Arthroscopic acl repair procedure
Reading File
Finding Sources
Searching the Web
arthroscopic ACL reconstruction procedure steps technique 2024
Searching PubMed
"anterior cruciate ligament" AND "arthroscopic reconstruction"
Finding Sources
Reading Web Page
https://www.hss.edu/health-library/conditions-and-treatments…
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from Campbell's Operative Orthopaedics 15th Ed 2026 plus web sources. I have enough to write a thorough, well-structured answer.
Here is a comprehensive overview of the arthroscopic ACL reconstruction procedure, based on Campbell's Operative Orthopaedics (15th Ed, 2026) and current surgical standards.
Arthroscopic ACL Reconstruction
The ACL is the most commonly reconstructed ligament in orthopaedic surgery - over 200,000 procedures are performed annually in the United States alone. The operation is performed arthroscopically as a day-case procedure under regional (epidural/adductor canal block) or general anesthesia.
Anatomy Review
The ACL is 31-35 mm long with two functional bundles:
- Anteromedial bundle (AMB) - taut in flexion, resists anterior tibial translation
- Posterolateral bundle (PLB) - taut in extension, resists rotational forces
The tibial footprint measures ~10 x 14 mm; the femoral footprint is ~8 x 15 mm ovoid, bordered anteriorly by the lateral intercondylar ridge ("resident's ridge"). Blood supply comes from the middle geniculate artery.
Graft Options
| Graft | Advantages | Disadvantages |
|---|---|---|
| Bone-Patellar Tendon-Bone (BPTB) | Bone-to-bone healing, gold standard for athletes | Anterior knee pain, donor site morbidity |
| Quadrupled Hamstring (gracilis + semitendinosus) | Less anterior knee pain, large graft volume | Risk of saphenous neuritis, slightly higher revision rate in young athletes |
| Quadriceps Tendon | Large intra-articular volume, preserved extensor strength vs BPTB | Less long-term outcome data |
| Allograft | No donor site morbidity | Higher revision rates, slower incorporation |
Step-by-Step Procedure (Endoscopic BPTB Technique)
(Based on Campbell's Operative Orthopaedics 15th Ed 2026, pp. 2757-2843)
1. Patient Positioning & Setup
- Supine position with the operative leg in a leg holder or lateral post
- Thigh tourniquet applied
- Full range of motion of the knee confirmed prior to incision
2. Graft Harvest
- A vertical midline incision over the patellar tendon
- A central-third strip of patellar tendon (10 mm wide) harvested with a 25 x 25 mm bone plug from the inferior pole of the patella and a 25 x 30 mm tibial bone plug
- A periosteal flap is raised and reflected medially to expose the proximal tibia for later tunnel placement
- Bone plugs contoured to fit a 10-mm tunnel; cancellous surfaces drilled with an 18-gauge wire for suture passage
