Types , methods and guiding principles of sterilisation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a thorough, textbook-based answer covering sterilisation from both a microbiology/clinical perspective and a medico-legal/reproductive perspective.
Sterilisation - Types, Methods, and Guiding Principles
Definition
Sterilisation is the complete destruction or removal of all microbial forms, including the most resistant organisms such as bacterial spores, mycobacteria, non-enveloped viruses, and fungi. This distinguishes it from disinfection, which may leave some resistant forms viable.
"Sterilization: Use of physical procedures or chemical agents to destroy all microbial forms, including bacterial spores."
- Medical Microbiology 9e (Murray), Box 3.1
Types of Sterilisation
By Agent Used
- Physical sterilisation - heat, radiation, filtration
- Gas/vapour sterilisation - ethylene oxide, hydrogen peroxide vapour, plasma gas
- Chemical sterilisation - peracetic acid, glutaraldehyde
Summary Table (from Sherris & Ryan's Medical Microbiology, 8th Ed.)
| Method | Activity Level | Spectrum | Uses / Comments |
|---|---|---|---|
| Autoclave | Sterilising | All | General use |
| Boiling | High | Most pathogens, some spores | General |
| Pasteurisation | Intermediate | Vegetative bacteria | Beverages, plastic hospital equipment |
| Ethylene oxide gas | Sterilising | All | Potentially explosive; aeration required |
| Ultraviolet radiation | Sterilising | All | Poor penetration |
| Ionising radiation | Sterilising | All | General, food industry |
| Hydrogen peroxide | High | Viruses, vegetative bacteria, fungi | Contact lenses; inactivated by organic matter |
| Chlorine | High | Viruses, vegetative bacteria, fungi | Water; inactivated by organic matter |
| Glutaraldehyde | High | All | Endoscopes, equipment |
| Quaternary ammonium compounds | Low | Most bacteria/fungi, lipophilic viruses | General cleaning |
Methods of Sterilisation - In Detail
1. Heat
A. Incineration / Naked Flame
- Simplest method; used for wire loops in microbiology labs or emergency sterilisation of needle/knife blade.
- Organic material is carbonised; all microbes including spores are destroyed.
B. Dry Heat (Hot Air Oven)
- Requires 160°C for 2 hours to destroy all organisms including spores.
- If no moisture is present, 160°C is needed (versus 121°C with moist heat).
