Operative surgery 101, surgeries, incision
Icsol
Intracranial space occupying lesion
Intracranial Space-Occupying Lesion (ICSOL)
Pathophysiology - Monroe-Kellie Doctrine
Causes (Aetiology)
| Category | Examples |
|---|---|
| Primary tumours | Glioma (GBM, astrocytoma, oligodendroglioma), meningioma, pituitary adenoma, vestibular schwannoma, medulloblastoma |
| Secondary (metastatic) | Lung, breast, melanoma, renal cell, colorectal |
| Infective | Brain abscess, subdural empyema |
| Vascular | Intracerebral hematoma, subdural hematoma, extradural hematoma |
| Other | Parasitic cysts (e.g. neurocysticercosis), arachnoid cysts, demyelinating pseudotumors |
Cerebral metastases are the most common intracranial tumours, diagnosed in ~25% of all cancer patients.
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Clinical Features - The Classic Triad
1. Raised ICP
- Headache - classically worse in the morning and on straining/coughing (high-pressure headache)
- Nausea and vomiting (especially morning vomiting)
- Blurred vision and diplopia (from VI nerve palsy - false localizing sign)
- Drowsiness progressing to coma
- Papilloedema on fundoscopy (takes time to develop, may be absent acutely)
2. Seizures
- Focal or generalized
- New-onset adult seizures demand neuroimaging to exclude ICSOL
3. Focal Neurological Deficit
| Tumour Location | Expected Deficit |
|---|---|
| Pituitary | Bitemporal hemianopia; gaze palsies |
| Cerebellopontine angle (e.g. vestibular schwannoma) | Hearing loss; tinnitus; balance problems |
| Anterior skull base (olfactory groove meningioma) | Anosmia; Foster Kennedy syndrome (ipsilateral optic atrophy + contralateral papilloedema) |
| Occipital | Homonymous hemianopia with central sparing |
| Parietal (dominant) | Gerstmann's syndrome (acalculia, agraphia, left-right disorientation, finger agnosia) |
| Temporal | Memory disturbance; superior quadrantanopia; dysphasia (dominant hemisphere) |
| Frontal | Personality change; gait disturbance; urinary incontinence |
| Posterior fossa | Ataxia; hydrocephalus |
| Brainstem | Multiple cranial nerve deficits; long tract signs; nystagmus |
Special Presentations
Investigations
Imaging
- CT head - first-line; rapidly identifies mass lesions, bleeds, oedema, hydrocephalus
- MRI - gold standard for characterizing tumours; superior for posterior fossa, brainstem, pituitary lesions
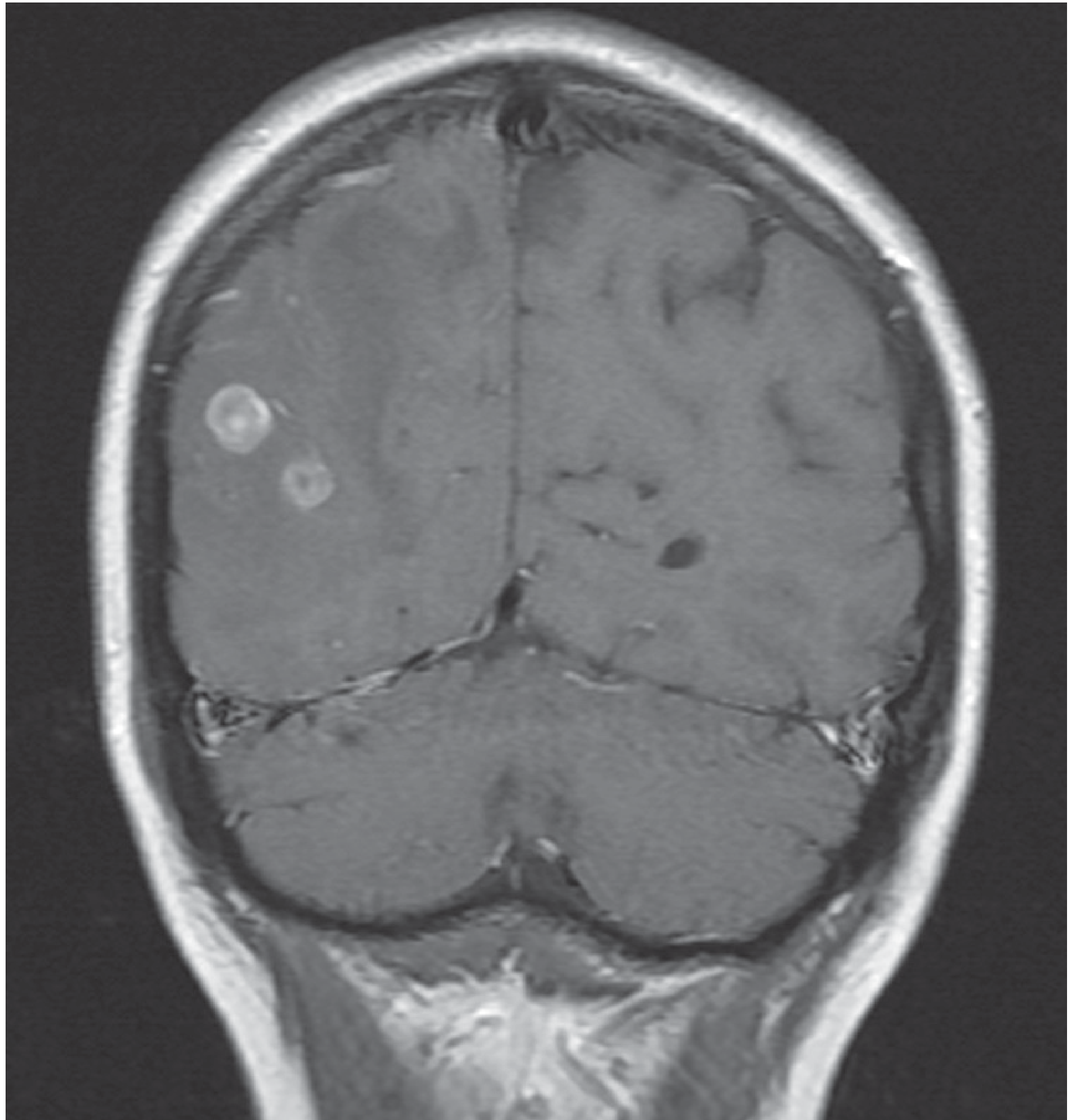
- Contrast-enhancing ring lesions = glioma or metastasis (also abscess)
- Diffusion-weighted imaging (DWI) helps distinguish abscess (restricted diffusion) from tumor
- Meningiomas show uniform dural-based contrast enhancement
- Metastases show well-demarcated, gadolinium-enhancing lesions with surrounding oedema
- ICP monitoring - gold standard is an external ventricular drain (EVD) or intraparenchymal pressure probe
- Lumbar puncture is CONTRAINDICATED until imaging has excluded an ICSOL (risk of cerebellar tonsillar herniation/"coning")
Management
Immediate / Emergency
- Raise head of bed to 30 degrees
- IV mannitol or hypertonic saline - osmotic agents to reduce cerebral oedema acutely
- Anaesthetic/neurosurgical involvement if pupil changes or declining GCS
- Urgent CT imaging
Medical
- Dexamethasone (high-dose glucocorticoid) - reduces vasogenic oedema around tumours and metastases
