Inflammatory bowel disease complete long answer for pathology mbbs exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent! I have all the comprehensive pathology content I need. Now let me compile the complete MBBS pathology exam answer on IBD.
Inflammatory Bowel Disease (IBD) - Complete Pathology Answer for MBBS Exam
Sources: Robbins & Kumar Basic Pathology, 10th ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th ed.
Definition
Inflammatory Bowel Disease (IBD) is a chronic, relapsing idiopathic inflammatory condition of the gastrointestinal tract. It encompasses two major disorders:
- Crohn Disease (CD)
- Ulcerative Colitis (UC)
Epidemiology
- IBD predominantly affects individuals in Western countries and is increasing in incidence in developing nations.
- Incidence: UC ~10-15 per 100,000; CD ~5-10 per 100,000 in Western populations.
- Peak onset: 15-30 years (second peak at 60-80 years; bimodal distribution).
- Slightly more common in females (CD) and males (UC); higher incidence in Jewish populations.
- Higher prevalence in urban populations and industrialized societies ("hygiene hypothesis").
Etiopathogenesis
IBD arises from a combination of three interacting factors: intestinal microbiota, epithelial barrier dysfunction, and aberrant mucosal immune responses, all occurring in a genetically susceptible host.
1. Genetic Factors
- IBD is a polygenic disease. Over 200 loci have been identified by GWAS.
- NOD2 gene (chromosome 16): The most strongly associated CD susceptibility gene. NOD2 encodes an intracellular receptor for bacterial cell wall muramyl dipeptide. Loss-of-function NOD2 variants impair innate immune defense against microbes, allowing bacterial invasion of the mucosa. Notably, NOD2 variants increase CD risk but are protective in UC.
- ATG16L1 and IRGM: Linked to CD; involved in autophagosome formation. Defective autophagy impairs clearance of intracellular pathogens and reactive oxygen species.
- IL-10 / IL-10 receptor genes: Mutations cause rare monogenic very-early-onset IBD (infantile colitis).
- HLA genes (especially HLA-DR2): Associated with UC.
- Many IBD risk loci overlap with those for type 1 diabetes, ankylosing spondylitis, and psoriasis.
2. Gut Microbiota (Microbial Dysbiosis)
- The normal gut microbiome is essential for maintaining immune homeostasis.
- In genetically susceptible individuals, normal commensal bacteria trigger inappropriate immune activation.
- Dysbiosis (altered microbiome composition) is consistently observed in IBD patients.
- Evidence: IBD does not occur in germ-free animals; antibiotics and probiotics can modulate disease activity.
3. Mucosal Immunity (Key Mechanism)
Both CD and UC involve mixed inflammatory responses driven by Th1 and Th17 cells (with additional Th2 in UC):
- CD: Dominated by Th1-mediated response - IFN-γ, TNF-α, IL-12 drive macrophage activation and granuloma formation.
- UC: More prominent Th2/Th17 component with IL-4, IL-5, IL-13, IL-17.
- Loss of T regulatory (Treg) cell function removes the brake on immune activation.
- TNF-α is central to pathogenesis (target of anti-TNF biologics like infliximab, adalimumab).
- Anti-IL-12/23 (ustekinumab), anti-IL-23, and JAK inhibitors are also effective, validating the immune mechanisms.
4. Epithelial Barrier Dysfunction
- Defective tight junctions increase intestinal permeability ("leaky gut").
- Reduced mucin secretion and defensin production (antimicrobial peptides from Paneth cells) in CD due to NOD2 dysfunction.
- Endoplasmic reticulum stress and unfolded protein response are implicated.
Comparison: Crohn Disease vs. Ulcerative Colitis
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Location | Any part of GI tract (mouth to anus); most common: terminal ileum + cecum | Colon only; always involves rectum |
| Distribution | Skip lesions (discontinuous) | Continuous from rectum proximally; no skip lesions |
| Depth of inflammation | Transmural | Mucosa + superficial submucosa only |
| Granulomas | Yes, noncaseating (35% of cases) | Absent |
| Fistulae/Sinuses | Common | Rare |
| Strictures | Common (fibrous, from transmural fibrosis) | Rare; when present, suspect malignancy |
| Rectal involvement | Spared in ~50% | Always involved (100%) |
| Cobblestone appearance | Yes (due to mucosal edema + longitudinal ulcers) | No |
| Toxic megacolon | Less common | More common |
| Malignancy risk | Increased (colorectal + small bowel adenocarcinoma) | Increased (colorectal adenocarcinoma) |
| Smoking | Worsens disease | Protective (paradoxically) |
| Surgery curative? | No (recurs at anastomosis ~40% in 10 years) | Yes (total colectomy is curative) |
| Fecal calprotectin sensitivity | 88% (pooled); specificity 67% | 88% (pooled); specificity 79% |
CROHN DISEASE - Detailed Pathology
Gross Morphology
- Most common sites: Terminal ileum (40% small intestine only), ileocecal region (most frequent), cecum; 30% involve both small and large intestine; colon-only disease in the remainder. Can involve esophagus and stomach (rare).
