I am a physical therapy student
Welcome! How can I help you today? Whether it's anatomy, biomechanics, rehabilitation techniques, clinical conditions, exercise prescription, or anything else related to physical therapy, feel free to ask!
Ulner nerve
Reading File
Searching the Web
ulnar nerve anatomy innervation physical therapy
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, PT-focused overview of the ulnar nerve, drawn from Gray's Anatomy for Students and Bradley and Daroff's Neurology in Clinical Practice.
The Ulnar Nerve - A Physical Therapy Guide
Origin & Roots
- Spinal levels: C8, T1
- Arises from the medial cord of the brachial plexus
- Travels with the median nerve and axillary artery in the proximal arm
Course Through the Upper Limb
Arm
- No branches given off in the arm
- Pierces the medial intermuscular septum at the arcade of Struthers (~8 cm proximal to the medial epicondyle)
- Passes posterior to the medial epicondyle ("funny bone") through the ulnar groove
- Enters the cubital tunnel beneath the humeral-ulnar aponeurosis (arch of flexor carpi ulnaris)
Forearm
- Passes between the two heads of flexor carpi ulnaris (FCU)
- Travels between the FCU and flexor digitorum profundus (FDP)
- Lies medial to the ulnar artery in the distal two-thirds of the forearm
- Gives off two cutaneous branches distally:
- Dorsal cutaneous branch (5-8 cm proximal to wrist): dorsal medial hand and dorsal ring/little fingers
- Palmar cutaneous branch: proximal medial palm
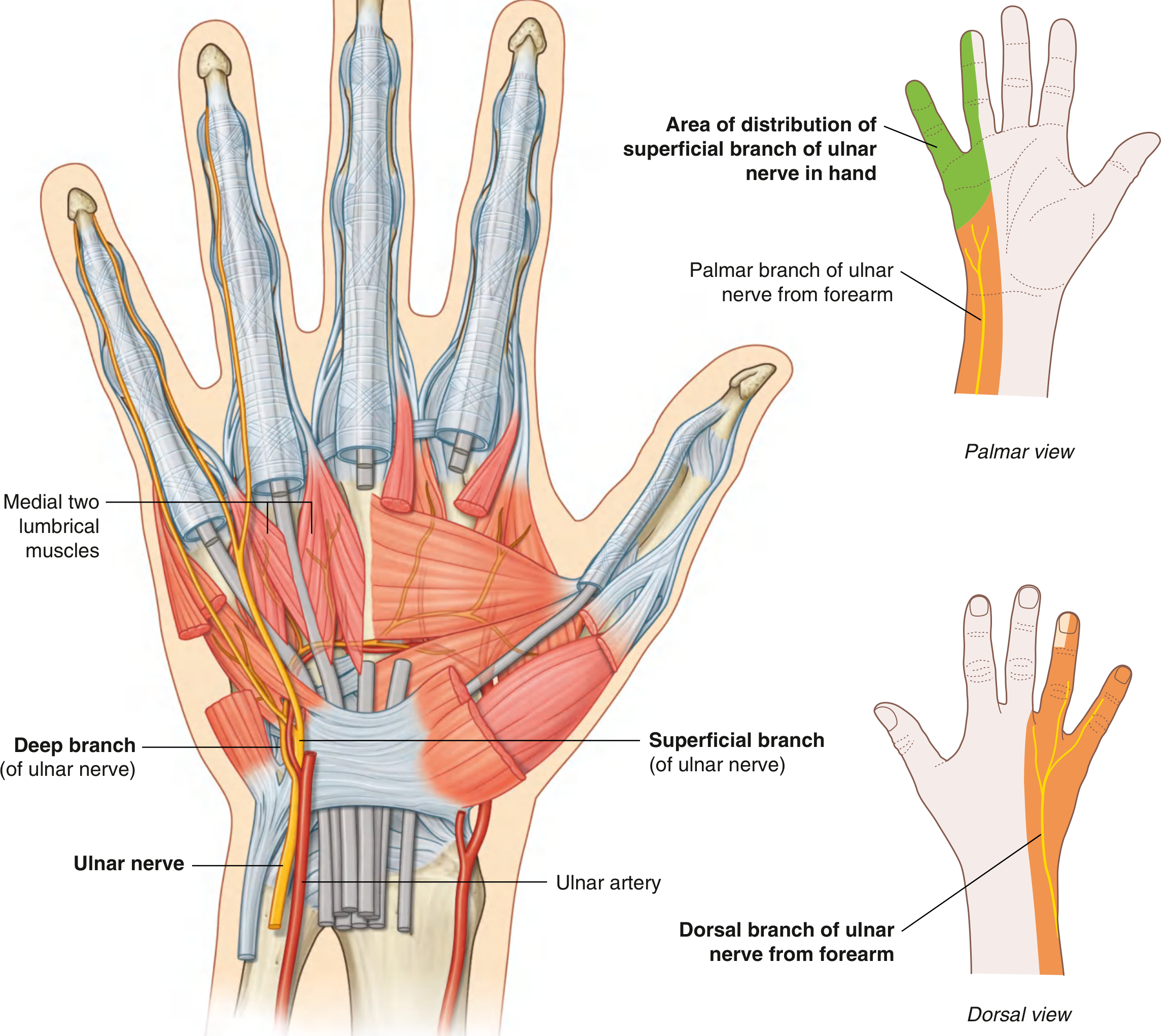
Wrist & Hand (Guyon's Canal)
- Passes superficial to the flexor retinaculum, lateral to the pisiform
- Divides in Guyon's canal into:
- Deep (motor) branch: curves around the hook of hamate, supplies hypothenar muscles, all interossei, medial two lumbricals, adductor pollicis, deep head of flexor pollicis brevis
- Superficial (sensory) branch: sensory to little finger and medial half of ring finger
Motor Innervation Summary
| Region | Muscles |
|---|---|
| Forearm | Flexor carpi ulnaris (FCU), Flexor digitorum profundus (medial half - ring & little fingers) |
| Hypothenar | Abductor digiti minimi, Flexor digiti minimi brevis, Opponens digiti minimi |
| Hand (intrinsics) | All dorsal & palmar interossei (4+4), Medial two lumbricals (ring & little), Adductor pollicis, Deep head of flexor pollicis brevis |
Sensory Innervation
- Palmar: Little finger + medial half of ring finger (palmar surface)