3. Arthroscopic Examination
- Standard anteromedial and anterolateral portals created (care taken not to damage the harvested patellar tendon)
- Systematic joint inspection performed
- Associated pathology addressed - meniscal tears repaired before graft fixation
- Ligamentum mucosum released; fat pad partially resected for visualization
- ACL stump debrided with a 5.5-mm full-radius resector; the outline of tibial and femoral footprints left intact as landmarks
4. Notchplasty
- With the knee at 30° flexion, a 5.5-mm burr opens the intercondylar notch to an inverted-U shape
- Extended only 2-3 mm superiorly and laterally; not extended too far medially (would impair patellofemoral articulation)
- As notchplasty proceeds posteriorly, knee is progressively flexed from 45° to 90°
- Goal: enough space to accommodate the 10-mm endoscopic reamer without graft impingement
5. Tibial Tunnel
- An ACL tibial guide is inserted through the anteromedial portal
- Guide tip placed at the posterior edge of the ACL footprint, midway between the tibial spines and just anterior to the PCL
- Tunnel drilled at 50-55° to the tibial articular surface to the 7 o'clock position
- Guide wire followed by sequential reamers (sized to match graft diameter)
6. Femoral Tunnel (Anteromedial Portal Technique)
- Knee flexed to 110-120° to expose the posterior wall of the notch
- An accessory medial (anteromedial) portal used for the femoral reamer to achieve anatomic tunnel placement in the posterosuperior part of the ACL femoral footprint
- Tunnel depth: ~30-35 mm with a 2-mm posterior cortical wall maintained
- Femoral tunnel can alternatively be created transtibially (older technique) but anteromedial portal access achieves more anatomic positioning
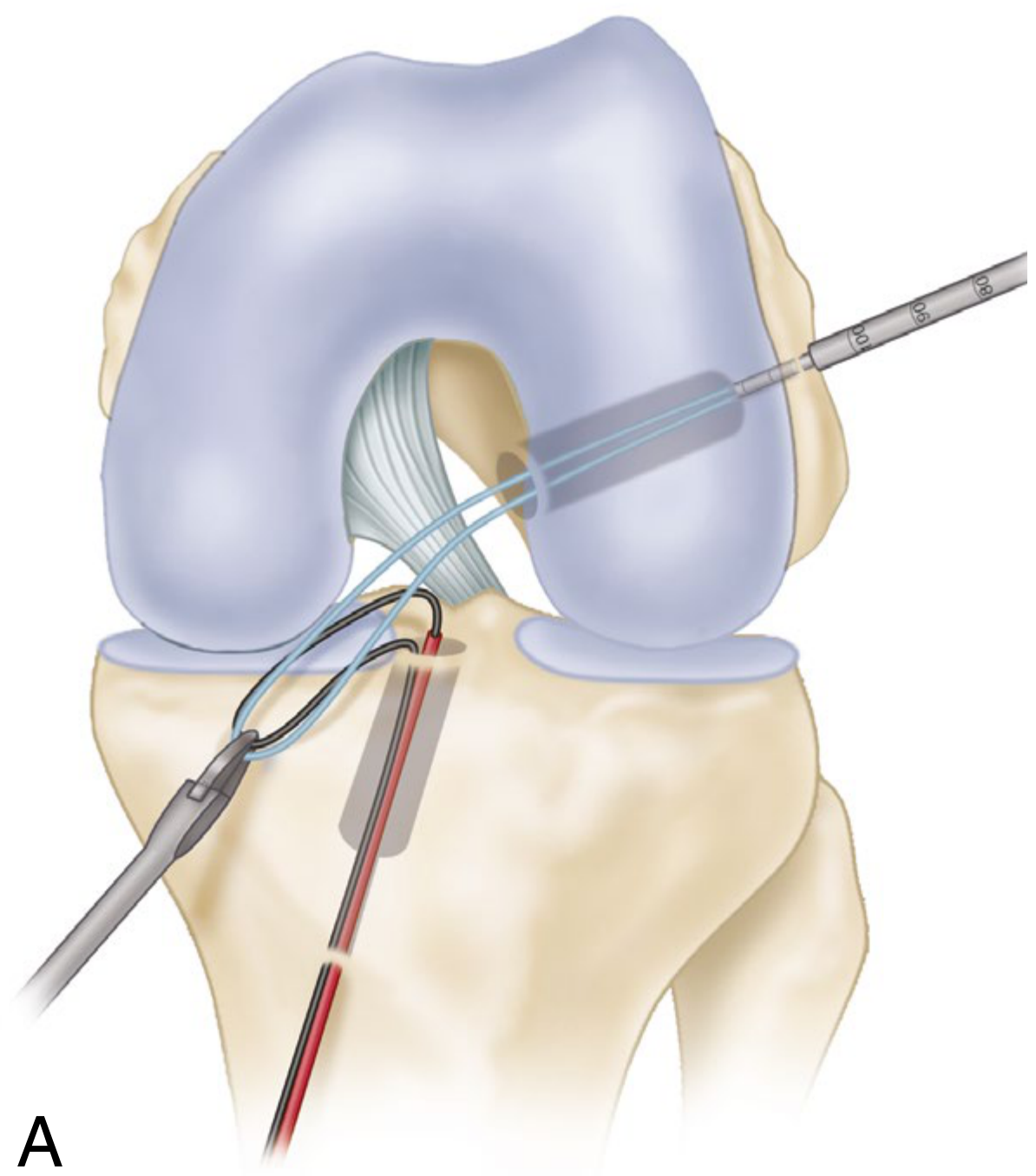
7. Graft Passage
- A passing wire or loop is threaded through the tibial tunnel, across the joint, and out through the femoral tunnel
- The bone-patellar tendon-bone graft is passed from the tibia upwards into the femoral tunnel, with the tibial bone plug cancellous surface rotated counterclockwise (right knee) so it faces laterally, replicating native ACL fiber orientation
- Graft position confirmed arthroscopically - no impingement in extension or flexion
8. Graft Fixation
- Femoral side: Interference screw (bioabsorbable or titanium) inserted alongside the bone plug; the screw diameter equals the gap size
- Tibial side: Knee brought to full extension; graft tensioned with 8-10 lb of pull for ~3 minutes while cycling the knee (allows collagen fiber stress relaxation); interference screw secured equal to gap size + 5 mm
- Overtensioning avoided - can cause joint capture or graft necrosis
9. Final Checks
- Full range of motion assessed; no graft impingement confirmed arthroscopically