- Anticonvulsants for seizure control (not routinely prophylactic)
- Treat obstructive hydrocephalus with early external ventricular drainage (EVD), especially for posterior fossa tumours
Surgical
- Craniotomy + resection - for primary tumours (glioma, meningioma) and selected metastases
- Intraoperative neuronavigation for localization
- 5-ALA (5-aminolevulinic acid) given pre-op: metabolite protoporphyrin IX accumulates in glioma cells and fluoresces pink under UV, guiding complete resection
- Transsphenoidal approach (endoscopic or microscopic through the nose) for pituitary adenomas
- Stereotactic radiosurgery (e.g. Gamma Knife) for small/deep lesions or vestibular schwannomas
- Ventriculoperitoneal (VP) shunt for hydrocephalus
Adjuvant Treatment (Malignant Glioma)
- High-dose focused radiotherapy + oral temozolomide (alkylating chemotherapy)
- Median survival for glioblastoma (GBM) remains just over 12 months
Common Tumours Summary
| Tumour | Key Features |
|---|---|
| GBM (glioblastoma) | Most aggressive; ring-enhancing on MRI; WHO Grade IV; IDH-wildtype; median survival ~12 months |
| Cerebral metastases | Most common intracranial tumour overall; lung > breast > melanoma |
| Meningioma | Benign, dural-based, uniformly enhancing; watch-and-wait for small/incidental lesions; surgical excision for symptomatic/large lesions |
| Pituitary adenoma | Bitemporal hemianopia; treated transsphenoidally; pituitary apoplexy is a surgical emergency |
| Vestibular schwannoma | CPA angle; hearing loss + tinnitus; surveillance, radiosurgery or surgery depending on size |
| Medulloblastoma | Posterior fossa in children; ataxia + hydrocephalus |
Key Points for Exams
- Lumbar puncture is contraindicated in raised ICP until ICSOL excluded by imaging
- False localizing sign: unilateral or bilateral VI nerve (abducens) palsy due to raised ICP (not from a lesion at the nerve)
- New-onset seizures in an adult = ICSOL until proven otherwise
- Cushing's triad = very late sign of transtentorial herniation
- Dexamethasone is the drug of choice for perilesional vasogenic oedema
- 5-ALA fluorescence guides glioma resection margins
- Metastases + gliomas = ring-enhancing on contrast CT; meningiomas = uniformly enhancing + dural tail
Dr Rashide's questions (week 3) 1. Read about *pancreatitis* , liver segments, IBD, Colorectal CA 2. Liver pathologies (CA, abscess, hepatitis) 3. Complications of pancreatitis: Hypovolemic shock, septic SIRS, DIVC, bleeding, perforation
DR. RASHIDE'S WEEK 3 - COMPLETE STUDY GUIDE
TOPIC 1: PANCREATITIS
Acute Pancreatitis
- Acute onset severe epigastric pain, often radiating to the back
- Serum amylase or lipase ≥ 3x upper limit of normal
- Characteristic imaging findings on CT/MRI
- Serum amylase: peaks within hours, elevated 3-5 days (half-life 10 h)
- Serum lipase: more specific; elevated 8-14 days (half-life 6.9-13.7 h) - preferred marker, especially if patient presents >48 h
- Amylase can be falsely elevated in: peptic ulcer, parotitis, cholecystitis, mesenteric ischemia, renal failure
- Elevated ALT in the setting of pancreatitis = 95% PPV for biliary (gallstone) pancreatitis
- Gallstones (most common in adults, ~40%)
- Ethanol/alcohol
- Trauma
- Steroids
- Mumps / infections (viruses - coxsackievirus, EBV)
- Autoimmune / hyperCalcaemia
