Brachial plexus
Reading File
Finding Sources
Searching the Web
brachial plexus anatomy roots trunks divisions cords branches clinical
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from the textbooks. Let me compile the full answer.
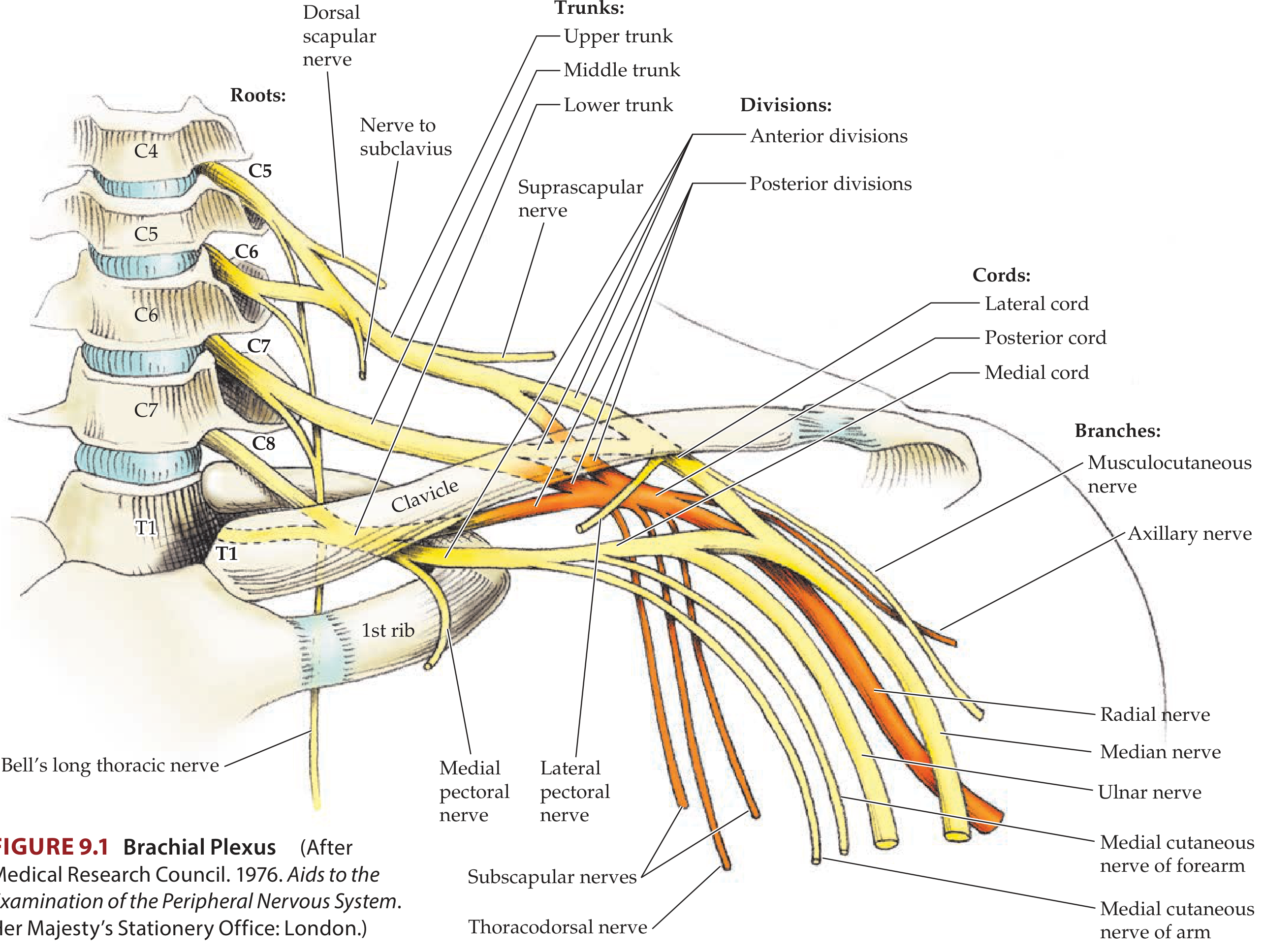
Brachial Plexus
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5-C8 and most of T1. It originates in the neck, passes laterally and inferiorly over rib I, and enters the axilla. It provides all motor and sensory innervation to the upper limb.