- Dorsal: Dorsomedial hand, dorsal little finger and medial ring finger
- Proximal medial palm: palmar cutaneous branch (not through Guyon's canal)
Common Injury Sites & Clinical Features
1. Cubital Tunnel Syndrome (most common)
- Compression at the elbow - beneath the humeral-ulnar aponeurosis / ulnar groove
- Causes: prolonged elbow flexion, leaning on elbows, post-fracture cubitus valgus ("tardy ulnar palsy")
- Symptoms: numbness/tingling in ring and little fingers, weak grip/pinch, intrinsic muscle wasting
- PT note: the dorsal cutaneous and palmar cutaneous branches are spared when compression is at Guyon's canal (wrist), which helps localize the lesion
2. Guyon's Canal Syndrome (wrist)
- Compression between pisiform and hook of hamate
- Causes: cycling (handlebar pressure), ganglion cysts, hook of hamate fracture
- Deep branch only: purely motor deficit (no sensory loss)
- Superficial branch only: purely sensory deficit
3. Elbow Fracture/Dislocation
- Acute injury with medial epicondyle fractures
Classic Clinical Sign: "Ulnar Claw Hand"
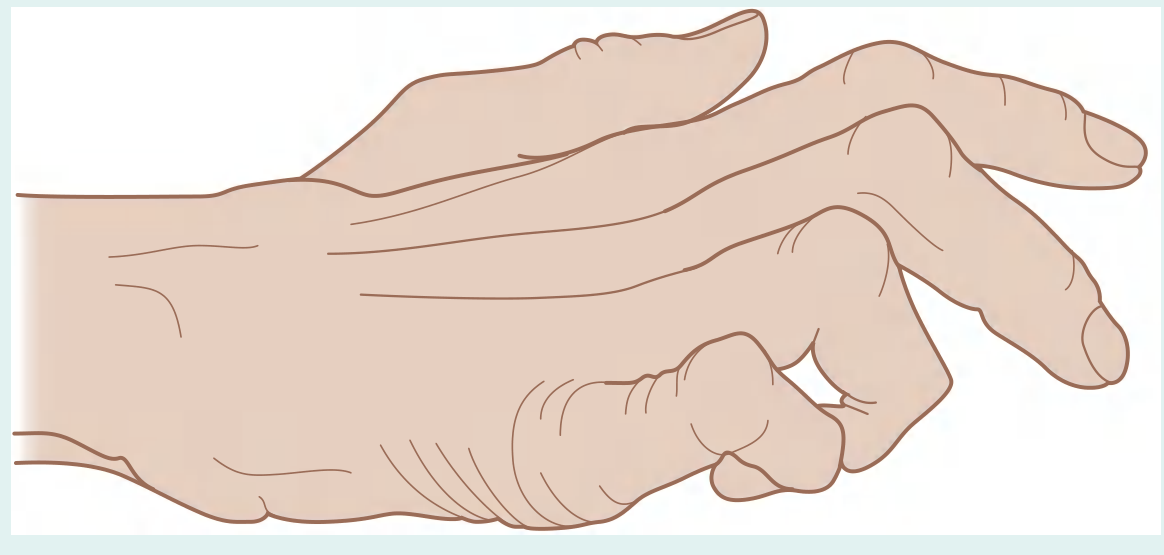
- MCPJs hyperextended + IPJs flexed in ring and little fingers
- Caused by loss of intrinsic muscles (lumbricals and interossei) with intact extrinsic flexors (FDP)
- Clawing is more pronounced at the wrist than at the elbow ("ulnar paradox") - because at the elbow, FDP to the ring/little fingers is also paralyzed, reducing the deforming force
Key PT Assessment Points
| Test | What It Checks |
|---|---|
| Froment's sign | Adductor pollicis weakness (substitute with FPL during key pinch) |
| Wartenberg's sign | Inability to adduct little finger (first dorsal interosseous/ADM weakness) |
| Card test | Interosseous weakness |
| 2-point discrimination | Sensory loss in ring/little fingers |
| Elbow flexion test | Provocative for cubital tunnel syndrome |
| Tinel's sign at elbow or wrist | Nerve irritability at compression site |
"Ulnar Paradox" - Remember This for Exams
A more proximal ulnar nerve lesion (at the elbow) produces less clawing than a distal lesion (at the wrist), because the FDP to ring/little fingers is also denervated proximally, reducing the flexion force at the IPJs.
Sources: Gray's Anatomy for Students, Bradley and Daroff's Neurology in Clinical Practice, StatPearls - Ulnar Nerve, TeachMeAnatomy
This is a shared conversation. Sign in to Orris to start your own chat.