- Suitable for: metals, glassware, heat-resistant oils and waxes immiscible in water.
- Not suitable for plastics or sharp instruments.
- Damages many instruments - not currently the preferred method.
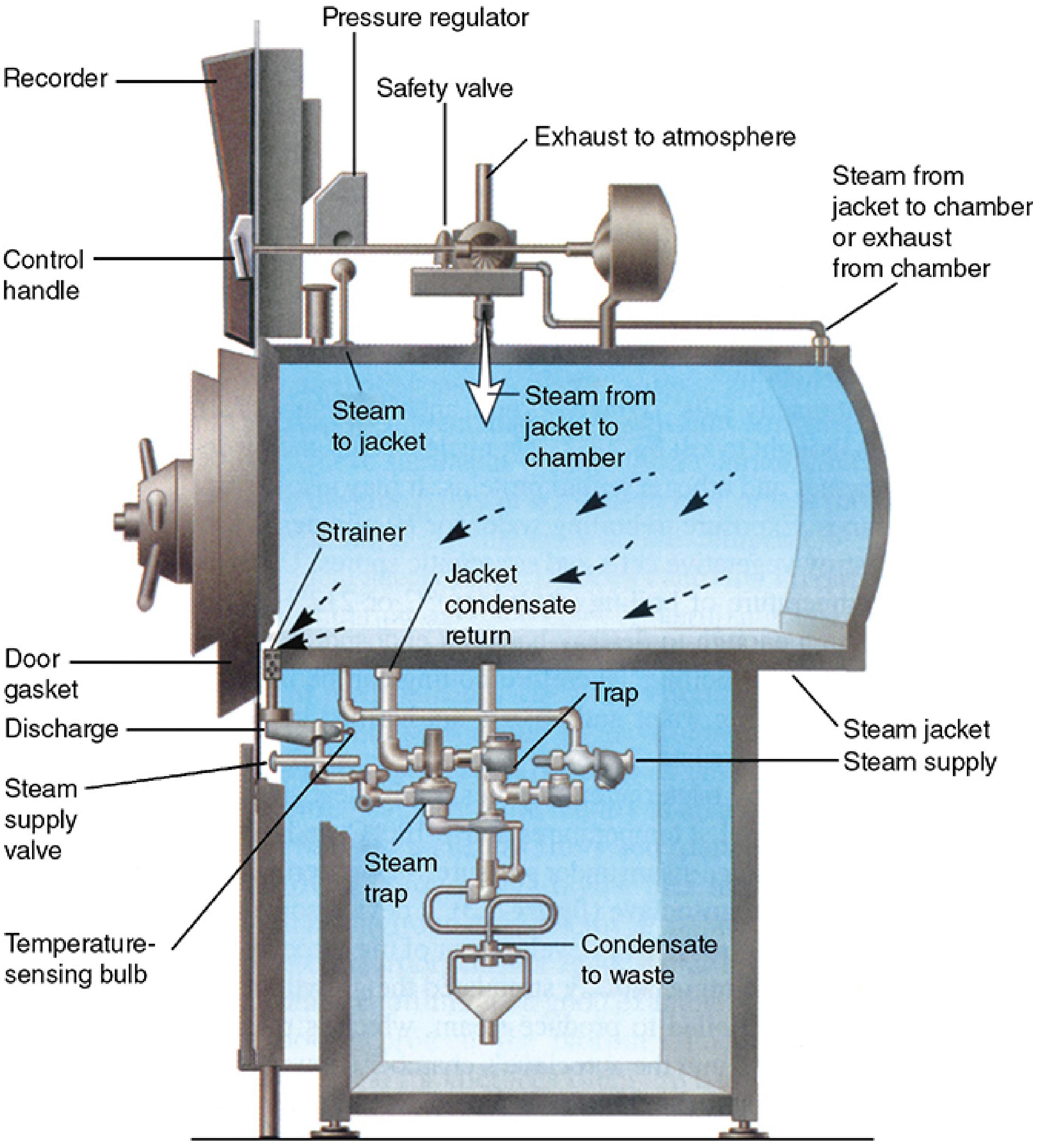
C. Moist Heat - Steam (Autoclave)
- The most widely used, inexpensive, nontoxic, and reliable method.
- Moist heat is far more effective than dry heat because reactive water molecules denature proteins irreversibly by disrupting hydrogen bonds at relatively low temperatures.
- Most vegetative bacteria are killed within minutes at 70°C or less.
Standard autoclave cycle: Saturated steam at 121°C for 15 minutes at 15 psi (103 kPa).
Three critical parameters:
- Time of exposure
- Temperature
- Amount of moisture (absence of air is essential)
A drop of just 1.7°C increases the required exposure time by 48%.
Flash autoclave (operating rooms): 134°C for 3 minutes - used for rapid availability of metal instruments.
The autoclave works as a pressurised chamber where air is replaced with pure saturated steam (either by chamber evacuation or downward displacement). Pressure itself plays no sterilising role - it merely raises steam temperature.
Suitable for: linen, dressings, gloves, syringes, instruments, culture media.
Not suitable for: plastics, sharp instruments.
D. Pasteurisation (intermediate level - not sterilisation)
- Exposure to 55-75°C to remove all vegetative bacteria.
- Spores are unaffected.
- Used for milk, fruit drinks, wine; also for plastic inhalation therapy equipment (70°C/30 min).
2. Gas / Vapour Sterilisation
A. Ethylene Oxide (EtO)
- An alkylating agent - inactivates microorganisms by replacing labile hydrogen atoms in DNA, preventing replication and transcription.
- Inflammable, potentially explosive, carcinogenic to laboratory animals.
- Used at 450-1200 mg/L at 29-65°C for 2-5 hours.
- Items must be aerated for an additional 12 hours after treatment to allow the toxic gas to diffuse out before use.
- Application: heat-labile devices such as artificial heart valves, certain plastics, lensed instruments that cannot withstand autoclaving.
- Due to toxicity and regulations, it is avoided when alternatives exist.
B. Hydrogen Peroxide Vapour
- Effective due to its oxidising nature.
- Used at 30% concentration at 55-60°C.
- Used for instrument sterilisation.
