Intususseption
Reading File
Finding Sources
Searching PubMed
intussusception
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks and excellent images. Here is a thorough, well-illustrated overview:
Intussusception
Intussusception is the telescoping of one segment of bowel (the intussusceptum, the inner segment) into the lumen of an immediately adjacent segment (the intussuscipiens, the outer receiving segment), dragging its mesentery along with it. This causes bowel obstruction, vascular compromise, and if untreated, ischemic necrosis.
Epidemiology
- Most common cause of intestinal obstruction in infants and young children (second only to appendicitis as a cause of acute abdomen in pediatric patients)
- Peak incidence: 5-9 months; nearly all cases occur under 2 years of age, though it can occur up to school age
- In adults: rare, accounting for only ~1% of all intestinal obstruction cases
- Rosen's Emergency Medicine, p. 2044; Sleisenger & Fordtran's GI & Liver Disease, p. 2495
Types
| Type | Frequency | Notes |
|---|---|---|
| Ileocolic | >80% | Most common; ileum telescopes past the ileocaecal valve into the colon |
| Ileoileocolic | Uncommon | |
| Ileoileal | Uncommon | More common in adults |
| Colocolic | Rare | Often has a pathological lead point |
Pathophysiology & Lead Points
In children, >90% are idiopathic - caused by lymphoid hypertrophy (Peyer's patches) of the bowel wall, typically following a viral infection. This creates a "lead point" that is carried distally by peristalsis.
Pathological lead points (5-10% in children; up to 80-90% in adults):
- Meckel's diverticulum
- Intestinal polyp
- Duplication cyst
- Small bowel lymphoma
- Nasojejunal tubes
- Malignancy (adults - the dominant cause)
Key clinical rule: In adults, symptomatic intussusception is associated with a pathologic - often malignant - process in 80-90% of cases, mandating surgical exploration WITHOUT enema reduction attempts.
- Sleisenger & Fordtran's, p. 2496; Grainger & Allison's Diagnostic Radiology, p. 1805
Pathological lead points are more likely in:
- Infants <3 months or children >6-7 years
- Recurrent intussusception
Clinical Features
Classic Triad (less than 25% present with all three)
- Colicky abdominal pain - episodic, paroxysmal; the child draws up their legs and screams, then appears well between episodes
- "Currant jelly" / "redcurrant jelly" stools - blood and mucus mixed, from ischemic mucosal sloughing of the intussusceptum
- Palpable abdominal mass - sausage-shaped mass in the right upper quadrant / right side of abdomen (present in <50%)
Other Features
- Vomiting (early and bilious if obstruction develops)
- Lethargy/pallor
- Signs of dehydration and hypovolemia as disease progresses
- "Dance's sign": empty right iliac fossa due to displacement of caecum
The situation can deteriorate rapidly in infants - hypovolemia and shock can develop quickly. Prolonged symptom duration reduces the likelihood of successful non-operative reduction.
Investigations
Ultrasound - First Line (sensitivity & specificity ~100%)
Ultrasound is the modality of choice. It is diagnostic even when performed by less-experienced radiologists if properly trained.
