I have my university exam of 1 st year of subject biochemistry These are the important long answer give me answer of this question "What are isoenzymes ? Give examples. What are their clinical significance in our body ?" and remeber it's a long question and make it easy to memorized
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a thorough, exam-ready answer. Here it is:
ISOENZYMES - Complete Long Answer (Exam Format)
1. DEFINITION
Isoenzymes (also called isozymes) are multiple molecular forms of the same enzyme that:
- Catalyze the same chemical reaction
- Differ from each other in their physical and chemical properties (e.g., electrophoretic mobility, heat stability, Km, pH optimum)
- Arise from genetically determined differences in amino acid sequence
Simple memory trick: "Same job, different forms" - like the same worker (enzyme) wearing different uniforms (protein structure) in different organs.
- Lippincott's Illustrated Reviews: Biochemistry, 8th ed.
2. ORIGIN / HOW THEY ARE FORMED
Isoenzymes arise due to 3 main mechanisms:
| Mechanism | Explanation | Example |
|---|---|---|
| Multiple gene loci | Different genes code for slightly different enzyme proteins | LDH, CK, Amylase |
| Allelic variation (Allozymes) | Different alleles of the same gene | Enzyme variants between individuals |
| Post-translational modification | Same protein modified differently (technically "multiple forms", not true isoenzymes) | Glycosylated forms of ALP |
3. HOW ISOENZYMES ARE SEPARATED
Isoenzymes are separated by electrophoresis - because they have different numbers of charged amino acids, they migrate at different speeds in an electric field.
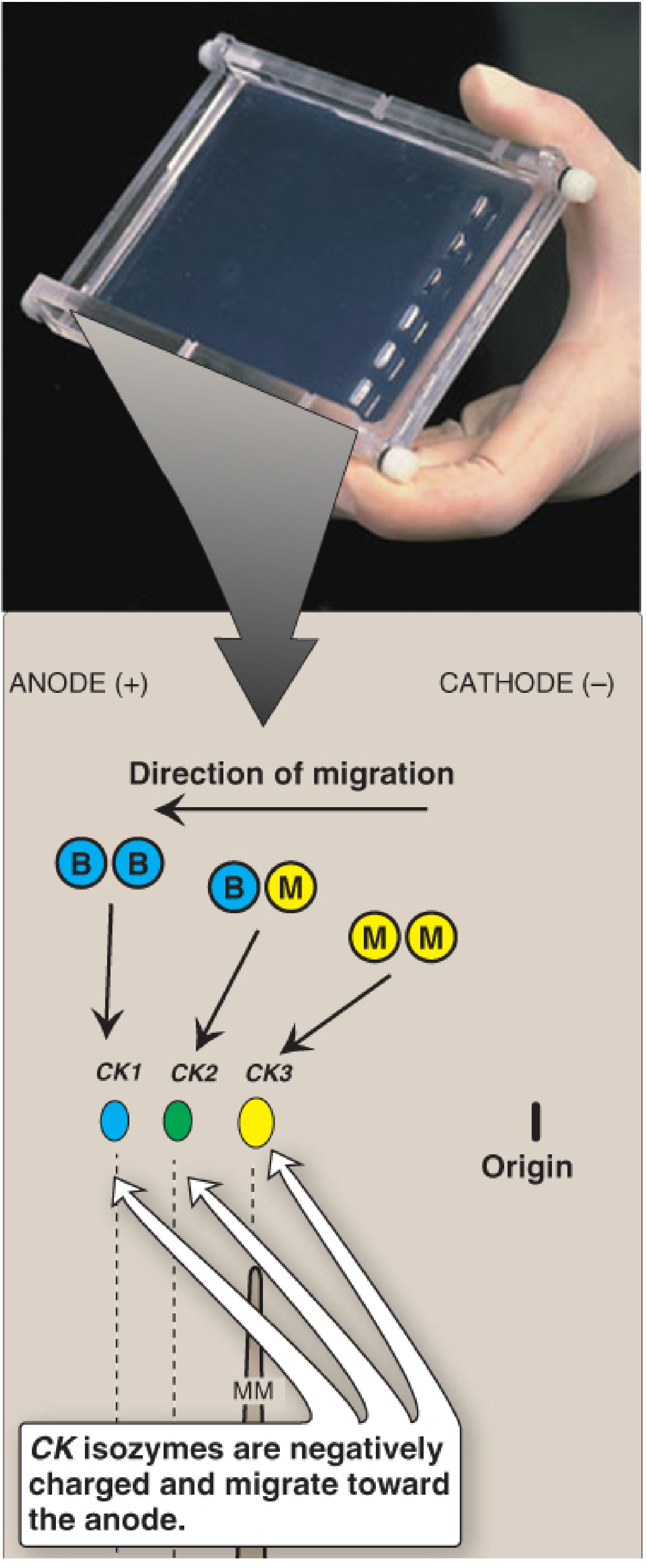
Fig: Electrophoresis of CK isoenzymes - CK1(BB) migrates farthest toward anode, CK3(MM) stays near origin. (Lippincott, Fig. 5.20)
Other separation methods include:
- Immunoassay (using monoclonal antibodies - most common today)
- Heat inactivation
- Chemical inhibition
4. IMPORTANT EXAMPLES
A. Lactate Dehydrogenase (LDH) - 5 Isoenzymes
LDH catalyzes: Pyruvate ⇌ Lactate