- Scorpion sting / hypertriglyceridemia
- Hyperlipidaemia
- ERCP (post-procedural)
- Drugs (valproate, L-asparaginase, 6-MP, prednisone)
- Epigastric tenderness with peritonism
- Cullen's sign - periumbilical bruising (retroperitoneal bleed)
- Grey Turner's sign - flank bruising (retroperitoneal bleed)
- Both are RARE but indicate haemorrhagic pancreatitis
- Tetany (from hypocalcaemia)
- USS - first-line to identify gallstones (sensitivity 95%)
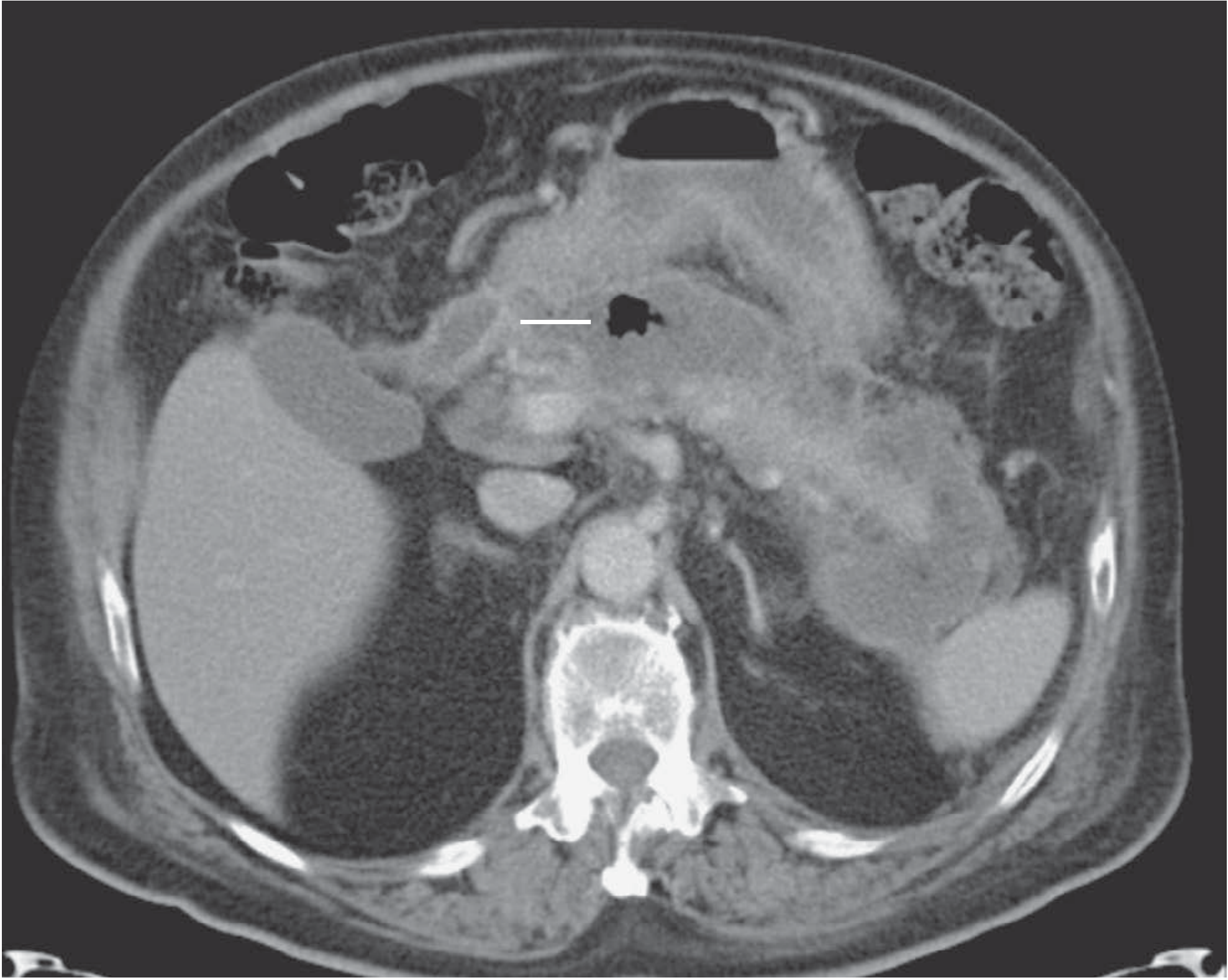
- CT (portal venous phase, 65-70s post-contrast) - gold standard for severity, necrosis, complications
- MRCP - for unexplained/recurrent cases, pancreatic duct anatomy; NOT in acute setting
- Plain AXR: non-specific - may show "sentinel loop" (isolated ileum), "cut-off colon sign"
Severity Assessment - Ranson's Criteria
| At Admission | During Initial 48 hours |
|---|---|
| Age >55 years | Haematocrit fall >10 points |
| WBC >16,000/mm³ | BUN rise >5 mg/dL |
| Blood glucose >200 mg/dL | Serum Ca²⁺ <8 mg/dL |
| Serum LDH >350 IU/L | Arterial PaO₂ <60 mmHg |
| Serum AST >250 U/dL | Base deficit >4 mEq/L |
| Fluid sequestration >6 L |
- Score ≥3 = severe acute pancreatitis
- APACHE II score ≥8 also defines severe pancreatitis
Management of Acute Pancreatitis
- IV fluid resuscitation (crystalloids) - aggressive early hydration
- Analgesia: NSAIDs (IV metamizole) or opioids (buprenorphine IV); avoid morphine (causes Sphincter of Oddi spasm)
- NBM initially; early oral feeding as tolerated
- ICU care, monitoring
- Early enteral nutrition (NG or nasojejunal) preferred over TPN
- High-dose dexamethasone or antibiotics if infected necrosis
- External ventricular drain/pancreatic drain for collections
- Early ERCP only if: coexisting cholangitis or proven biliary obstruction (hyperbilirubinaemia)
- Early laparoscopic cholecystectomy (within 3 days) for mild biliary pancreatitis = standard of care
- Peripancreatic fluid collections (early, usually resolve)
- Pancreatic pseudocyst - fluid collection encapsulated after ≥4 weeks
- Walled-off necrosis (WON) - solid debris encapsulated; needs drainage
- All drained endoscopically if in apposition to stomach/duodenum
TOPIC 2: LIVER SEGMENTS (COUINAUD)
RIGHT LOBE LEFT LOBE
Segments V, VI, VII, VIII Segments I, II, III, IV
(Caudate lobe = Segment I)
- Boundaries between segments differ from the visible anatomical right/left lobe boundary
- Left lobe = medial (segment IV) + lateral (segments II & III) parts
- Each segment has its own portal triad: branch of portal vein + hepatic artery + bile duct (= Glisson triad)
- Blood drains inward along sinusoids between hepatocytes, into the central vein → hepatic veins → IVC
- Kupffer cells (hepatic macrophages) line the sinusoidal endothelium
- Ito cells (hepatic stellate cells) in the perisinusoidal space (Disse space) - store fat; become activated in fibrosis
- Zone 1 (periportal) - first to receive oxygen; most metabolically active; first affected by toxic injury
- Zone 3 (centrilobular) - last to receive oxygen; first affected by ischaemia and in alcoholic hepatitis
TOPIC 3: INFLAMMATORY BOWEL DISEASE (IBD)
Crohn's Disease vs. Ulcerative Colitis
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Distribution | Any part of GI tract (mouth to anus); most common = terminal ileum | Colon and rectum ONLY; always involves rectum |