- Lachman test and pivot shift performed - knee should be slightly tighter than the uninjured side
- No protruding bone or screw into the joint
10. Closure
- Patellar tendon approximated with interrupted absorbable sutures
- Bone graft placed into patellar defect; peritenon closed
- Periosteal flap replaced over tibial tunnel
- Skin closed with subdermal running Monocryl; adhesive strips, cooling sleeve, and elastic wrap applied
Hamstring Graft Modifications
When using a quadrupled hamstring graft (gracilis + semitendinosus), the technique differs at harvest:
- A 3-cm incision over the pes anserinus insertion
- Gracilis and semitendinosus tendons identified; fibrous extensions to the gastrocnemius released at 6-7 cm proximal to insertion
- Open-end tendon stripper used; tendons folded in half to form 4 strands
- Krackow whipstitch in both ends with No. 2 non-absorbable sutures
- Tibial tunnel reamed 2 mm smaller than graft diameter, then serially dilated for snug fit (dilation significantly increases pullout strength)
- Femoral fixation with an EndoButton or similar cortical suspensory device via the anteromedial portal
- Tibial fixation with an interference screw or post; backup sutures fixed to tibia with a SwiveLock
Double-Bundle Technique
Anatomic double-bundle ACL reconstruction places grafts into both the AMB and PLB footprints, more closely replicating native knee kinematics. It requires two femoral tunnels (drilled through an accessory medial portal) and two tibial tunnels. Useful in knees with rotational instability, though outcomes data vs. single-bundle remain debated.
Postoperative Protocol (Key Points)
| Phase | Timing | Goals |
|---|---|---|
| Immediate | Days 0-2 | Cold therapy, elevation, quad sets, ROM 0-90° |
| Early | Weeks 2-6 | Full weight-bearing, stationary bike, achieve full ROM |
| Strengthening | Months 2-4 | Progressive resistance, proprioception training |
| Return-to-sport | Months 9-12 | Clearance requires strength symmetry >90%, functional testing |
Complications to Know
- Graft failure / laxity - most common; failure rates ~5-10% at 5 years
- Infection - septic arthritis requiring arthroscopic debridement
- Notch impingement - inadequate notchplasty or malpositioned tunnel
- Patellofemoral pain - especially with BPTB; anterior knee pain in ~15-25%
- Saphenous neuritis - specific to hamstring harvest
- DVT/PE - risk factors include tourniquet time and immobility
- Tunnel malposition - most common technical error; leads to stiffness or re-rupture
Source: Campbell's Operative Orthopaedics, 15th Edition (2026), Chapter 50/56 - Anterior Cruciate Ligament; HSS ACL Reconstruction Guide; PMC primary ACL repair with suture tape augmentation
This is a shared conversation. Sign in to Orris to start your own chat.