- Skip lesions: Multiple, separate, sharply delineated areas of disease interspersed with normal mucosa - hallmark distinguishing feature from UC.
- Earliest lesion: Aphthous ulcer (superficial mucosal erosion overlying a lymphoid follicle).
- Progression: Aphthous ulcers enlarge and coalesce into elongated, serpentine ("snake-like") ulcers oriented along the long axis of the bowel.
- Cobblestone appearance: Edema + mucosal ulceration creates a pattern where islands of surviving mucosa are raised, separated by crevices of ulcerated tissue, resembling cobblestones.
- Fissures: Deep linear ulcers (fissure ulcers) may extend through the full thickness of the wall to cause perforation or fistula tracts (entero-enteric, enterovesical, enterovaginal, perianal).
- Wall thickening: Bowel wall is markedly thickened and rubbery ("hose-pipe bowel") due to transmural edema, inflammation, submucosal fibrosis, and muscularis propria hypertrophy - leads to stricture formation.
- Creeping fat: Mesenteric adipose tissue wraps around the serosal surface (fat wrapping) - pathognomonic of CD.
- Lymph nodes: Mesenteric lymph nodes are enlarged; may show granulomas.
Microscopic (Histological) Features
Active phase:
- Neutrophilic infiltrate of the crypt epithelium (cryptitis) progressing to crypt abscesses (clusters of neutrophils within crypts).
- Ulceration: Abrupt transition between ulcerated and normal mucosa.
- Transmural inflammation: Lymphoid aggregates throughout all layers - mucosa, submucosa, muscularis propria, and serosa.
- Fissure ulcers: Knife-like clefts extending deep into the wall.
Chronic changes:
- Crypt architectural distortion: Crypts branch, shorten, and become haphazardly arranged due to repeated cycles of destruction and regeneration.
- Epithelial metaplasia: Gastric antral-type glands appear in small bowel (pseudopyloric metaplasia); Paneth cell metaplasia in left colon (where they are normally absent).
- Mucosal atrophy: Loss of crypts after years of disease.
- Submucosal fibrosis and muscularis propria hypertrophy.
Hallmark feature:
- Noncaseating (non-caseating) granulomas: Present in ~35% of cases. Composed of epithelioid macrophages with Langhans or foreign-body giant cells, NO central caseation (unlike tuberculosis). Can be found in any layer of the bowel wall, mesenteric lymph nodes, and even distant skin. Absence of granulomas does NOT exclude CD.
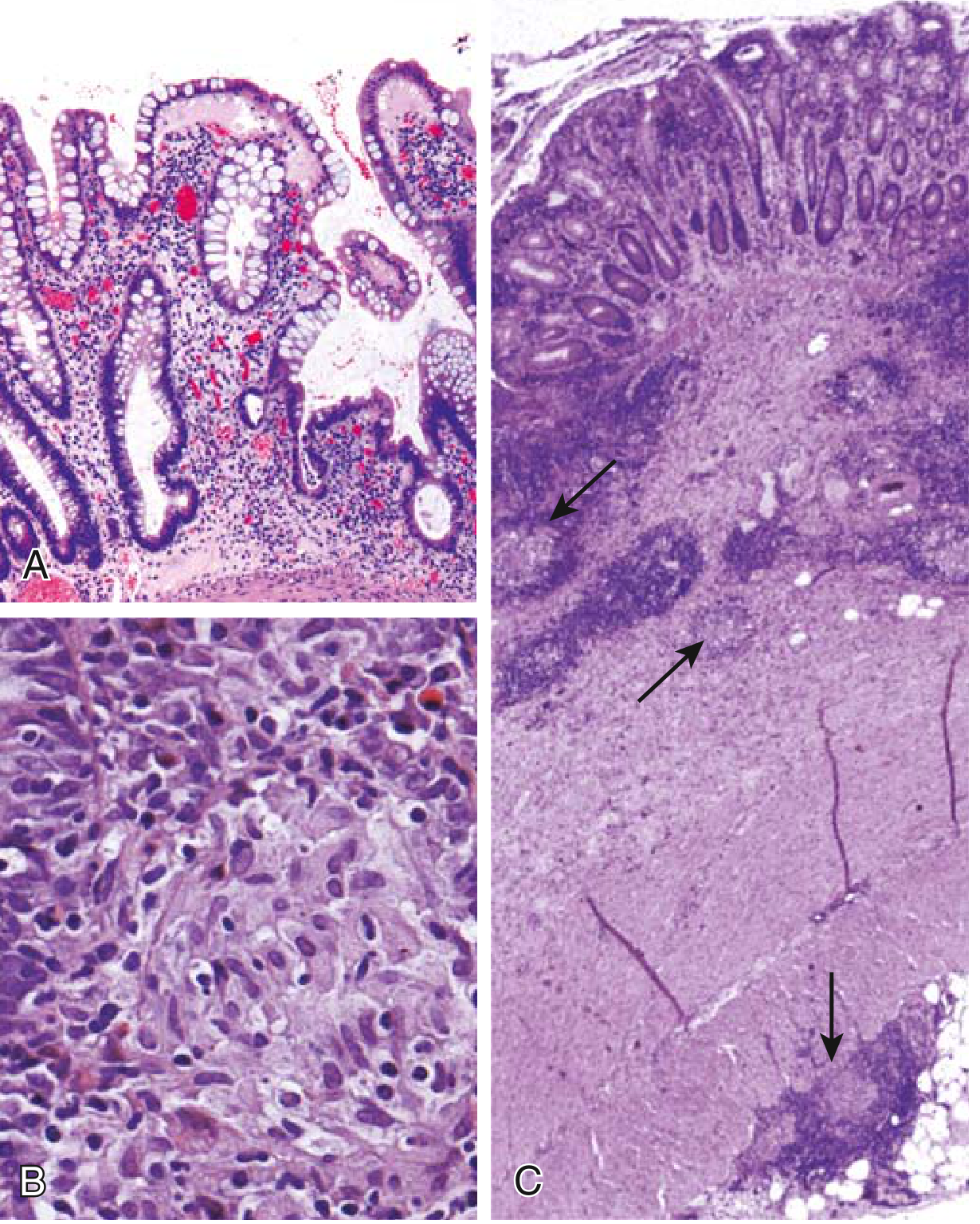
FIG. 13.29 from Robbins & Kumar Basic Pathology - Microscopic pathology of Crohn disease. (A) Haphazard crypt organization. (B) Noncaseating granuloma. (C) Transmural disease with submucosal and serosal granulomas (arrows).
