Basics of pacemaker and ppi types icd crt
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile everything.
Basics of Cardiac Implantable Electronic Devices (CIEDs): Pacemakers, ICD, and CRT
1. PACEMAKER - Basics
What It Does
A pacemaker senses intrinsic cardiac electrical activity and delivers an electrical pulse only when needed (demand pacing). It consists of:
- Pulse generator - hermetically sealed, lithium battery (~30 g, lifespan 7-12 years), semiconductor chip as CPU
- Lead system - unipolar or bipolar electrodes placed in the heart via subclavian or cephalic vein under fluoroscopy
Unipolar vs. Bipolar Leads
| Feature | Unipolar | Bipolar |
|---|---|---|
| Cathode | Lead tip electrode | Lead tip electrode |
| Anode | Generator casing | Ring electrode ~2 cm proximal to tip |
| Sensing | More prone to EMI interference | Preferred - less external interference |
| Pacing artifact on ECG | Large spike | Small spike |
The NBG (NASPE/BPEG) Pacemaker Code
Developed by the North American Society of Pacing and Electrophysiology (NASPE) and British Pacing and Electrophysiology Group (BPEG), revised in 2002:
| Position | I | II | III | IV | V |
|---|---|---|---|---|---|
| Meaning | Chamber Paced | Chamber Sensed | Response to Sensing | Rate Modulation | Antitachycardia |
| Options | O = None | O = None | O = None | O = None | O = None |
| A = Atrium | A = Atrium | I = Inhibited | R = Rate mod | P = Antitachycardia pacing | |
| V = Ventricle | V = Ventricle | T = Triggered | M = Multiple | S = Shock | |
| D = Dual | D = Dual | D = Dual | C = Communicating | D = Dual |
In daily practice, only the first 3 letters are used (e.g., VVI, DDD, AAI).
2. PACEMAKER TYPES / MODES (PPI = Permanent Pacemaker Implantation)
Common Modes
| Mode | Paces | Senses | Response | Use |
|---|---|---|---|---|
| AOO | Atrium | None | None | Asynchronous atrial - rarely used |
| VOO | Ventricle | None | None | Asynchronous ventricular - magnet mode |
| AAI | Atrium | Atrium | Inhibited | Sick sinus syndrome with intact AV node |
| VVI | Ventricle | Ventricle | Inhibited | AF with slow ventricular response; most common single-chamber |
| VDD | Ventricle | Dual | Dual | Senses atrium, paces ventricle - AV synchrony without atrial pacing |
| DDD | Dual | Dual | Dual | Most physiologic; intact sinus node, AV block |
| VVIR / DDDR | + Rate modulation | - | - | Chronotropic incompetence, active patients |
Rate Modulation (R in position IV)
Physiologic sensors (motion sensors, minute ventilation, QT interval, temperature, venous O2 sat) automatically increase/decrease pacing rate with physical activity. Key for patients who exercise.
Magnet Application
Placing a magnet over the generator closes a reed switch, converting the demand pacemaker into an asynchronous/fixed-rate pacemaker at the "magnet rate."
Indications for PPI
| Indication | Notes |
|---|---|
| Symptomatic/hemodynamically unstable bradycardia | Hypotension, altered consciousness, angina, pulmonary edema |
| Sick sinus syndrome | Prolonged asystole >3 s with syncope |
| Complete heart block | Third-degree AV block |
| Mobitz type II AV block | High risk of progression to complete block |
| Torsades de pointes | Overdrive pacing |
| Recurrent monomorphic VT | Overdrive pacing |
3. ICD (Implantable Cardioverter-Defibrillator)
Also called AICD (Automatic Implantable Cardioverter-Defibrillator).
Components
- Pulse generator - sealed titanium casing with lithium-silver-vanadium oxide battery, capacitors (charge over 3-10 sec), microprocessors, memory, telemetry
- Leads - sensing electrodes + defibrillation coil(s), inserted via subclavian/axillary/cephalic vein to RV apex (left side preferred for better shocking vector)
- Dual-coil lead - proximal coil in SVC + distal coil in RV creates 3D electric field for better defibrillation
Energy
- Capacitors store charge and discharge rapidly
- Max output: 30 J in most units; up to 45 J in higher-energy models
ICD Types
| Type | Leads | Advantage |
|---|---|---|
| Single-chamber | RV lead only | Simpler, but poor SVT discrimination |
| Dual-chamber | RA + RV leads | Better rhythm discrimination, fewer inappropriate shocks |
| CRT-D | RA + RV + LV (coronary sinus) | Combines CRT with defibrillation |
Distribution of annual ICD implants: ~27% single-chamber, ~32% dual-chamber, ~41% CRT systems.