| Pattern | Skip lesions (patchy, discontinuous) | Continuous, no skip lesions |
| Depth | Transmural inflammation | Mucosal/submucosal only |
| Histology | Non-caseating granulomas; deep fissures | Crypt abscesses; no granulomas |
| Wall appearance | Thickened "hose-pipe" bowel; mesentery inflamed ("fat wrapping") | Thin, friable mucosa |
| Complications | Abscesses, fistulae, strictures, perforation | Toxic megacolon, colorectal CA (risk ↑ with duration) |
| Surgery | Not curative (disease recurs) | Proctocolectomy = curative |
| Cancer risk | Slight ↑ | Significant ↑ after 10 years |
Clinical Features of Crohn's Disease
- Insidious onset; chronic exacerbations and remissions
- Recurrent RIF pain (from terminal ileal involvement or ileocaecal mass)
- Diarrhoea (malabsorption of fats + bile salts)
- Weight loss; growth retardation in children
- Perianal disease: fistulae, skin tags, abscesses
- Arthritis/spondylitis (20%)
- Skin: pyoderma gangrenosum, erythema nodosum (5%)
- Iritis/uveitis (3%)
- Cholangitis/liver involvement
- Colonoscopy + biopsy - granulomas are diagnostic
- Small bowel MRI or contrast study - "cobblestone" pattern, rose-thorn ulcers, strictures
- Sulphasalazine (5-ASA) - maintenance
- Corticosteroids - acute flares
- Azathioprine / 6-MP - immunomodulator
- Anti-TNF (infliximab, adalimumab) - severe/refractory
- Surgery: resection of complicated segments (not curative; recurs)
TOPIC 4: COLORECTAL CARCINOMA (CRC)
Epidemiology
- Greatest cause of cancer mortality in non-smokers in the West
- Incidence increases with age
- Risk factors: high red meat / low fibre diet; IBD; hereditary syndromes
- ~10% hereditary - Familial Adenomatous Polyposis (FAP), HNPCC (Lynch syndrome)
Pathogenesis - Adenoma-Carcinoma Sequence
- FAP: hundreds/thousands of polyps; near 100% malignant transformation → prophylactic colectomy
Staging - Dukes' Classification
| Stage | Description | 5-Year Survival |
|---|---|---|
| A | Tumour confined to mucosa | ~95% |
| B | Tumour invades muscle wall | ~68% |
| C | Lymph node metastases | ~34% |
| D | Distant metastases | <10% |
Modern staging also uses TNM (T1-T4, N0-N2, M0-M1)
Clinical Features
- Change in bowel habit (most common)
- Rectal bleeding (distal lesions)
- Iron deficiency anaemia (occult bleeding from proximal/caecal tumours)
- Weight loss
- Palpable abdominal mass
- 50% are in sigmoid colon or rectum
- Complications: obstruction, perforation, fistula, bleeding
Treatment
- Surgical resection is primary - right hemicolectomy, left hemicolectomy, anterior resection, abdominoperineal resection (APR) for low rectal
- Adjuvant chemotherapy (FOLFOX - oxaliplatin + 5-FU) for stage III/IV
- Radiotherapy for rectal cancer (neoadjuvant to downsize)
- Surveillance colonoscopy post-op
TOPIC 5: LIVER PATHOLOGIES
A. Hepatocellular Carcinoma (HCC)
- Cirrhosis from ANY cause (alcohol, NAFLD, viral hepatitis)
- Hepatitis B - can cause HCC WITHOUT cirrhosis
- Hepatitis C - HCC develops after long-standing cirrhosis
- Aflatoxin exposure
- Fibrolamellar HCC variant - younger patients, no underlying cirrhosis
- CT/MRI: arterial hyperenhancement + portal venous washout = diagnostic in chronic liver disease
- LI-RADS 5 = diagnostic of HCC (no biopsy needed in most cases)