C. Plasma Gas Sterilisation
- Hydrogen peroxide is vaporised, then reactive free radicals are produced using microwave or radio-frequency energy.
- Efficient; produces no toxic by-products.
- Has replaced many ethylene oxide applications.
- Limitation: cannot be used on materials that absorb or react with hydrogen peroxide.
D. Formaldehyde Vapour
- An alkylating agent; can be used without pressure to decontaminate larger areas such as rooms.
3. Radiation
A. Ultraviolet (UV) Light
- Absorbed by nucleic acids, causing genetic damage (pyrimidine dimer formation).
- Limited practical value due to poor penetration - cannot penetrate glass, paper, or most surfaces.
- Main application: irradiation of air in critical hospital sites and biosafety cabinets.
B. Ionising Radiation (Gamma / Cathode Rays)
- Carries far greater energy than UV.
- Causes direct DNA damage and produces toxic free radicals and hydrogen peroxide from intracellular water.
- Widely used industrially for sterilising pre-packaged disposable surgical supplies: gloves, plastic syringes, specimen containers, some foodstuffs.
- Items can be packaged before exposure since radiation penetrates packaging.
4. Filtration
- Both live and dead microorganisms can be removed from liquids by positive or negative-pressure filtration.
- Membrane filters with a pore size of 0.2 μm are effective for removing bacteria from large volumes of fluid.
- Particularly useful for fluids containing heat-labile components such as serum.
- Not effective for removing viruses (too small).
- Also: HEPA filters (High-Efficiency Particulate Air) for air filtration (0.22-0.45 μm pore size).
5. Chemical Sterilants
| Chemical | Mechanism | Notes |
|---|---|---|
| Peracetic acid | Oxidising agent | Excellent activity; end-products (acetic acid + oxygen) are non-toxic |
| Glutaraldehyde | Alkylating agent | Broad spectrum including spores; safety concerns - careful handling required |
Sterilisation (Reproductive/Medico-Legal Context)
In a medical-legal sense, sterilisation refers to a procedure that renders a person permanently or temporarily infertile without affecting sexual potency.
Types (by Consent and Intent)
- Compulsory sterilisation - ordered by the State (e.g., on mental defectives, sexual criminals - eugenic perspective). Not practised in India.
- Voluntary sterilisation - performed with the informed and documented consent of both spouses.
- (A) Therapeutic - to prevent danger to health or life from future pregnancy.
- (B) Eugenic - to prevent conception of physically or mentally defective offspring; aims to improve the gene pool.
- (C) Contraceptive - for family planning/limiting family size.
Methods
Permanent methods:
- Vasectomy (male)
- Tubectomy/tubal ligation (female)
- Exposure to deep X-rays (both sexes)
Temporary methods:
- Coitus interruptus
- IUCD (loop/IUD)
- Oral hormonal pills
- Foam tablets
- Diaphragm, spermicidal jellies, condoms
Guiding Principles of Sterilisation (Medico-Legal)
To avoid legal complications, the following precautions must be observed (The Essentials of Forensic Medicine and Toxicology, 36th Ed.):
- Written consent of both wife and husband must be obtained for contraceptive sterilisation.
- Therapeutic or eugenic sterilisation is not unlawful if performed after obtaining true and valid consent.
- After vasectomy, a post-operative check is preferable. The patient should be advised to abstain from intercourse for approximately 3 months, or until seminal examination shows absence of spermatozoa on two successive occasions.
- Hormonal pills may rarely be harmful; necessary precautions must be taken to avoid complications.
Guiding Principles for Microbial Sterilisation (Clinical/Infection Control)
Key determinants of sterilisation effectiveness (Medical Microbiology 9e):
- Nature of the item to be sterilised
- Number and resilience of contaminating organisms (bioburden)
- Amount of organic material present - organic matter can inactivate chemical sterilants
- Type and concentration of sterilant
- Duration and temperature of exposure
- Cleaning must precede sterilisation - organic debris must be removed first for disinfection/sterilisation to be fully effective
Spaulding Classification (clinical application)
This guides the choice of sterilisation vs. disinfection:
- Critical items (enter sterile tissue or bloodstream - e.g., surgical instruments, implants): require sterilisation
- Semi-critical items (contact mucous membranes - e.g., endoscopes): require high-level disinfection
- Non-critical items (contact intact skin - e.g., blood pressure cuffs): require low-level disinfection
Sources: Sherris & Ryan's Medical Microbiology, 8th Ed. | Medical Microbiology 9e (Murray et al.) | The Essentials of Forensic Medicine and Toxicology, 36th Ed. | Park's Textbook of Preventive and Social Medicine
Medico legal problems and complications of artificial imsemination
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from four forensic medicine textbooks. Here is the full compiled answer.