Classic US signs:
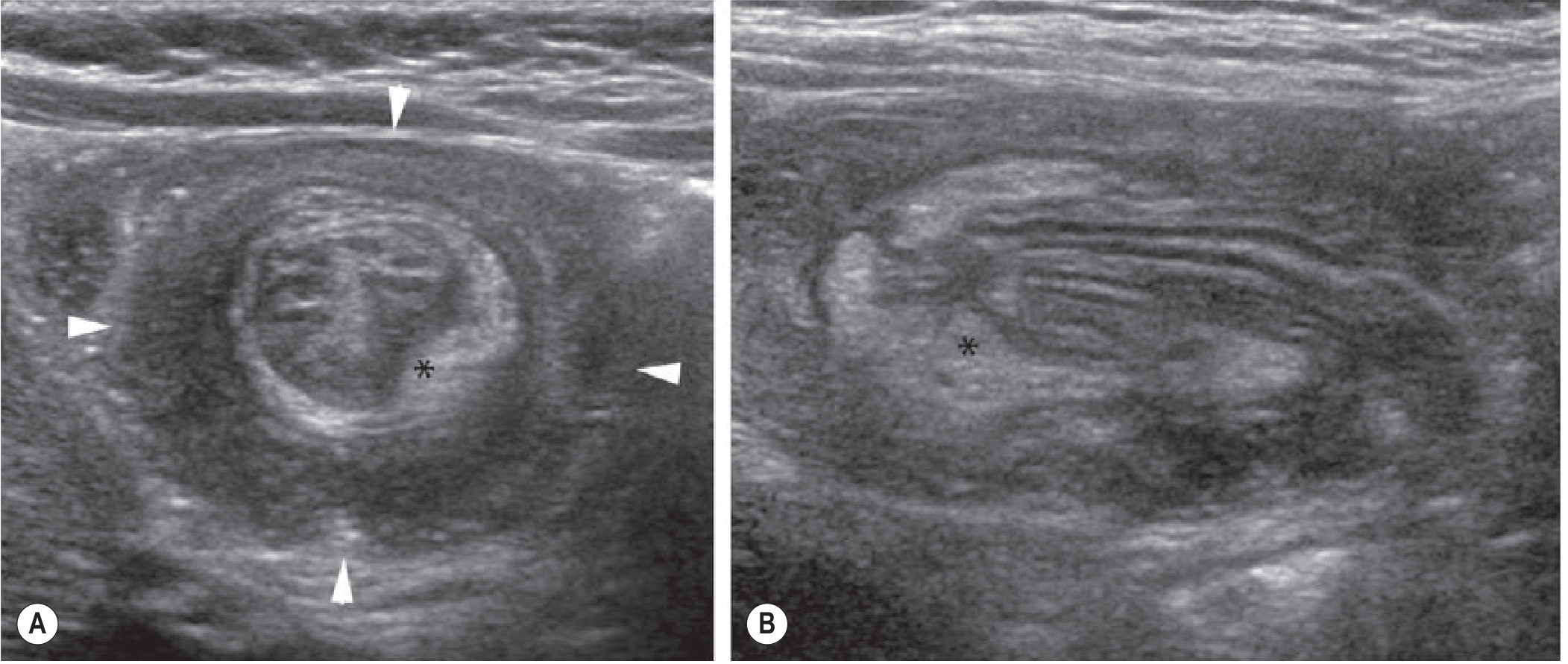
Ultrasound of intussusception (Grainger & Allison's Diagnostic Radiology). (A) Axial view showing the classic "doughnut" / "target sign" (arrowheads) - multiple layers of bowel wall, with the hyperechoic crescent of mesenteric fat () inside. (B) Longitudinal "sandwich sign" - multiple bowel wall layers with mesenteric fat ().