- Tumour marker: AFP (alpha-fetoprotein) - elevated in HCC
- Staging: BCLC (Barcelona Clinic Liver Cancer) staging system used clinically
- Liver transplantation - treatment of choice in cirrhosis + limited HCC (Milan criteria)
- Surgical resection - for Child-Pugh A patients without portal hypertension; perioperative mortality <5%
- Thermal ablation - for small HCC (<2-3 cm); equivalent outcomes to resection in small tumours
- TACE (transarterial chemoembolisation) - for intermediate HCC
- Sorafenib / Atezolizumab + bevacizumab - systemic therapy for advanced HCC
B. Liver Abscess
- Incidence: ~1/5000 hospital admissions
- Organisms: Klebsiella, E. coli, Streptococcus milleri group (usually polymicrobial)
- Routes of infection:
- Biliary tract pathology - most common (35%)
- Portal spread (from appendicitis, diverticulitis) - 20%
- Contiguous spread, bacteraemia, cryptogenic (10%)
- Increased risk: elderly, diabetics, immunosuppressed
- Fever, anorexia, malaise, right upper quadrant pain/discomfort
- Raised WCC, elevated LFTs, CRP
- USS / CT - multiloculated cystic mass with rim enhancement and possible air-fluid level
- Aspiration for culture and sensitivity
- Aspiration + antibiotics (metronidazole + cephalosporin or aminoglycoside + metronidazole for anaerobic/Gram-negative cover)
- Percutaneous drainage for large/complex abscesses
- Surgery rarely required
C. Viral Hepatitis
| Feature | Hep A | Hep B | Hep C | Hep D | Hep E |
|---|---|---|---|---|---|
| Transmission | Faeco-oral | Blood/sexual/vertical | Blood | Blood (needs HBV) | Faeco-oral |
| Chronic disease | No | Yes (10% adults, 90% neonates) | Yes (80%) | Yes | No (except in pregnancy) |
| Cirrhosis/HCC | No | Yes | Yes | Yes | No |
| Vaccine available | Yes | Yes | No | (HBV vaccine protects) | Yes (some countries) |
| Key test | Anti-HAV IgM | HBsAg, HBeAg, anti-HBc | Anti-HCV + HCV RNA PCR | Anti-HDV | Anti-HEV IgM |
| Treatment | Supportive | Tenofovir/Entecavir | DAA (Sofosbuvir-based) | Interferon | Supportive |
TOPIC 6: COMPLICATIONS OF PANCREATITIS
A. Hypovolaemic Shock
- Plasma leaks into the retroperitoneal and peritoneal spaces
- Vomiting adds to volume loss
- Haemoconcentration occurs → raised Hct and BUN (Ranson criteria items)
- Reduced circulating volume → decreased preload → reduced cardiac output → shock
B. Septic SIRS (Systemic Inflammatory Response Syndrome)
- Temperature >38°C or <36°C
- Tachycardia >90/min OR tachypnoea >20/min
- WBC >12 × 10⁹/L or <4 × 10⁹/L
C. DIC (Disseminated Intravascular Coagulation)
- Bleeding - from factor/platelet consumption and FDPs
- Thrombosis - fibrin deposition in microvessels → ischaemia of kidneys, brain, skin
| Test | DIC result |
|---|---|
| Platelet count | ↓ (consumed) |
| PT/INR | ↑ (prolonged) |
| APTT | ↑ |
| Fibrinogen | ↓ (consumed) |
| D-dimers / FDPs | ↑↑ |
| Blood film | Microangiopathic haemolytic anaemia (schistocytes) |
- Treat underlying cause (the most important step)
- If active bleeding: FFP (fresh frozen plasma) + cryoprecipitate (fibrinogen) + platelet transfusion
- If thrombosis predominates: heparin (selected cases - purpura fulminans)
- Goal: stop depletion of clotting factors; monitor fibrinogen, platelet count, and FDPs
D. GI Bleeding in Pancreatitis
- Stress ulceration of the gastric/duodenal mucosa (from splanchnic ischaemia)