Medico-Legal Problems and Complications of Artificial Insemination
Definition and Background
Artificial Insemination (AI) is the deposition of semen in the vagina, cervical canal, or uterus by instruments to bring about pregnancy that is not attained or is unattainable by sexual intercourse. The semen may come from:
- AIH (Artificial Insemination - Homologous/Husband): semen of the woman's own husband
- AID (Artificial Insemination - Donor/Heterologous): semen of an anonymous donor
- AIHD (Artificial Insemination - Husband + Donor): pooled semen from both, to create a technical possibility that the husband is the biological father - this is used specifically to sidestep psychological and legal issues of AID
Precautions Required Before AID (to avoid medico-legal trouble)
(Parikh's Textbook of Medical Jurisprudence)
- Written informed consent of both husband and wife is mandatory.
- The identity of donor and recipient must not be revealed to each other; the donor should not know the result of insemination.
- The donor must be below 40 years, not related to either spouse, should have children of his own, and must resemble the husband as closely as possible in race and physical characteristics.
- The donor must be in robust physical and mental health, free from hereditary or familial disease. Medical screening must exclude tuberculosis, diabetes, epilepsy, endocrine dysfunction, psychosis; must include Wassermann reaction (syphilis) and Rh grouping.
- The donor must be screened for HIV antibody initially at donation and retested after 3 months. Semen must be frozen and held until the second test result is confirmed negative (the "window period" protocol).
- The wife of the donor must also give consent for the donation.
- A female nurse must be present during the insemination procedure.
- The doctor who performs AID should not deliver the child - because he knows the true paternity and cannot enter it truthfully in the birth record without committing perjury, yet silence also creates an ethical conflict.
- A single donor's semen should not be used to produce more than 10 children - to prevent the risk of half-siblings unknowingly marrying (incest).
Legal Problems of Artificial Insemination
I. AIH - Legal Position
AIH is justifiable and unobjectionable in principle since the child is biologically the product of both spouses. However:
A child born in wedlock as a consequence of AIH does not constitute evidence of proper consummation of marriage. This is legally significant if a spouse later seeks annulment on grounds of non-consummation.
II. AID - Specific Legal Issues
AID raises far more complex legal problems because the husband is not the biological father of the child.
1. Legitimacy of the Child
- The husband is not the biological father, and strictly speaking the child is illegitimate and cannot inherit the father's property.
- The child can only acquire legitimate status through formal adoption.
- In practice in India, if parents do not disclose the AID, the child remains a "natural child" for all practical purposes.
- If a naturally conceived child is born after an AI child, the AI child remains illegitimate unless adopted, while the naturally born child is legitimate.
2. Adultery
- AID is NOT adultery under Indian law. Section 497 IPC requires sexual intercourse (coitus) as a necessary element of adultery. Since AID involves no physical union, neither the recipient (wife) nor the donor can be held guilty of adultery.
- However, without the husband's knowledge and consent, AID could morally be viewed as a form of infidelity and can serve as a ground for divorce.
- If the husband was unaware, he is almost certainly entitled to sue his wife for divorce and the practitioner for damages.
3. Nullity of Marriage and Divorce
- AI alone is not a ground for nullity of marriage or divorce, because sterility per se is not a recognised ground.
- Exception: If AID was necessitated by the husband's impotence, impotence IS a ground for nullity. The wife may then seek nullity or divorce even if a child was born through AID.
- If AID was performed without the husband's consent - he can sue his wife for divorce AND sue the doctor for damages.
4. Maintenance and Custody
- In the event of divorce, questions of maintenance and custody of an AI child raise complex issues, since the husband has no biological link.
5. Unmarried Women, Widows, and Lesbian Couples
- A child born by AI to an unmarried woman, widow, or lesbian couple is illegitimate under Indian law.