- Transverse plane: "target sign" or "doughnut sign" - a mass 3-5 cm in diameter with concentric rings
- Longitudinal plane: "sandwich sign"
- "Crescent in doughnut" sign: hyperechoic semilunar structure = mesenteric fat pulled into the intussusceptum - distinguishes from mimickers
- Lymph nodes and free fluid may be seen within the intussusceptum
- Use a high-frequency linear array transducer; mass is usually found just deep to the anterior abdominal wall, right of midline
Plain Radiograph (controversial; not routinely recommended)
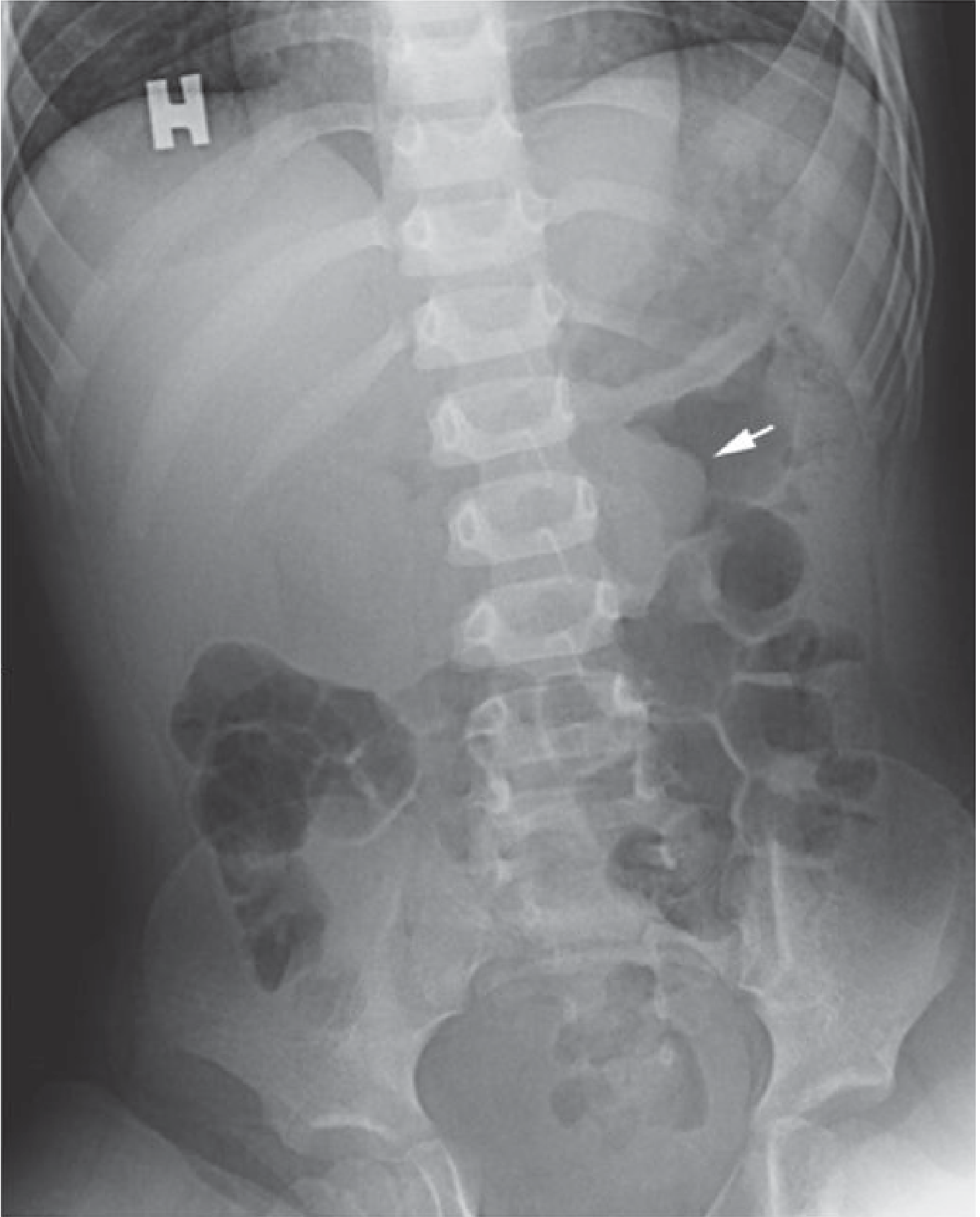
Plain abdominal X-ray (Grainger & Allison's): "Meniscus sign" (arrow) - soft-tissue mass of the intussusceptum outlined against an air-filled bowel loop.