- Splenic artery pseudoaneurysm - pancreatic enzymes erode the splenic artery → life-threatening haemorrhage
- Haemosuccus pancreaticus - bleeding into the pancreatic duct → haematemesis or melaena
- Portal hypertension from splenic vein thrombosis → gastric varices (left-sided/sinistral portal hypertension)
- Resuscitate with blood products
- OGD for stress ulcer bleeding; proton pump inhibitors
- Angiography + embolisation for pseudoaneurysm
- Surgery if embolisation fails
E. Perforation in Pancreatitis
- Usually involves the colon (transverse colon most common - "colonic necrosis")
- Mechanism: peripancreatic inflammation and necrosis extends to involve the mesocolon and bowel wall
- Can also cause duodenal perforation or small bowel necrosis
- Presents with: peritonitis, free air on AXR/CT, sudden deterioration
- Management: Emergency laparotomy; resection of perforated segment; defunctioning stoma; drain necrosum
QUICK SUMMARY TABLE
| Topic | Key Fact |
|---|---|
| Acute pancreatitis | Ranson ≥3 = severe; lipase more specific than amylase |
| Liver segments | 8 Couinaud segments based on portal/hepatic vascular distribution |
| Crohn's | Transmural; skip lesions; any GI segment; granulomas |
| UC | Mucosal only; continuous from rectum; no granulomas; curative surgery |
| Colorectal CA | Dukes' A=95%, B=68%, C=34%, D<10% survival |
| HCC | Arterial enhancement + portal washout on CT; BCLC staging; transplant if cirrhotic |
| Liver abscess | Biliary origin 35%; Klebsiella/E. coli; aspirate + antibiotics |
| SIRS | ≥2 of: temp, HR/RR, WBC criteria |
| DIC | Simultaneous clotting + bleeding; ↓fibrinogen, ↑FDPs, ↓platelets; treat cause first |
| Pancreatitis-GI bleed | Pseudoaneurysm = life-threatening; stress ulcers common |
Acute pancreatic 101
ACUTE PANCREATITIS - COMPLETE GUIDE
OVERVIEW
- 80-90% = mild, self-limiting
- 10-20% = severe, with systemic complications and MODS
- Mortality: mild <1% | severe 10-50%
- Death is bimodal: early (first 2 weeks) from MODS; late (after 2 weeks) from septic complications
PATHOPHYSIOLOGY
Step-by-Step Mechanism
Precipitating cause (gallstone / alcohol / etc.)
↓
Zymogen granules + lysosomes COLOCALIZE inside acinar cells
↓
Lysosomal cathepsin B activates trypsinogen → TRYPSIN
↓
Trypsin activates other proenzymes:
- Elastase → blood vessel digestion → haemorrhage
- Phospholipase A2 → cell membrane destruction
- Lipase → fat necrosis
- Complement + kinin systems activated
↓
Acinar cell injury/death (apoptosis + necrosis)
↓
Release of proinflammatory cytokines: TNF-α, IL-1, IL-2, IL-6
↓
Neutrophil & macrophage recruitment into pancreas
↓
Local: pancreatic oedema → necrosis → abscess / pseudocyst
↓
Systemic: cytokine storm → SIRS → MODS → MSOF
- SPINK1 (Serine Protease Inhibitor Kazal Type 1) - binds and inactivates ~20% of trypsin
- Mesotrypsin and enzyme Y degrade active trypsin
- Low intra-acinar calcium prevents autoactivation
- Separation of zymogens from lysosomes in the Golgi apparatus
AETIOLOGY
| Letter | Cause |
|---|---|
| G | Gallstones (40-45% - most common in adults) |
| E | Ethanol/Alcohol (35-40%) |
| T | Trauma (blunt abdominal injury; post-op ischaemia) |
| S | Steroids |
| M | Mumps + other infections (coxsackievirus, EBV) |
| A | Autoimmune / hAemolytic uraemic syndrome |
