HIATUS HERNIA DEFINATION CAUSE SYMPTOMS INVESTIGATION AND TREATMENT
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
hiatus hernia types sliding paraesophageal diagram
Reading File
Loading Image
Loading Image
Searching Images
sliding hiatal hernia type I anatomy diagram
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a complete, structured overview of hiatus hernia.
Hiatus Hernia
Definition
A hiatus hernia is the herniation of abdominal organs — most commonly the stomach — through the oesophageal hiatus of the diaphragm into the mediastinum (chest). The herniated contents typically include the abdominal segment of the oesophagus with part of the stomach, though the greater omentum, colon, spleen, pancreas, and small intestine can occasionally be involved.
— Harrison's Principles of Internal Medicine 22E; Grainger & Allison's Diagnostic Radiology
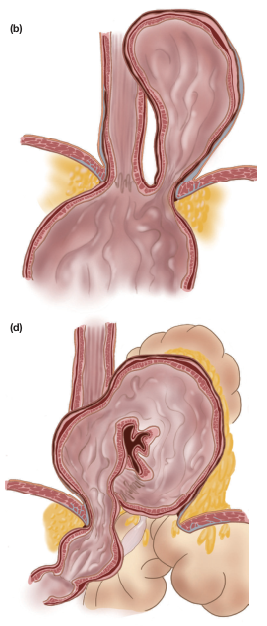
Types
There are four recognised types, broadly grouped into sliding and paraesophageal varieties:
| Type | Name | Description | Frequency |
|---|---|---|---|
| Type I | Sliding hernia | Gastro-oesophageal junction (GOJ) + gastric cardia translocate cephalad through the hiatus; GOJ is above the diaphragm | ~90–95% |
| Type II | True paraesophageal hernia | GOJ remains in normal position; gastric fundus/greater curvature herniates alongside the oesophagus | Uncommon |
| Type III | Mixed (sliding + paraesophageal) | Both the GOJ and gastric fundus herniate; "upside-down stomach" can result | Less common |
| Type IV | Complex paraesophageal | Viscera other than stomach herniate (colon, small bowel, spleen, pancreas) | Rare |
— Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine
Anatomical illustrations of hernia types (b = paraesophageal/rolling; d = mixed):
Causes and Predisposing Factors
Pathophysiology
- Weakening of the phrenoesophageal ligament/membrane — the key structural defect in sliding hernias; allows cephalad displacement of the GOJ
- Dilatation of the diaphragmatic hiatus — normally a slit-like muscular opening in the right crus; becomes more circular with atrophy of surrounding fibres in established hernias
- Increased intraabdominal pressure — chronically disrupts the hiatal apparatus
- Focal defect in the phrenoesophageal membrane — mechanism for rolling/paraesophageal hernias
Risk Factors
- Obesity (abdominal pressure)
- Pregnancy
- Chronic cough / straining (e.g., constipation, heavy lifting)
- Advancing age — incidence increases with age; a "wear and tear" phenomenon
- Hereditary/connective tissue factors — predispose to ligamentous laxity
- Congenitally enlarged oesophageal hiatus — may underlie some cases
— Harrison's Principles of Internal Medicine 22E; Grainger & Allison's Diagnostic Radiology
Symptoms
Type I (Sliding) Hernia