Features on AXR:
- Soft-tissue mass contrasting an air-filled bowel loop ("meniscus sign")
- Proximal dilated gas-filled bowel loops
- Absence of gas in the caecum (suggests ileocaecal intussusception)
- Free intraperitoneal gas is extremely rare but would contraindicate enema reduction
CT Scan (adults / uncertain cases)
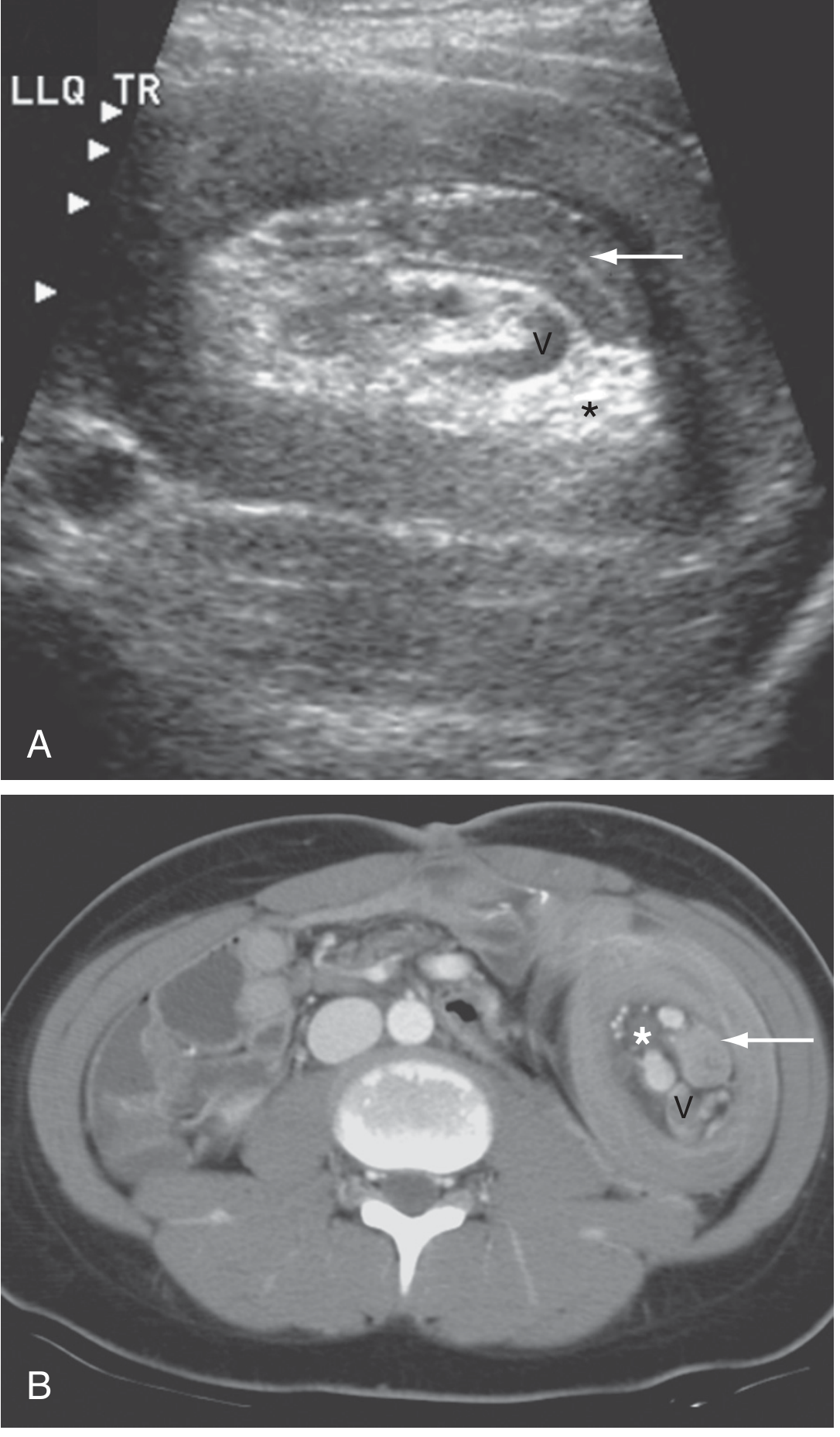
Abdominal US (A) and axial CT (B) in a patient with intussusception (Sleisenger & Fordtran's). The intussusceptum (arrow) carries mesenteric fat () and dilated mesenteric vessels (V) into the intussuscipiens.*
CT is the modality of choice in adults or when US is inconclusive. Characteristic appearance: "bowel-within-bowel" configuration.