LDH exists as a tetramer (4 subunits) made of two types - H (Heart) and M (Muscle):
| Isoenzyme | Subunit Composition | Predominantly Found In |
|---|---|---|
| LD1 | HHHH | Heart muscle, RBCs |
| LD2 | HHHM | Heart, RBCs |
| LD3 | HHMM | Brain, kidney, lung |
| LD4 | HMMM | Liver, skeletal muscle |
| LD5 | MMMM | Liver, skeletal muscle |
Memory trick for LDH: "1-2 Heart, 3 Everywhere, 4-5 Liver"
B. Creatine Kinase (CK) - 3 Isoenzymes
CK catalyzes: Creatine + ATP → Phosphocreatine + ADP
CK exists as a dimer (2 subunits) made of B (Brain) and M (Muscle) subunits:
| Isoenzyme | Subunit Composition | Predominantly Found In |
|---|---|---|
| CK1 (BB) | BB | Brain |
| CK2 (MB) | MB | Cardiac muscle (unique!) |
| CK3 (MM) | MM | Skeletal muscle (majority in heart too) |
Memory trick: "BB = Brain, MB = Myocardium, MM = Muscles"
C. Alkaline Phosphatase (ALP) - 4 Isoforms
| Isoenzyme | Source Tissue |
|---|---|
| ALP-1 | Liver |
| ALP-2 | Bone |
| ALP-3 | Intestine |
| ALP-4 | Placenta |
D. Alpha-Amylase - 2 Isoenzymes
| Isoenzyme | Source |
|---|---|
| Salivary amylase | Parotid gland (gene on chromosome 1) |
| Pancreatic amylase | Pancreas (gene on chromosome 1) |
5. CLINICAL SIGNIFICANCE
This is the most important part - different isoenzymes leak from different damaged organs into blood, so measuring them tells us WHICH organ is injured.
(A) Diagnosis of Myocardial Infarction (Heart Attack)
CK-MB (CK2) is the classic marker of heart muscle damage:
- CK-MB is >5% of total CK ONLY in cardiac muscle - nowhere else
- After a heart attack (MI):
- Appears in blood: 4-8 hours after chest pain
- Peaks: ~24 hours
- Returns to normal: 48-72 hours
Cardiac Troponins (cTnT and cTnI) are now the gold standard (more sensitive/specific):
- Appear: 4-6 hours after MI
- Peak: 24-36 hours
- Remain elevated: 3-10 days (useful for late presentations)
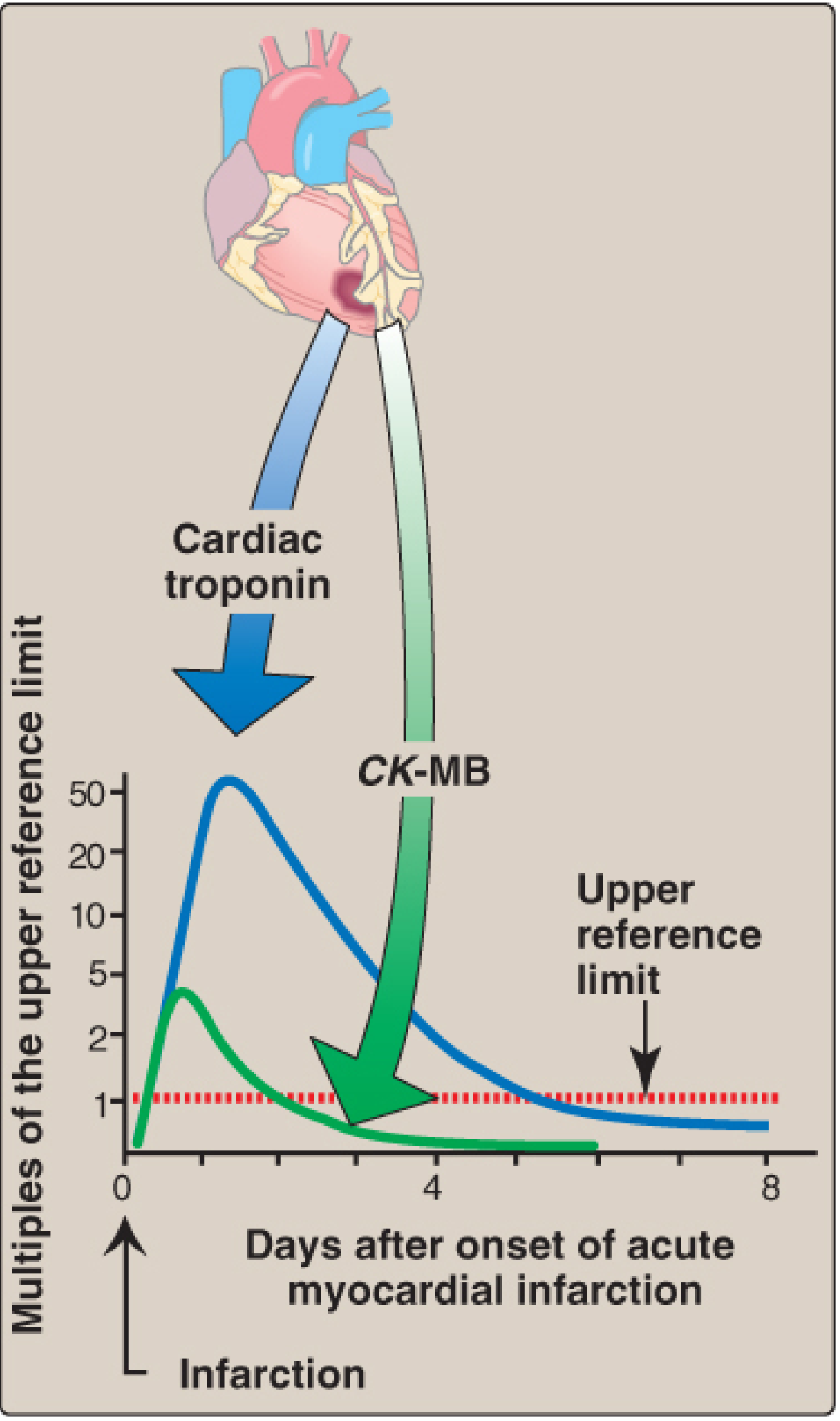
Fig: Troponin rises much higher than CK-MB and stays elevated longer. (Lippincott, Fig. 5.21)
(B) Diagnosis of Liver Disease vs. Bone Disease
Both liver and bone release ALP - but which isoenzyme is elevated tells us the cause:
| Elevated Isoenzyme | Suggests |
|---|---|
| ALP-1 (Liver) elevated | Liver disease (hepatitis, cirrhosis, cholestasis) |
| ALP-2 (Bone) elevated | Bone disease (Paget's disease, bone cancer, rickets) |
| ALP-4 (Placental) elevated | Normal pregnancy |
(C) Diagnosis Using LDH Isoenzymes
| Pattern | Clinical Significance |
|---|---|
| LD1 > LD2 ("flipped pattern") | Myocardial infarction (normally LD2 > LD1) |
| LD5 markedly elevated | Liver damage or skeletal muscle damage |
| LD1-LD2 elevated | Hemolytic anemia (RBC destruction) |
| LD3 elevated | Pulmonary embolism, pancreatitis |
(D) Diagnosis of Brain/Muscle Injury
| Finding | Clinical Meaning |
|---|---|
| CK1 (BB) elevated in CSF | Brain damage (stroke, head injury) |
| CK3 (MM) markedly elevated | Skeletal muscle damage (muscular dystrophy, crush injury) |
(E) Hereditary Diseases
Genetically determined variations in isoenzyme structure explain:
- Differences in drug sensitivity between individuals
- Hereditary metabolic diseases (e.g., enzyme deficiency diseases affecting specific isoforms)
6. SUMMARY TABLE (Quick Revision)
| Enzyme | No. of Isoenzymes | Key Clinical Use |
|---|---|---|
| LDH | 5 (LD1-LD5) | MI, liver disease, hemolytic anemia |
| CK | 3 (BB, MB, MM) | MI (CK-MB), brain injury (CK-BB), muscle injury (CK-MM) |
| ALP | 4 | Liver vs. bone disease |
| Amylase | 2 | Pancreatitis (pancreatic amylase rises) |
| Troponin | Cardiac isoforms | Gold standard for MI |
7. QUICK MEMORY MNEMONICS
- Definition: "Same reaction, different structure, different organ"
- CK subunits: Brain = B, Muscle = M → BB(brain), MB(heart), MM(muscle)
- LDH rule: LD1 = Heart, LD5 = Liver (1 to 5 = Heart to Liver)
- ALP: Liver → ALP-1, Bone → ALP-2 (L before B)
- MI timeline for CK-MB: "4-8 → 24 → 48-72" (appears, peaks, normalizes)
- Troponin is better: Appears same time as CK-MB but stays elevated 3-10 days and rises much higher
Sources: Lippincott's Illustrated Reviews: Biochemistry, 8th ed., p. 202-204 | Tietz Textbook of Laboratory Medicine, 7th ed., p. 771 | Bailey and Love's Surgery, 28th ed.