- Often asymptomatic — many patients have no significant symptoms
- Heartburn (pyrosis) — most common complaint; due to GERD resulting from impairment of the anti-reflux barrier
- Acid regurgitation
- Dysphagia — particularly with associated stricture or Schatzki ring
- Chest pain — can mimic cardiac pain
Type II, III, IV (Paraesophageal) Hernias
- Postprandial epigastric or chest pain
- Substernal fullness / bloating
- Shortness of breath (large hernias compress lungs)
- Nausea and vomiting
- Iron deficiency anaemia — from chronic blood loss via Cameron ulcers (linear gastric erosions at the diaphragmatic level)
- Gastric volvulus — in large hernias, can cause acute severe pain, inability to vomit, and inability to pass nasogastric tube (Borchardt's triad)
- Strangulation / obstruction — uncommon but life-threatening emergency
Although most patients with GERD have a hiatus hernia, most patients with a hiatus hernia do not have significant reflux. — Miller's Anesthesia 10e
— Goldman-Cecil Medicine; Schwartz's Principles of Surgery 11e
Investigations
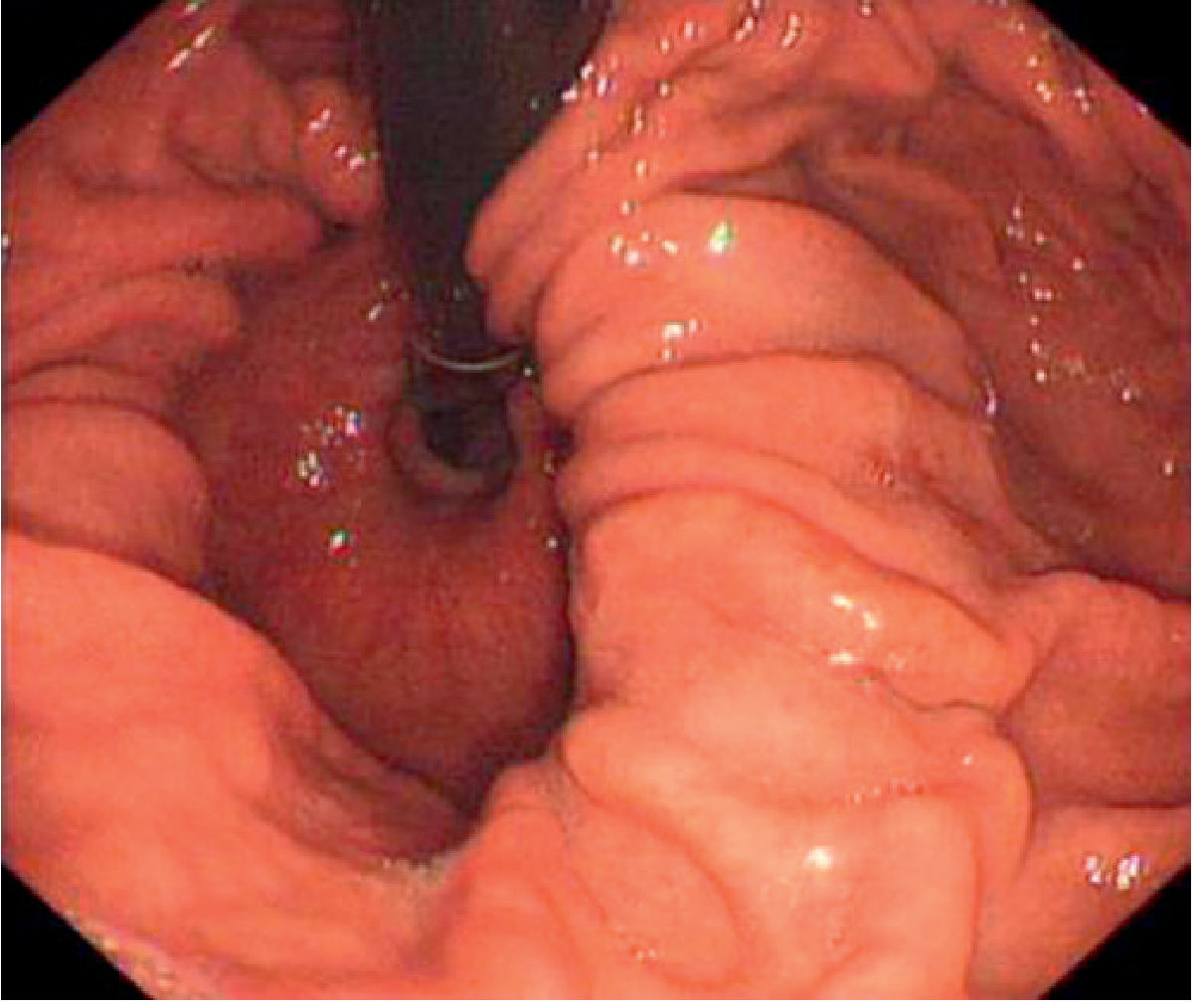
1. Endoscopy (OGD — Oesophagogastroduodenoscopy)
- Most accurate for identifying mucosal complications: reflux oesophagitis, Barrett's oesophagus, Cameron ulcers, strictures
- Diagnostic finding: gastric rugae seen passing through the diaphragmatic hiatus; or oesophageal B ring (squamocolumnar junction) visualised above the diaphragm
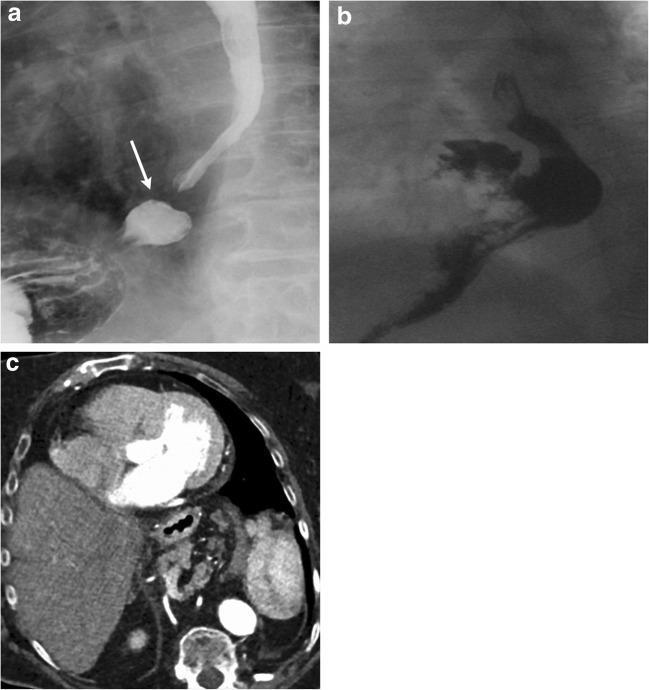
2. Barium Swallow (Fluoroscopy)
- Useful for identifying anatomy and type of hernia
- Sliding hernia confirmed when gastric rugae traverse the diaphragm or the B ring is above the diaphragm
- Less accurate for small (<2 cm) sliding hernias
- Best modality for rolling and mixed-type hernias alongside CT
- Assessment of gastric volvulus possible
3. CT Scan of the Chest/Abdomen
- Excellent for large hernias, paraesophageal hernias, and complex anatomy
- Identifies herniated contents, hernia size, and complications
- Gold standard for Type III and IV hernias
4. High-Resolution Manometry (HRM)
- Current gold standard for diagnosing small sliding hiatal hernias
- Measures lower oesophageal sphincter (LES) pressure, length, and position
- Separates LES pressure from crural diaphragm contribution
- Identifies deficient anti-reflux barrier components
5. 24-Hour Ambulatory pH Monitoring
- Gold standard for establishing the presence and degree of gastro-oesophageal reflux
- Confirms pathological acid exposure time
- Used in surgical planning
6. Chest X-Ray
- May show retrocardiac air-fluid level or air-filled viscus behind the heart in large hernias
- Incidental finding of dilated intrathoracic stomach
— Grainger & Allison's Diagnostic Radiology; Yamada's Textbook of Gastroenterology
Treatment
Conservative / Medical Management (Type I — Sliding)