Management
Initial Resuscitation (all patients)
- IV fluid resuscitation
- Nasogastric decompression
- Broad-spectrum antibiotics
- Analgesia
Non-operative Reduction (children - first-line)
Contraindications to enema reduction:
- Peritonitis (clinical signs)
- Free intraperitoneal air on imaging
- Hemodynamic instability / shock
Techniques:
| Method | Details |
|---|---|
| Pneumatic (air) reduction | Air enema under fluoroscopy - most widely used in UK |
| Hydrostatic reduction | Contrast or saline enema under fluoroscopy or US guidance |
- Target reduction rate: >80%
- Success is confirmed when air/contrast flows freely into small bowel AND symptoms resolve
- Sedation has been shown to increase success rate without increase in complications
- Recurrence rate: ~5% after successful non-operative reduction
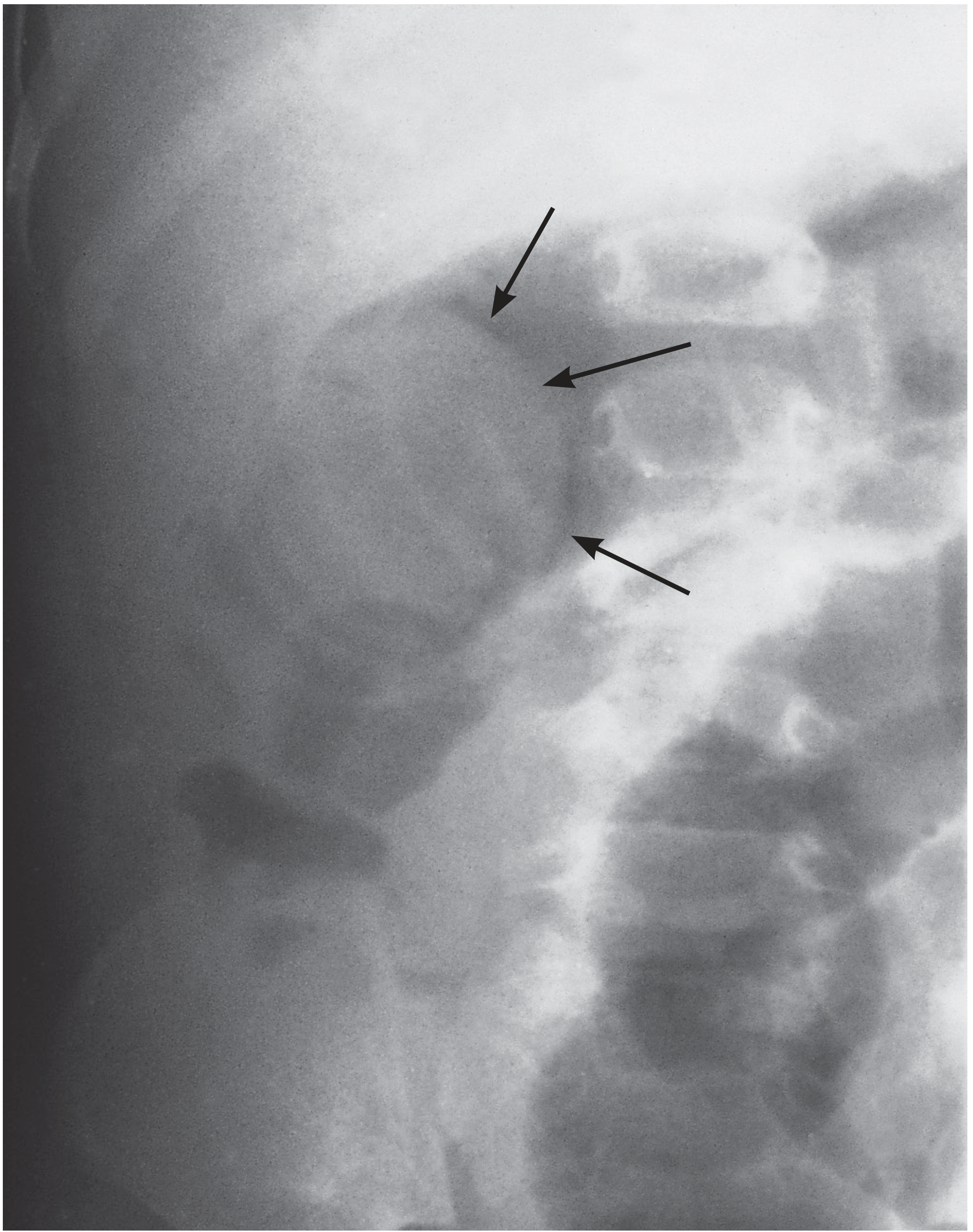
Air enema reduction of an intussusception (Bailey & Love's Surgery). Arrows mark the soft-tissue shadow of the intussusceptum being reduced.
Surgical Management (open or laparoscopic)
Indications:
- Failed non-operative reduction (>2-3 attempts)
- Perforation or peritonitis
- Clinical deterioration
- Suspected pathological lead point
- Adult intussusception (virtually always)
- Small bowel intussusception (not suited for enema)
- Strangulation / bowel infarction
Options:
- Manual reduction: squeeze the intussusceptum back through the intussuscipiens (do NOT pull from the proximal end)
- Resection and anastomosis: if reduction fails, bowel is non-viable, or a pathological lead point is present
- In adults: primary resection without attempted intraoperative reduction is the preferred approach for colonic/ileocolic intussusception, given the high malignancy rate