Structure: Roots - Trunks - Divisions - Cords - Branches
Mnemonic: Robert Taylor Drinks Cold Beer
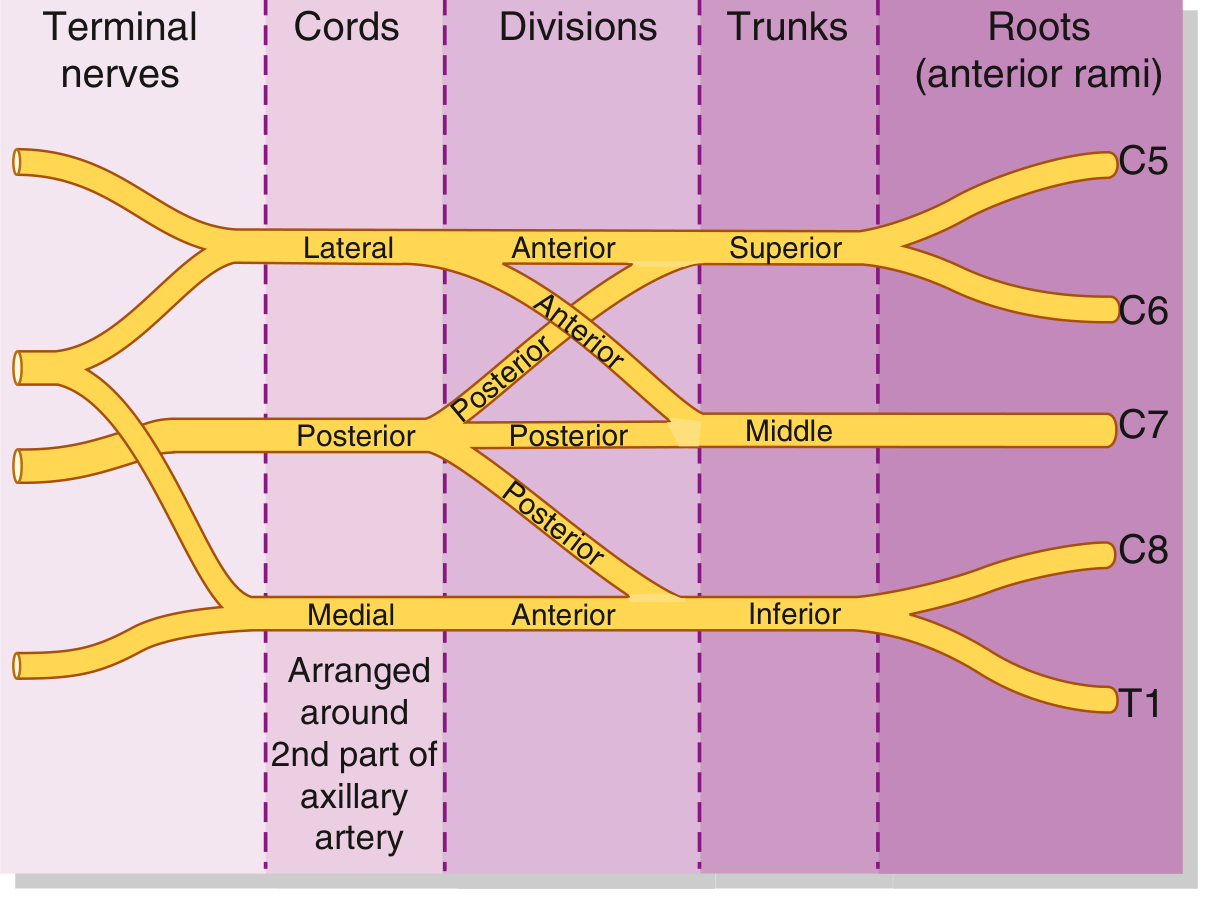
1. ROOTS (C5, C6, C7, C8, T1)
- Formed by the anterior rami of spinal nerves C5-T1
- Emerge between the anterior and middle scalene muscles
- Lie posterior and superior to the subclavian artery
- Receive gray rami communicantes from the sympathetic trunk (postganglionic sympathetic fibers)
- C5 root contributes to the phrenic nerve
Branches from roots:
| Branch | Origin | Innervates |
|---|---|---|
| Dorsal scapular nerve | C5 root | Rhomboid major, rhomboid minor |
| Long thoracic nerve | C5-C7 roots | Serratus anterior |
| Contribution to phrenic nerve | C5 | Diaphragm (partial) |
2. TRUNKS
The three trunks cross the posterior triangle of the neck and pass over rib I:
| Trunk | Formation | Position |
|---|---|---|
| Superior trunk | C5 + C6 roots | |
| Middle trunk | C7 root alone | |
| Inferior trunk | C8 + T1 roots | Lies on rib I, posterior to subclavian artery |
Branches from trunks:
| Branch | Origin | Innervates |
|---|---|---|
| Suprascapular nerve | Superior trunk (C5, C6) | Supraspinatus, infraspinatus |
| Nerve to subclavius | Superior trunk (C5, C6) | Subclavius |
3. DIVISIONS
Each trunk divides into anterior and posterior divisions (6 total). They pass behind the clavicle. No peripheral nerves arise directly from the divisions.
- Three anterior divisions - ultimately supply anterior compartments (flexors)
- Three posterior divisions - ultimately supply posterior compartments (extensors)
4. CORDS
Formed from regrouped divisions, the cords surround the second part of the axillary artery and are named by their relationship to it:
| Cord | Formation | Roots | Position |
|---|---|---|---|
| Lateral cord | Anterior divisions of superior + middle trunks | C5, C6, C7 | Lateral to axillary artery |