Since the main clinical consequence of sliding hernias is GERD, treatment mirrors GERD management:
Lifestyle modifications:
- Weight loss (reduce abdominal pressure)
- Elevate head of bed
- Small, frequent meals; avoid meals 2–3 hours before lying down
- Avoid precipitants: alcohol, smoking, fatty foods, caffeine, chocolate, NSAIDs
Pharmacological:
- Proton pump inhibitors (PPIs) — first-line; e.g., omeprazole, lansoprazole; suppress acid secretion
- H₂-receptor antagonists — alternative or adjunct
- Antacids / alginates — for symptomatic relief of breakthrough symptoms
- Prokinetics — may help with delayed gastric emptying
Surgical Management
Indications for surgery:
- Failed or intolerable medical therapy
- Symptomatic paraesophageal hernias (Types II, III, IV)
- Complications: strangulation, obstruction, volvulus, bleeding, perforation
- Large hernias with iron deficiency anaemia
- Patient preference to stop lifelong medication
Surgical principles (anti-reflux surgery):
- Reduction of the hernia back into the abdomen
- Crural repair — closure of the diaphragmatic hiatus with permanent sutures ± mesh reinforcement
- Fundoplication — wrapping of the gastric fundus around the lower oesophagus to restore the anti-reflux barrier
Fundoplication types:
- Nissen fundoplication (360° wrap) — most common; best for normal or near-normal oesophageal motility
- Partial fundoplication (Toupet 270° posterior; Dor 180° anterior) — preferred when oesophageal dysmotility is present
Approach:
- Laparoscopic — now the standard approach; lower morbidity, shorter hospital stay, faster recovery
- Open laparotomy or thoracotomy — reserved for re-operative cases, failed laparoscopy, or complex anatomy
Mesh reinforcement of hiatus:
- Recurrence rates with primary suture closure alone: 10–40%
- Biologic or synthetic mesh reduces recurrence; biologic mesh widely used due to lower erosion risk
Post-operative consideration:
- Dysphagia is a potential complication of overly tight fundoplication
- Recurrence can occur (intrathoracic wrap migration)
— Harrison's Principles of Internal Medicine 22E; Schwartz's Principles of Surgery 11e; Miller's Anesthesia 10e; Goldman-Cecil Medicine
Key Summary Table
| Feature | Type I (Sliding) | Type II–IV (Paraesophageal) |
|---|---|---|
| Frequency | 90–95% | 5–10% |
| GOJ position | Above diaphragm | Below diaphragm (Type II) / above (Types III, IV) |
| Main symptom | Heartburn / GERD | Postprandial fullness, chest pain, anaemia |
| Main risk | Reflux oesophagitis, Barrett's | Volvulus, strangulation, obstruction |
| Treatment | Medical (PPIs) ± surgery | Surgery (usually indicated if symptomatic) |
| Surgery type | Nissen fundoplication | Hernia reduction + crural repair + fundoplication |
This is a shared conversation. Sign in to Orris to start your own chat.