ULCERATIVE COLITIS - Detailed Pathology
Gross Morphology
- Distribution: Always involves the rectum (100%) and extends proximally in a continuous (uninterrupted) fashion.
- Ulcerative proctitis: rectum only
- Left-sided colitis: up to splenic flexure
- Pancolitis: entire colon involved
- Backwash ileitis: Mild mucosal inflammation of distal ileum in severe pancolitis (does NOT represent small bowel CD).
- NO skip lesions - this is absolute.
- Mucosa appears red, granular, and friable, with broad-based ulcers aligned along the long axis.
- Abrupt transition between diseased and normal colon (vs. CD where transition is gradual).
- Pseudopolyps: Isolated islands of regenerating mucosa that bulge into the lumen, surrounded by areas of ulceration; created by repeated cycles of ulceration and healing.
- Unlike CD: no mural thickening, serosal surface is normal, no strictures, no fistulae.
- Toxic megacolon: In severe disease, inflammatory mediators damage the muscularis propria, causing colonic dilatation (>6 cm on X-ray); risk of perforation is high; clinical presentation is fever, tachycardia, hypotension.
Microscopic (Histological) Features
- Inflammation limited to mucosa and superficial submucosa - defining feature.
- Cryptitis, crypt abscesses (clusters of neutrophils in crypts), crypt distortion, epithelial metaplasia - similar to CD.
- In severe disease, ulcers may extend into submucosa, but muscularis propria is rarely involved.
- NO granulomas - their presence should prompt consideration of CD.
- Submucosal fibrosis, mucosal atrophy, and crypt architectural distortion remain as residua of healed disease.
- Histologic pattern may revert to near-normal after prolonged remission.
Clinical Features Summary
Crohn Disease
- Intermittent attacks of diarrhea (often non-bloody), colicky abdominal pain, fever, and weight loss.
- 20% present acutely mimicking appendicitis (right lower quadrant pain + fever).
- Colonic involvement: bloody diarrhea.
- Complications: Strictures, fistulae (perianal, enterovesical, enterovaginal), abscesses, malabsorption (vitamin B12 if terminal ileum involved), iron deficiency anemia, hypoalbuminemia.
- Disease recurs at anastomosis (~40% require re-resection within 10 years).
Ulcerative Colitis
- Relapsing attacks of bloody, stringy, mucoid diarrhea with lower abdominal cramps relieved by defecation.
- Attacks may persist for days to weeks.
-
50% have mild disease; almost all experience at least one relapse.
- Complications: Toxic megacolon, perforation, massive hemorrhage, colorectal carcinoma.
- Proctocolectomy is curative (unlike CD).