| Medial cord | Anterior division of inferior trunk alone | C8, T1 | Medial to axillary artery |
| Posterior cord | All three posterior divisions | C5-T1 | Posterior to axillary artery |
5. BRANCHES (Terminal Nerves)
The five major terminal nerves form the "M" or "W" shape in the axilla:
From the Lateral Cord:
| Branch | Roots | Supplies |
|---|---|---|
| Lateral pectoral nerve | C5-C7 | Pectoralis major (+ minor via communication) |
| Musculocutaneous nerve | C5-C7 | Biceps, brachialis, coracobrachialis (BBC mnemonic); sensory to lateral forearm |
| Lateral root of median nerve | C5-C7 | Joins with medial root to form median nerve |
From the Medial Cord:
| Branch | Roots | Supplies |
|---|---|---|
| Medial pectoral nerve | C8, T1 | Pectoralis major and minor |
| Medial cutaneous nerve of arm | C8, T1 | Skin over medial distal arm |
| Medial cutaneous nerve of forearm | C8, T1 | Skin over medial forearm |
| Ulnar nerve | C8, T1 | Intrinsic hand muscles, medial 1.5 fingers |
| Medial root of median nerve | C8, T1 | Joins lateral root to form median nerve |
From the Posterior Cord (mnemonic: STAR or ARTS):
| Branch | Roots | Supplies |
|---|---|---|
| Superior subscapular nerve | C5, C6 | Subscapularis (upper) |
| Thoracodorsal nerve | C6-C8 | Latissimus dorsi |
| Axillary nerve | C5, C6 | Deltoid, teres minor; sensory to lateral arm |
| Radial nerve | C5-T1 | All posterior compartment muscles of arm and forearm; sensory to posterior arm, forearm, dorsum of hand |
| Inferior subscapular nerve | C5, C6 | Subscapularis (lower), teres major |
Clinical Correlates
Brachial Plexus Injuries - Overview
Injuries can be supraclavicular (roots/trunks - most common, due to shoulder trauma) or infraclavicular (cords/divisions - from glenohumeral dislocation).