Tiered Therapy (Hierarchical Treatment)
- Antitachycardia pacing (ATP) - overdrive pacing; terminates up to 90% of monomorphic VT <200 bpm; silent/painless
- Low-energy cardioversion (≤5 J) - if ATP fails
- High-energy defibrillation (30-45 J) - for VF or refractory VT
ICD Indications
- Secondary prevention: Survivors of VF or hemodynamically unstable VT not due to reversible cause
- Primary prevention: LVEF ≤35%, NYHA class II-III on optimal medical therapy, expected survival >1 year (ischemic cardiomyopathy ≥40 days post-MI; non-ischemic after ≥3 months of GDMT)
- Inherited channelopathies: Brugada syndrome, Long QT, HCM with high risk features
4. CRT (Cardiac Resynchronization Therapy)
Also called biventricular pacing.
What It Does
~1/3 of patients with HFrEF have QRS prolongation (often LBBB pattern), causing mechanical dyssynchrony of the failing heart. CRT paces both RV and LV simultaneously (via a coronary sinus lead for LV + RV lead), restoring coordinated contraction and improving:
- Cardiac output and LVEF
- Peak VO2 (~1-2 mL/kg/min improvement)
- NYHA functional class
- Reduction in hospitalizations and all-cause mortality
Lead Setup
- Right ventricular lead - standard endocardial lead
- Coronary sinus lead - for left ventricular pacing
- Right atrial lead - often included for AV synchrony
CRT Types
| Device | Full Name | Function |
|---|---|---|
| CRT-P | CRT-Pacemaker | Biventricular pacing only |
| CRT-D | CRT-Defibrillator | Biventricular pacing + ICD shock capability |
CRT Indications (ACC/AHA Guidelines)
Optimal condition: LVEF ≤35% + LBBB + QRS ≥150 ms + sinus rhythm + NYHA II-IV on GDMT
The CRT indications algorithm from Fuster & Hurst's The Heart, 15th Ed.:
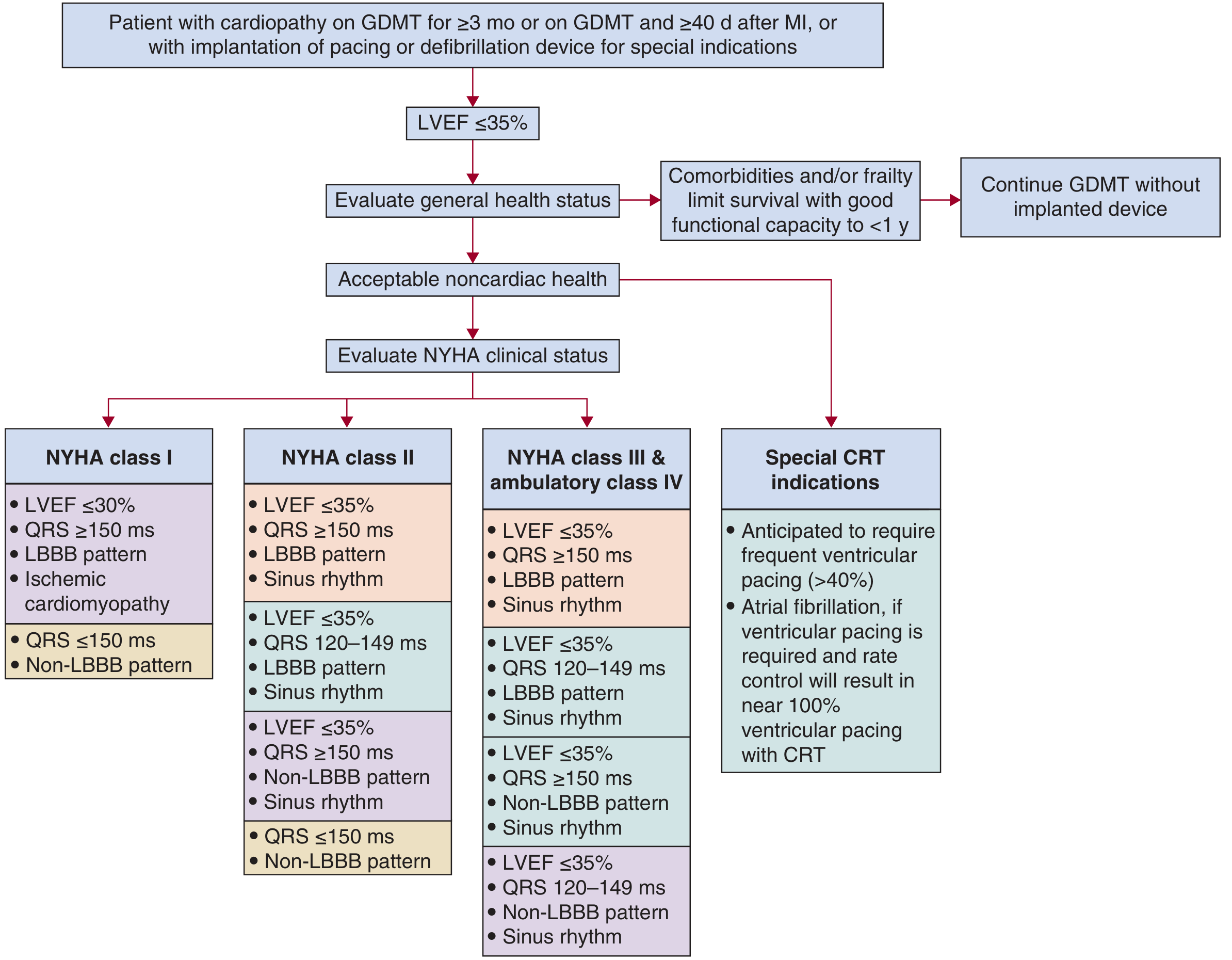
| NYHA Class | LVEF | QRS | Pattern | Indication |
|---|---|---|---|---|
| I | ≤30% | ≥150 ms | LBBB, ischemic CM | Indicated |