Extraintestinal Manifestations (Both diseases)
| System | Manifestation |
|---|---|
| Joints | Migratory polyarthritis, sacroiliitis, ankylosing spondylitis |
| Eyes | Uveitis, episcleritis |
| Skin | Erythema nodosum, pyoderma gangrenosum |
| Liver/Biliary | Primary sclerosing cholangitis (PSC - more common in UC), pericholangitis |
| Others | Clubbing (CD), thromboembolism |
Note: PSC is strongly associated with UC (70-80% of PSC patients have UC). It may precede, accompany, or follow IBD, and does NOT improve after colectomy.
Dysplasia and Cancer Risk
- Risk begins after 8-10 years of colonic IBD.
- UC with pancolitis: risk approaches ~15-18% at 30 years; risk increases ~10% per decade after the first 7-8 years of disease.
- Cancer risk correlates with extent and duration of disease; universal colitis > left-sided > proctitis.
- CD involving the colon has an increased CRC risk of 4-20x vs. general population; also increased risk of small bowel adenocarcinoma (arising in bypassed/strictured segments).
- Dysplasia is the precursor to IBD-associated carcinoma (analogous to adenoma-carcinoma sequence).
- Classified as low-grade or high-grade dysplasia.
- Crypts show "back-to-back" glands with reduced/irregular architecture.
- Nuclear changes: enlarged, hyperchromatic nuclei, increased mitoses, pseudostratification (picket-fence appearance).
- 25% of colons with high-grade dysplasia on biopsy harbor a concurrent carcinoma.
- Dysplasia is patchy - may be present in colon but absent from rectum (surveillance colonoscopy with random biopsies is required).
Investigations
| Test | Finding |
|---|---|
| Colonoscopy + biopsy | Gold standard |
| Fecal calprotectin | Sensitive marker of intestinal inflammation; pooled sensitivity 88%, specificity 73% (IBD vs. no IBD) |
| CRP / ESR | Elevated in active disease; CRP correlates with endoscopic activity in CD |
| Fecal lactoferrin | Correlates with intestinal inflammation |
| CDAI (Crohn's Disease Activity Index) | Remission <150; response = decrease ≥100 points |
| MR enterography | Mural thickening, hyperenhancement, comb sign (engorged peri-enteric vessels) in CD |
| Barium studies | String sign of Kantor (narrow terminal ileum in CD stricture) |
| pANCA | Associated with UC (~70%) |
| ASCA | Associated with CD (~60%) |
Treatment Overview (for context in pathology exam)
| Category | Agents |
|---|---|
| Aminosalicylates | Sulfasalazine, mesalazine (5-ASA) - mild UC |
| Corticosteroids | Prednisolone - acute flares |
| Immunomodulators | Azathioprine, 6-mercaptopurine, methotrexate |
| Biologics (anti-TNF) | Infliximab, adalimumab |
| Anti-integrin | Vedolizumab (anti-α4β7) |
| Anti-IL-12/23 | Ustekinumab |
| JAK inhibitors | Tofacitinib |
| Surgery | Total proctocolectomy (curative in UC); resection for complications in CD |
High-Yield Summary Table for Exam
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Entire GI tract | Yes | No (colon only) |
| Rectum spared | Yes (50%) | Never |
| Skip lesions | Yes | No |
| Transmural | Yes | No (mucosal) |
| Granulomas | Yes (35%) | No |
| Cobblestone | Yes | No |
| Creeping fat | Yes | No |
| Pseudopolyps | Less common | Common |
| Fistulae | Common | Rare |
| Strictures | Common | Rare |
| Toxic megacolon | Less common | More common |
| Surgery curative | No | Yes |
| Cancer risk | Colon + small bowel | Colon only |
| PSC association | Less | More (70-80% of PSC) |
| Smoking | Worsens | Protective |
Key Points to Remember (Exam Tips)
- CD = Cobblestone, Creeping fat, Crypt abscess, non-Caseating granulomas (all 4 Cs)
- UC = Ulcerative, Continuous, begins at reCtal end, no granUlomas (continuous mucosal disease from rectum)
- In CD, granulomas are present in only 35% - their absence does NOT rule out CD.
- PSC is more associated with UC; ankylosing spondylitis crosses both.
- Both diseases can cause crypt abscesses - this is NOT specific to either.
- Fistula formation is unique to CD (transmural disease allows this).
- IBD-associated carcinoma arises from dysplasia, not from polyps.
- CD recurs post-surgery; UC is cured by colectomy.
References: Robbins & Kumar Basic Pathology, 10th ed., pp. 578-582; Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th ed., pp. 744-756; Sleisenger and Fordtran's Gastrointestinal and Liver Disease.
This is a shared conversation. Sign in to Orris to start your own chat.