"Spinal cord injuries in the cervical region and direct pulling injuries tend to affect the roots. Severe trauma to the first rib usually affects the trunks. The divisions and cords can be injured by dislocation of the glenohumeral joint."
- Gray's Anatomy for Students
Erb's Palsy (Upper Brachial Plexus Injury - C5, C6)
- Mechanism: Forceful separation of head from shoulder - birth injury (shoulder dystocia), motorcycle accidents, improper anesthesia positioning
- Muscles affected: Deltoid, supraspinatus, infraspinatus, biceps, brachialis, brachioradialis
- Classic posture: "Waiter's tip" - arm adducted, internally rotated, elbow extended, forearm pronated, wrist flexed
- Loss: Abduction, external rotation, elbow flexion, supination
- Reflex loss: Biceps reflex absent; Moro reflex asymmetric in neonates
Klumpke's Palsy (Lower Brachial Plexus Injury - C8, T1)
- Mechanism: Forceful arm abduction (breech delivery, grabbing overhead during fall)
- Muscles affected: Intrinsic hand muscles (interossei, lumbricals, thenar, hypothenar); flexors of the wrist and fingers
- Classic posture: "Claw hand" - loss of intrinsic muscles
- Associated: Horner syndrome (involvement of T1 sympathetic fibers) - ptosis, miosis, anhidrosis
Individual Nerve Injuries
| Nerve | Common Cause | Key Finding |
|---|---|---|
| Long thoracic (C5-C7) | Carrying heavy loads on shoulder | Winged scapula (serratus anterior loss) |
| Axillary (C5-C6) | Anterior shoulder dislocation, surgical neck humerus # | Deltoid weakness; loss of sensation lateral arm ("regimental badge" area) |
| Radial (C5-T1) | Humeral shaft fracture (spiral groove), crutch injury | Wrist drop - finger and wrist extension lost; "Saturday night palsy" |
| Musculocutaneous (C5-C7) | Rare; axillary trauma | Weak elbow flexion/supination; sensory loss lateral forearm |
| Median (C5-T1) | Carpal tunnel syndrome, wrist laceration | "Hand of oath" / "Ape hand"; thenar wasting; loss of thumb opposition; sensory loss lateral 3.5 digits |
| Ulnar (C8-T1) | Medial epicondyle fracture, cubital tunnel | Claw hand (ring and little fingers); Froment's sign; loss of pinch grip; sensory loss medial 1.5 digits |
Obstetric Brachial Plexus Palsy (Birth Injury)
- Incidence: 0.4-4% of live births
- Upper root (C5-C6) most common -> Erb's palsy
- Recovery within 2-4 weeks suggests good prognosis
- Deficits persist in ~25% of patients
- Surgical plexus reconstruction is considered if no spontaneous recovery at 3 months
- (Bradley and Daroff's Neurology in Clinical Practice)
Key Relationships
- Plexus passes between anterior and middle scalene muscles
- Cords are arranged around the second part of the axillary artery (relation used in axillary nerve blocks)
- The subclavian artery is posterior to the anterior scalene; the plexus is posterior and lateral to the artery
- The median nerve is formed by contributions from both lateral (C5-C7) and medial (C8-T1) cords, making it a "bridge" between the two
Sources: Gray's Anatomy for Students | Neuroanatomy through Clinical Cases, 3rd Ed | Color Atlas of Human Anatomy | Bradley and Daroff's Neurology in Clinical Practice | Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.