| II | ≤35% | ≥150 ms | LBBB, sinus rhythm | Indicated |
| II | ≤35% | 120-149 ms | LBBB, sinus rhythm | Indicated |
| III/IV (ambulatory) | ≤35% | ≥120 ms | LBBB, sinus rhythm | Indicated |
| Any | - | - | Anticipated >40% RV pacing | Special indication |
| AF with near 100% ventricular pacing required | - | - | - | Special indication (+ AV node ablation) |
Key Clinical Trials
| Trial | Population | Finding |
|---|---|---|
| COMPANION | NYHA III-IV, LVEF ≤35%, QRS ≥120 ms (n=1520) | CRT-P: 24% mortality reduction; CRT-D: 36% reduction |
| CARE-HF | NYHA III-IV, LVEF ≤35%, QRS ≥120 ms (n=813) | CRT-P: 36% mortality reduction; 52% reduction in HF hospitalization |
| MADIT-CRT | NYHA I-II, LVEF ≤30%, QRS ≥130 ms | CRT-D vs ICD: 25-35% reduction in mortality + HF hospitalization |
| RAFT | NYHA II-III, QRS ≥120 ms | CRT-D: mortality + HF hospitalization benefit; only trial showing mortality benefit in mild HF |
CRT Complications
- Coronary sinus dissection or perforation during LV lead placement
- Lead dislodgement (especially LV lead)
- Diaphragmatic/phrenic nerve pacing (from LV lateral free wall lead)
- Device pocket infection, pneumothorax, pocket erosion
Summary Comparison
| Feature | Pacemaker (PPI) | ICD | CRT |
|---|---|---|---|
| Primary purpose | Prevent bradycardia | Prevent sudden cardiac death (VT/VF) | Restore mechanical synchrony in HF |
| Leads | 1-2 (RA, RV) | 1-2 (RV ± RA) | 3 (RA + RV + LV via coronary sinus) |
| Delivers shock? | No | Yes (up to 45 J) | No (CRT-P) / Yes (CRT-D) |
| Key indication | Bradyarrhythmia, AV block, SSS | VT/VF, LVEF ≤35% + NYHA II-III | LVEF ≤35% + LBBB + QRS ≥120 ms + NYHA II-IV |
| Battery life | 7-12 years | 5-8 years | 5-9 years |
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Tintinalli's Emergency Medicine; Fuster & Hurst's The Heart, 15th Ed.; Braunwald's Heart Disease, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.