What is urticaria
Reading File
Finding Sources
Searching the Web
urticaria definition types pathophysiology treatment overview
Reading File
Reading File
Searching Images
urticaria hives skin wheals
Reading File
Finding Sources
I now have comprehensive information from the textbooks and images. Here's a complete overview:
Urticaria (Hives)

Definition
Urticaria (commonly called hives) is a skin condition characterized by wheals — raised, edematous plaques with pale centers and red borders — typically accompanied by intense itching. Individual lesions are transient, usually lasting less than 24 hours, representing localized dermal edema produced by transvascular fluid extravasation. Angioedema (deeper swelling) frequently accompanies urticaria. — Rosen's Emergency Medicine, p. 2413
About 15–20% of the population experiences urticaria at some point in their lifetime.
Pathophysiology
Multiple mediators are involved, including histamine, bradykinin, kallikrein, and acetylcholine. Urticaria can be triggered by immunologic or nonimmunologic mechanisms:
- Immunologic (IgE-mediated): Allergen exposure triggers IgE-bound mast cells to degranulate, releasing histamine and other vasoactive mediators → vasodilation + increased vascular permeability → wheal formation.
- Non-immunologic: Direct mast cell degranulation by drugs (aspirin, opioids), foods (strawberries, lobster), or physical stimuli — no prior sensitization needed.
— Rosen's Emergency Medicine, p. 2413
Classification
By Duration
| Type | Duration | Notes |
|---|---|---|
| Acute | < 6 weeks | More often has identifiable trigger (40–60% of cases) |
| Chronic | > 6 weeks | Trigger identified in only 10–20%; more common in women aged 40s–50s; 50% persist ≥5 years |
By Mechanism / Type
- Allergic (IgE-mediated) — foods (seafood, tree nuts, eggs), medications (penicillin), insect stings
- Drug-induced — penicillin and aspirin are the most common triggers; aspirin's mechanism is likely non-immunologic
- Infection-related — rhinovirus, rotavirus, hepatitis, mononucleosis, coxsackievirus; occult fungal (Candida), bacterial, or parasitic infections
- Physical urticarias:
- Dermatographism — stroking skin produces wheals ("skin writing")
- Cold urticaria — triggered by cold exposure; may be associated with cryoglobulinemia or connective tissue disease
- Cholinergic urticaria — triggered by exercise, heat, or emotional stress; characteristic 1–3 mm wheals with large erythematous flares
- Solar urticaria — confined to sun-exposed areas
- Heat urticaria — rare
- Contact urticaria — foods, animal dander/saliva, topical chemicals, cosmetics
- Autoimmune (chronic spontaneous) — associated with autoantibodies against IgE or its receptor
- Urticarial vasculitis — urticaria with systemic features (arthralgias, GI symptoms), associated with immune complex deposition and complement activation
— Rosen's Emergency Medicine, p. 2413; Medscape
Clinical Features
- Raised, edematous plaques with pale centers and red (erythematous) borders
- Intense pruritus (itching)
- Individual lesions resolve within 24 hours without scarring or post-inflammatory change
- New lesions may continuously appear while old ones resolve
- May occur in isolation or as part of systemic anaphylaxis

Differential Diagnosis
Conditions that can mimic urticaria include:
- Drug eruptions
- Erythema multiforme
- Erythema marginatum
- Juvenile rheumatoid arthritis / systemic JIA
- Urticarial bullous pemphigoid
- Urticarial vasculitis
- Neutrophilic urticaria
- Papular urticaria
— Fitzpatrick's Dermatology, p. 46; Rosen's Emergency Medicine, p. 2414
Treatment
| Approach | Details |
|---|---|
| Remove trigger | Identify and eliminate the offending allergen/drug when possible |
| H1 antihistamines (1st line) | Cetirizine, loratadine, fexofenadine (non-sedating preferred); hydroxyzine for symptomatic relief |
| H2 antihistamines | Add an H2 blocker (e.g., ranitidine) for combination therapy in chronic urticaria |
| Corticosteroids | Prednisone or dexamethasone for moderate–severe urticaria; short courses (14–21 days with taper); chronic steroid use is not recommended |
| Physical urticarias | Antihistamines 30–60 min before known trigger (e.g., cold exposure); phototherapy for solar urticaria |
For severe anaphylaxis-associated urticaria, epinephrine is the priority intervention.
— Rosen's Emergency Medicine, p. 2414
Key takeaway: Urticaria is a common, mast-cell-driven skin condition producing transient itchy wheals. Acute cases usually have an identifiable trigger; chronic cases (>6 weeks) are more often autoimmune or idiopathic and require longer-term antihistamine therapy.
Sternburg cells
Finding Sources
Finding Sources
Searching the Web
Reed-Sternberg cells Hodgkin lymphoma pathology morphology
Finding Sources
Searching Images
Reed-Sternberg cell histology owl eye nucleus Hodgkin lymphoma
Reading File
Reading File
Reading File
I have everything needed for a comprehensive answer. Here it is:
Reed-Sternberg Cells
Note: You likely mean Reed-Sternberg cells (named after Dorothy Reed and Carl Sternberg) — the hallmark of Hodgkin lymphoma.
What Are They?
Reed-Sternberg (RS) cells are the neoplastic giant cells that define Hodgkin lymphoma. They are derived from germinal center B cells — proven by single-cell microdissection studies showing identical clonal immunoglobulin gene rearrangements with somatic hypermutation in every RS cell from a given case.