Operative photograph of ileocolic intussusception (Bailey & Love's Surgery).
Adult Intussusception - Special Considerations
- Accounts for <5% of all intussusception cases
- Presents subacutely - symptoms may persist days to weeks
- Often found incidentally at CT or at surgery
- 80-90% have a pathological lead point, most commonly malignant (colonic adenocarcinoma, metastases, lymphoma)
- No attempt at enema reduction - proceed to surgical resection
- Short-segment small bowel intussusception seen incidentally on thin-slice CT in asymptomatic patients is thought to be a normal, transient, physiological finding
- Sleisenger & Fordtran's GI, p. 2496; Rosen's Emergency Medicine, p. 2046
Complications
- Bowel ischemia and necrosis
- Perforation and peritonitis
- Colonic perforation during pneumatic reduction (rare)
- Hypovolemic shock
- Death if untreated
Summary Table
| Feature | Pediatric | Adult |
|---|---|---|
| Frequency | Common | Rare (<5%) |
| Lead point | Usually idiopathic (lymphoid hyperplasia) | Pathological in 80-90% |
| Most common type | Ileocolic | Small bowel or ileocolic |
| Primary imaging | Ultrasound | CT |
| First-line treatment | Pneumatic/hydrostatic enema | Surgery (resection) |
| Enema reduction | Yes (if no peritonitis/perforation) | No |
| Malignancy risk | Low | High |
Recent evidence note: Two 2024-2025 systematic reviews (PMID 39085533 and PMID 40831154) confirm that adult intussusception carries a high rate of pathological lead points and that primary surgical resection remains the standard of care, consistent with the textbook guidance above.
Sources: Sleisenger & Fordtran's GI & Liver Disease; Grainger & Allison's Diagnostic Radiology; Bailey & Love's Short Practice of Surgery (28th ed.); Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.