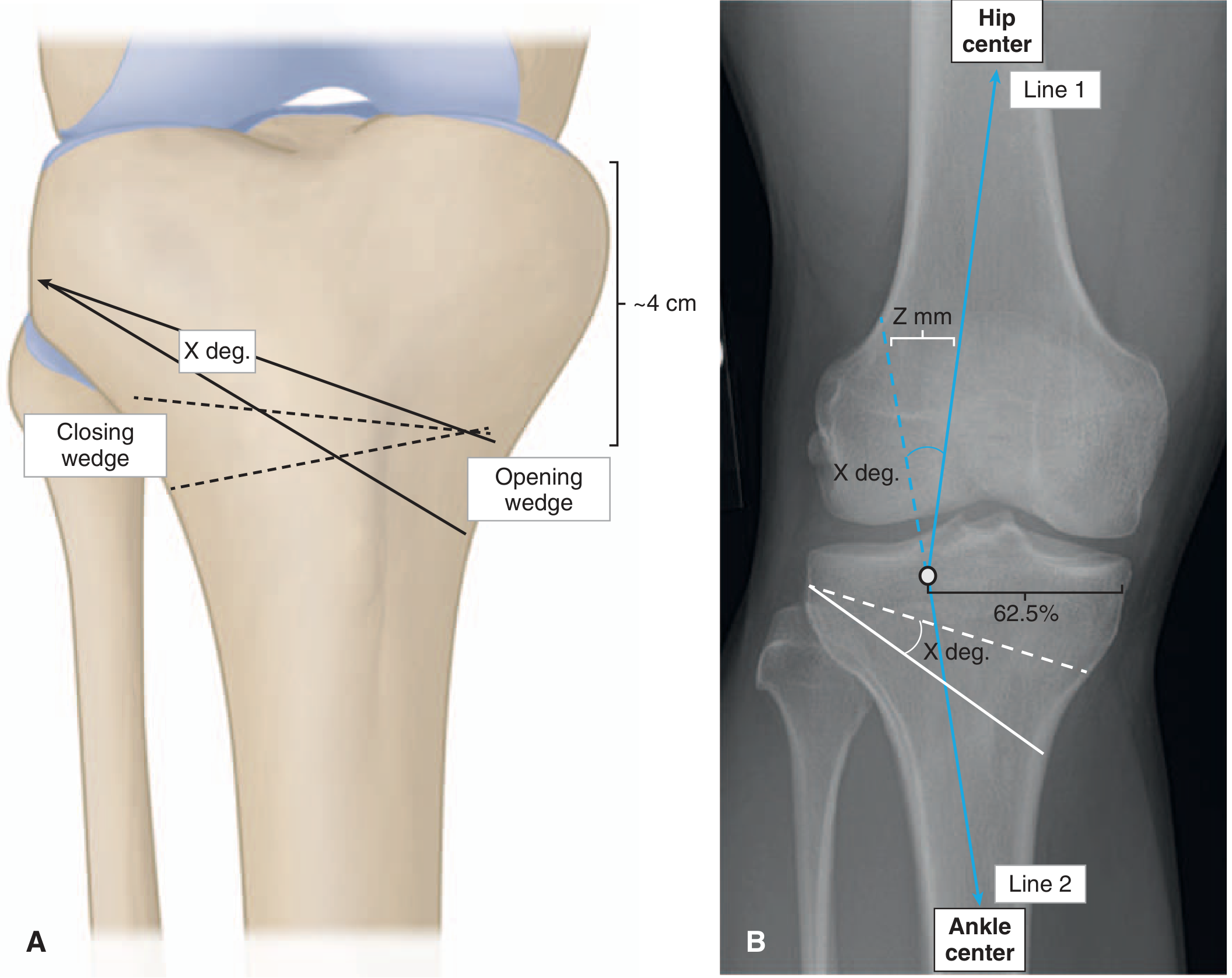
Planning is based on bilateral weight-bearing AP long-leg radiographs (hip-to-ankle):
- The weight-bearing line is drawn from the hip centre to the ankle centre
- The target point on the tibial plateau is 62.5% of the tibial plateau width (lateral to midpoint) — the Fujisawa point
- The angle of correction (X°) is the angle between the current mechanical axis and the desired axis
- The osteotomy is performed ~4 cm distal to the joint line, at the level of the fibular head tip
- The osteotomy gap width (Z mm) is calculated by superimposing the correction angle onto the measured osteotomy line length
Large wedge corrections >8° carry higher complication risk and increased chance of losing correction. — Miller's
Surgical Techniques
1. Medial Opening-Wedge HTO
- Osteotomy is performed medially; a gap is opened to the desired correction angle
- Maintained with a plate and locking screws ± bone graft or substitute
- Modern locking plate fixation allows early weight-bearing and mobilisation
- Advantage: does not require fibular osteotomy; easier to adjust correction intraoperatively
2. Lateral Closing-Wedge HTO
- A bone wedge is removed from the lateral side; the cortices are compressed closed
- Historically required fibular osteotomy
- More inherently stable construct but less adjustable
Both techniques are planned and performed with jigs under radiographic (fluoroscopic) control. — Bailey & Love's 28th Ed.
Complications
Opening-Wedge Technique
- Patella baja (infrapatellar contracture/tendon scarring) — most common complication of both techniques
- Collapse of the open wedge
- Nonunion
- Bone graft harvest site pain
Closing-Wedge Technique
- Patella baja — most common complication → leads to loss of flexion
- Loss of posterior tibial slope → loss of flexion
- Peroneal nerve palsy (from aberrant retractor placement near fibular neck)
General/Other
- Common peroneal nerve injury is a recognised risk of proximal tibial/fibular osteotomy; the nerve supply to extensor hallucis longus is particularly vulnerable — Localization in Clinical Neurology 8th Ed.