I am not able to understand how they are formed
Let me give you a super simple, step-by-step explanation of how isoenzymes are formed - no complicated language!
How Isoenzymes Are Formed - Super Simple Explanation
First, understand ONE basic concept:
Enzymes are proteins. Proteins are made from genes (DNA).
So: Gene → mRNA → Protein (Enzyme)
Now, isoenzymes form in 3 ways:
WAY 1: Different Genes Make Slightly Different Enzymes
(Most common - this is the "true" isoenzyme)
Imagine two brothers raised in different cities. They do the same job (both are doctors), but they look slightly different because they developed differently.
In the body:
- Your body has more than one gene that codes for the same type of enzyme
- Each gene is slightly different (due to evolution over millions of years)
- Each gene produces a slightly different version of the enzyme protein
- But ALL versions still do the same job (catalyze the same reaction)
Gene 1 (in Heart) → Enzyme Version H (H subunit)
Gene 2 (in Muscle) → Enzyme Version M (M subunit)
Example - LDH:
- The H-subunit gene is expressed more in the heart
- The M-subunit gene is expressed more in liver/muscle
- These two subunits mix to form 5 combinations = 5 LDH isoenzymes
WAY 2: Mixing of Subunits (like mixing LEGO blocks)
This is how LDH and CK form multiple isoenzymes from just 2 types of subunits.
Think of it like this:
You have 2 types of LEGO blocks: Block H and Block M
You must build a structure using exactly 4 blocks (tetramer).
How many combinations can you make?
H H H H → LD1 (all H blocks)
H H H M → LD2
H H M M → LD3
H M M M → LD4
M M M M → LD5 (all M blocks)
That gives you 5 isoenzymes from just 2 building blocks!
For CK, you use 2 blocks (B and M) to build a structure of 2 blocks (dimer):
B + B → CK1 (BB) found in Brain
B + M → CK2 (MB) found in Heart ← most important!
M + M → CK3 (MM) found in Muscle
Key point: The heart happens to have BOTH B-type and M-type subunit genes active, so it produces the unique CK-MB combination. No other tissue does this significantly.
WAY 3: Same Gene, Different Modifications After Production
(Technically called "multiple forms" not true isoenzymes)
Same protein → gets modified differently → looks different
Like the same plain T-shirt dyed different colors in different shops.
Same ALP protein
↓
In Liver → gets attached to liver cell membrane → ALP-Liver form
In Bone → gets attached to bone cell membrane → ALP-Bone form
In Placenta → gets different sugar attachments → ALP-Placental form
This happens through a process called post-translational modification (modification after the protein is made).
Why does each organ make different isoenzymes?
Because gene expression is tissue-specific.
Not every gene is "switched on" in every cell. Each organ switches on only the genes it needs.
Heart cell: H-subunit gene = ON ✓, M-subunit gene = little ON
Liver cell: H-subunit gene = OFF, M-subunit gene = ON ✓
This is why LD1 (HHHH) is mostly in the heart, and LD5 (MMMM) is mostly in the liver.
The Complete Picture in One Diagram
DNA (Genes)
|
├── Gene H → H subunit protein ┐
| ├─ Mix together → 5 LDH isoenzymes
└── Gene M → M subunit protein ┘
├── Gene B → B subunit protein ┐
| ├─ Mix together → 3 CK isoenzymes
└── Gene M → M subunit protein ┘
One-Line Summary to Write in Exam:
"Isoenzymes are formed because multiple genes code for slightly different subunit proteins, which then combine in various proportions to produce enzyme molecules with the same catalytic function but different physical properties. Their tissue-specific expression pattern gives each organ a characteristic isoenzyme profile."
Does this make it clearer? If you want, I can explain any one part (like gene expression or subunit mixing) in even simpler terms with more examples!
This is a shared conversation. Sign in to Orris to start your own chat.