| S | Scorpion venom / Structural abnormalities (pancreas divisum) |
| H | Hyperlipidaemia (triglycerides >1000 mg/dL) / Hypercalcaemia |
| E | ERCP (post-procedural) |
| D | Drugs (valproate, L-asparaginase, azathioprine, 6-MP, thiazides, furosemide, statins, metronidazole) |
CLINICAL FEATURES
Symptoms
- Epigastric pain radiating to the back - cardinal symptom; constant, severe, non-colicky
- Pain typically does NOT radiate to the shoulder (that is diaphragmatic irritation)
- Nausea and vomiting in ~90% - does NOT relieve the pain (unlike peptic ulcer)
- If pain disappears suddenly → consider another diagnosis (perforation?), or fat necrosis becoming walled off
Signs
| Sign | Description |
|---|---|
| Epigastric tenderness | With peritonism in severe cases; abdominal rigidity |
| Cullen's sign | Periumbilical bruising = retroperitoneal haemorrhage |
| Grey Turner's sign | Flank bruising = retroperitoneal haemorrhage |
| Both are RARE but = haemorrhagic (severe) pancreatitis | |
| Tetany | Hypocalcaemia (rare) |
| Jaundice | Choledocholithiasis or bile duct compression by pancreatic head oedema |
| Pleural effusion | Dullness at left base (from diaphragmatic involvement) |
| Tachycardia + hypotension | Third-space fluid loss → hypovolaemia |
| Abdominal distension | Paralytic ileus |
DIAGNOSIS
Revised Atlanta Classification (RAC) - Needs 2 of 3:
- Acute onset severe persistent epigastric pain ± radiation to back
- Serum amylase or lipase ≥ 3x upper limit of normal
- Characteristic imaging findings
Biochemistry
| Test | Comment |
|---|---|
| Serum lipase | More specific than amylase; preferred if presenting >48h; elevated 8-14 days |
| Serum amylase | Rises within hours; returns to normal 3-5 days; NOT specific (also raised in: peptic ulcer, cholecystitis, bowel obstruction, parotitis, renal failure) |
| ALT elevated + pancreatitis | 95% PPV for gallstone (biliary) pancreatitis |
| FBC | Leukocytosis; raised Hct suggests haemoconcentration from third-spacing |
| Glucose | Hyperglycaemia common |
| BUN + Creatinine | Elevated - from hypovolaemia / renal compromise |
| Serum Ca²⁺ | Low Ca²⁺ = fat saponification; poor prognosis |
| CRP | Peaks at 48-72 h; CRP >150 mg/L = severe pancreatitis |
| LDH, AST | Part of Ranson's criteria |
Imaging
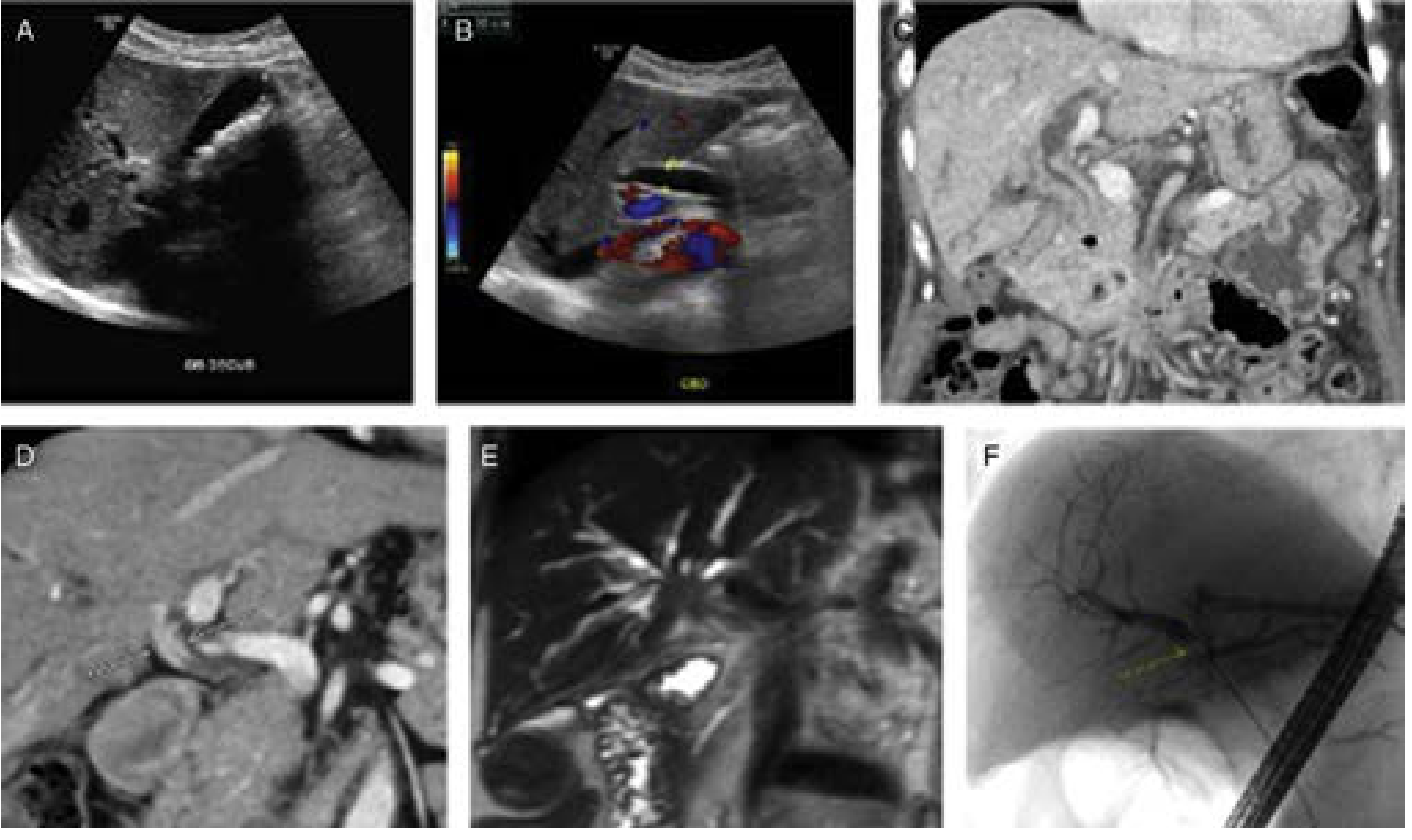
- Abdominal USS - First-line; high sensitivity (95%) for gallstones; limited view of pancreas by bowel gas
- CT abdomen with IV contrast (portal venous phase) - Gold standard for severity, necrosis assessment; best at 72-96 hours after onset
- Shows: pancreatic swelling, peripancreatic fat stranding, fluid collections, non-enhancing areas (= necrosis), extraluminal gas (= infected necrosis)
- MRCP - Best for pancreatic/biliary duct anatomy; used in unexplained/recurrent pancreatitis (NOT in acute setting)
- Plain AXR - Non-specific: "sentinel loop" (isolated ileus), "cut-off colon sign" at splenic flexure, pancreatic calcifications (chronic disease)
SEVERITY ASSESSMENT
Revised Atlanta Severity Classification (2012)
| Grade | Criteria |
|---|---|
| Mild | No organ dysfunction, no local/systemic complications; mortality <1% |
| Moderate | Transient organ failure (<48 h) and/or local/systemic complications |
| Severe | Persistent organ failure (>48 h); mortality 10-50% |
- Shock: systolic BP <90 mmHg