Despite being B-cell derived, they have lost most B-cell markers, which is one of their diagnostic peculiarities.
— Robbins & Kumar Basic Pathology, p. 418
Morphology
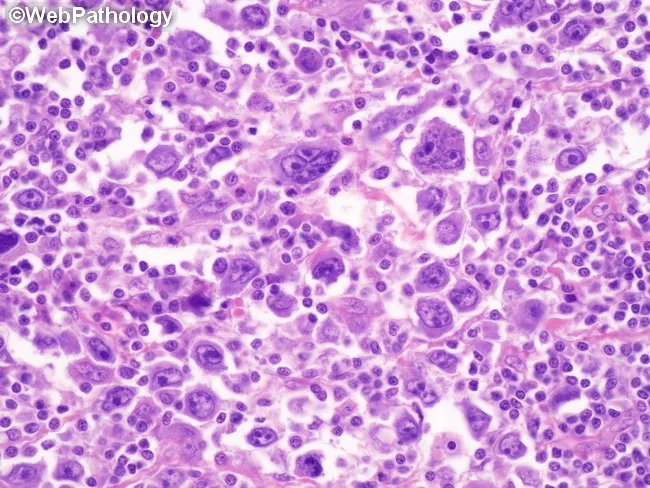
RS cells are unmistakable on light microscopy:
- Size: Very large — 15 to 45 μm in diameter
- Nucleus: Enormous multilobate nucleus, or two mirror-image nuclei/lobes
- Nucleoli: Exceptionally prominent, large, inclusion-like, acidophilic (eosinophilic), surrounded by a clear halo
- "Owl-eye" appearance — the two nuclei facing each other, each with a prominent nucleolus, resemble an owl's eyes (pathognomonic)
- Cytoplasm: Abundant, slightly eosinophilic
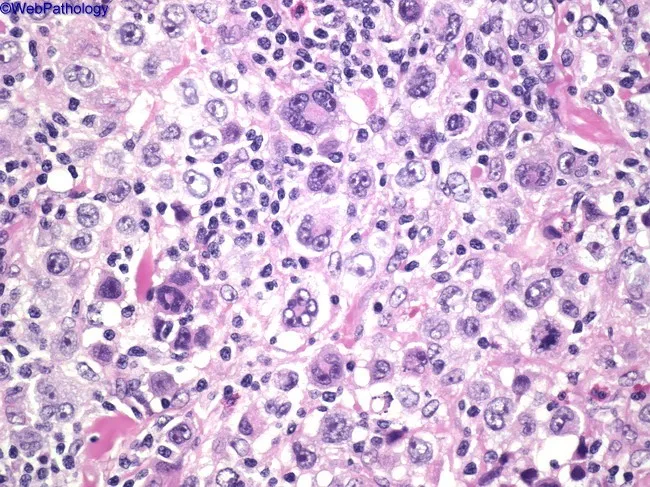
— Robbins & Kumar Basic Pathology, p. 419
Immunophenotype
| Marker | RS Cell Expression |
|---|---|
| CD15 | ✅ Positive |
| CD30 | ✅ Positive |
| CD45 (leukocyte common antigen) | ❌ Negative |
| B-cell markers (CD20, etc.) | ❌ Negative (usually) |
| T-cell markers | ❌ Negative |
| PAX5 | Weakly positive |
This unusual phenotype — CD15+, CD30+, CD45−, B-cell marker negative — is essential for diagnosis and differentiation from other lymphomas.
RS Cell Variants by Hodgkin Lymphoma Subtype
| Subtype | Variant RS Cell | Key Feature |
|---|---|---|
| Nodular sclerosis (~70%) | Lacunar cell | Single multilobed nucleus, small nucleoli, pale cytoplasm that retracts in formalin ("lacune") |
| Mixed cellularity (~25%) | Classic RS cell (plentiful) | Classic owl-eye; mixed inflammatory background with eosinophils, plasma cells, macrophages |
| Lymphocyte-rich | Classic RS cell (few) | Background of small lymphocytes |
| Lymphocyte-depleted | RS cells in sheets | Sparse background, worst prognosis |
| Nodular lymphocyte-predominant | L&H / "Popcorn cell" | Delicate multilobed nucleus; CD20+, CD15−, CD30− — biologically distinct |
Key Pathogenic Features
- EBV association: Present in RS cells in up to 70% of mixed-cellularity cases; EBV genome identical in all RS cells, indicating infection precedes clonal expansion
- Immune evasion: RS cells lose β2-microglobulin (no class I MHC expression) and overexpress PD-L1/PD-L2 — this inhibits T-cell responses. Amplification of the chromosome 9 locus encoding PD-L1/PD-L2 is common, and anti-PD-1 antibodies (e.g., pembrolizumab) are effective even in refractory disease
- Cytokine production: RS cells secrete IL-5 (attracts eosinophils), TGF-β (fibrosis), and IL-13 (autocrine growth stimulus) — explaining the characteristic inflammatory background that constitutes the bulk of the tumor mass
Clinical Relevance
- RS cells typically make up only 1–5% of the tumor mass; the rest is reactive inflammatory infiltrate
- Diagnosis requires identification of RS cells or variants in the appropriate cellular background — immunophenotyping is essential
- Hodgkin lymphoma spreads in a stepwise, contiguous fashion (unlike NHL), informing staging and radiotherapy planning
— Robbins & Kumar Basic Pathology, pp. 417–420
This is a shared conversation. Sign in to Orris to start your own chat.