6. Succession / Property Rights
- The AI child (from AID) is not the rightful legal heir and cannot succeed to the father's property unless formally adopted.
7. Incest
- There is a real risk of incestuous relationships between offspring born by AID and the donor's own children - especially when one donor's semen is used widely without limit.
- Half-siblings have unknowingly married in documented cases internationally.
- This is why a 10-child maximum per donor rule is followed.
- In India, while the risk is acknowledged, incest arising from this circumstance is not specifically punishable.
8. Birth Records and Perjury
- The doctor performing AID who also delivers the child faces a dilemma: he knows the true paternity but cannot record it truthfully in the birth certificate without disclosing confidential information, yet recording the husband as the father could amount to falsification of records.
- To avoid this, the practitioner who performs AID should not also deliver the child.
9. Litigation for Defective Child
- There is always a risk of litigation against the doctor following the birth of a physically or mentally defective child born through AID, even if full screening was performed.
Complications of Artificial Insemination
Medical/Clinical Complications
- Transmission of sexually transmitted infections including HIV if screening protocols are not followed.
- Transmission of genetic diseases if the donor carries hereditary conditions not detected by screening.
- Possible allergic reactions to semen components.
- Risk of ovarian hyperstimulation if fertility drugs are used alongside AI.
- Multiple pregnancies if ovulation induction is used.
Psychiatric and Psychological Complications
(The Essentials of Forensic Medicine and Toxicology, 36th Ed.)
-
The husband may feel humiliation about his deficiency and the presence of another man's child in the family. If the child is mentally retarded or physically deformed, bitter feelings intensify as others may hold him responsible for the deformity.
-
The mother/wife may develop neurosis rooted in the fact that "the child belongs to her alone." She may develop an obsession to identify the donor, and a desire to have a second child from the same donor.
-
The child may suffer significant mental trauma if he/she later discovers the circumstances of his/her birth.
-
The couple together may develop psychiatric problems arising from AID - even the Parikh's textbook recommends that married couples who want a child through donor insemination should instead be urged to adopt.
Ethical Issues
- Eugenics concern: Some sperm banks select only donors with "elite" characteristics (academic achievement, physical traits). The question of whether this constitutes eugenics remains unresolved ethically.
- Commercialisation: Collection of semen from professional/paid donors without proper screening - a practice that is unfortunately common in India.
- Donor anonymity vs. child's right to know their genetic origins - an ongoing ethical debate globally.
- Sex selection: Segregation of XX/XY chromosomes for sex selection is prohibited under the Delhi AI Act and ICMR guidelines.
- Exploitation risk: In the absence of robust regulation, there is potential for exploitation of both donors and recipients.
The Delhi Artificial Insemination (Human) Act, 1995
The only statutory legislation on AI in India, applicable to the National Capital Territory of Delhi. Its main purposes:
- To allow childless couples to have a child through AI and give it legal status.
- To control the spread of HIV 1 and HIV 2 through AI.
- To regulate donation, storage, sale or supply of human semen/ovum for AI.
- Makes it obligatory for the medical practitioner to:
- Obtain written consent of husband and wife.
- Obtain written consent of donor and their spouse.
- Test for HIV 1, HIV 2, and STDs before performing AI.
- Not segregate XX/XY chromosomes (no sex selection).
- Not disclose the identity of donor or recipient.
- Maintain complete records of donor and recipient bio-data.
- Not carry on a semen bank without registration.
Note: There is no national statutory law in India on AI as a whole. The ICMR has issued guidelines but these are not legally binding. Regulation remains very weak across India outside Delhi.
Summary Table
| Issue | AIH | AID |
|---|---|---|
| Adultery | Not applicable | Not adultery under IPC S.497 (no coitus) |
| Legitimacy of child | Legitimate | Illegitimate (unless adopted) |
| Consummation of marriage | Not proved by AI | Not applicable |
| Ground for divorce | No | Yes, if done without husband's consent |
| Nullity of marriage | If impotence present | If impotence was the reason |
| Inheritance | Child inherits | Child cannot inherit |
| Incest risk | None | Yes (donor's children) |
| Doctor's liability | Low | High - especially for defective child |
Sources: Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology | P.C. Dikshit's Textbook of Forensic Medicine and Toxicology | The Essentials of Forensic Medicine and Toxicology, 36th Ed. (2026) | Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.