- Stress risers from prior HTO fixation holes are a risk factor for periprosthetic fracture if TKA is later performed — Rockwood & Green's 10th Ed.
- Delayed bone healing, especially with stiff locked plate constructs
Outcomes & Survivorship
- Rate of conversion to TKA: ~13% at 6 years (meta-analysis data) — Miller's
- Conversion to TKA after HTO requires longer operative time and more frequent use of revision implants
- The most common long-term failure mode is progression of arthritis to involve additional compartments
HTO vs Distal Femoral Osteotomy (DFO)
| Feature | HTO | DFO |
|---|---|---|
| Deformity | Varus (proximal tibial vara — mPTA <90°) | Valgus (lateral femoral condyle hypoplasia — mLDFA <90°) |
| Goal | Valgus-producing osteotomy | Varus-producing osteotomy |
| Compartment unloaded | Medial | Lateral |
| Patellofemoral effects | Worsens patellofemoral mechanics slightly | Improves PF mechanics (reduces Q angle) |
HTO in Context of Cartilage Restoration
MACI and osteochondral allograft transplantation (OAT) will fail in the presence of mechanical overload from malalignment. HTO must precede or be performed simultaneously with cartilage restoration procedures when malalignment co-exists with a chondral defect. — Miller's Review of Orthopaedics 9th Ed.
Sources: Miller's Review of Orthopaedics 9th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed. | Schwartz's Principles of Surgery 11th Ed. | Rockwood & Green's Fractures in Adults 10th Ed. | Localization in Clinical Neurology 8th Ed.
Make a presentation for orthopaedic audience on high tibial osteotomy
Reading File
Reading File
Reading File
Searching Images
high tibial osteotomy opening wedge closing wedge technique
Searching Images
knee varus deformity mechanical axis weight bearing line radiograph
Searching Images
HTO plate fixation locking screws postoperative radiograph
Searching Images
knee osteotomy complications patella baja peroneal nerve
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not foun…
Running Command
mkdir -p /home/daytona/workspace/hto-presentation && echo "Created"
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.