- Pulmonary insufficiency: PaO₂ <60 mmHg
- Renal failure: creatinine >2 mg/dL after resuscitation
- GI bleed >500 mL/24 h
Ranson's Criteria (gallstone pancreatitis)
| At Admission | During Initial 48 hours |
|---|---|
| Age >55 years | Haematocrit fall >10 points |
| WBC >16,000/mm³ | BUN elevation >5 mg/dL |
| Blood glucose >200 mg/dL | Serum Ca²⁺ <8 mg/dL |
| Serum LDH >350 IU/L | Arterial PaO₂ <60 mmHg |
| Serum AST >250 U/dL | Base deficit >4 mEq/L |
| Fluid sequestration >6 L |
CT Severity Index (Balthazar)
| Pancreatic Inflammation | Points | Pancreatic Necrosis | Points |
|---|---|---|---|
| Normal | 0 | None | 0 |
| Focal/diffuse enlargement | 1 | ≤30% | 2 |
| Fat inflammatory changes | 2 | 30-50% | 4 |
| Single fluid collection | 3 | >50% | 6 |
| Two+ collections or gas | 4 |
- CTSI 0-3: mortality 3%, morbidity 8%
- CTSI 4-6: mortality 6%, morbidity 35%
- CTSI 7-10: mortality 17%, morbidity 92%
BISAP Score (Bedside Index of Severity in AP - calculated at admission):
- BUN >25 mg/dL
- Impaired mental status
- SIRS present
- Age >60
- Pleural effusion
- Score 0-1: mortality <1% | Score 4-5: mortality >20%
Other markers:
- APACHE II score ≥8 = severe pancreatitis
- CRP >150 mg/L at 48-72 h = severe pancreatitis
- Serum procalcitonin, IL-6 also correlate with severity (not widely available)
LOCAL COMPLICATIONS - REVISED ATLANTA CLASSIFICATION
| Time | Interstitial Edematous | Necrotizing |
|---|---|---|
| <4 weeks | APFC (Acute Peripancreatic Fluid Collection) - no wall, homogeneous | ANC (Acute Necrotic Collection) - mixed liquid + solid, no wall |
| >4 weeks | Pseudocyst - homogeneous, encapsulated, round/oval, well-defined wall | WON (Walled-Off Necrosis) - mixed liquid/solid, encapsulated, well-defined wall |
- Pseudocyst = no solid debris, entirely fluid; can be drained simply
- WON = contains solid necrotic debris; needs step-up drainage approach
MANAGEMENT
Cornerstones (for ALL severities):
- Aggressive IV fluid resuscitation - Lactated Ringer's (LR) preferred over normal saline (LR associated with decreased SIRS odds at 24 h, OR 0.38)
- Pain control
- Early nutrition
Fluid Resuscitation
- Hypovolaemia = unfavourable prognostic factor
- Rate must be individualised based on: age, comorbidities, vital signs
- Monitor: urine output (target ≥0.5 mL/kg/hr), BUN, Hct, vital signs
Pain Management
- NSAIDs (e.g. IV metamizole 2 g/8 h) for mild pain
- Opioids for moderate-severe pain: buprenorphine 0.3 mg/4 h IV, pentazocine, meperidine
- AVOID morphine - causes Sphincter of Oddi spasm (worsens biliary obstruction)
Nutrition
- Early enteral nutrition (NG or nasojejunal) = strongly preferred over TPN
- Lower infection rates, lower cost with enteral feeding
- NG feeding as effective as NJ in most cases; NJ preferred if gastric retention from duodenal oedema
- TPN only if enteral route not tolerated
Antibiotics
- NOT indicated for mild-moderate sterile pancreatitis
- Indicated for:
- Documented infected necrosis
- Concurrent cholangitis
- Secondary infections
- Carbapenems = first choice (best pancreatic penetration)
- Alternatives: quinolones + metronidazole, 3rd-gen cephalosporins, piperacillin
Specific Interventions
- ERCP only if: concurrent cholangitis or proven biliary obstruction (hyperbilirubinaemia + dilated CBD)
- Early ERCP for ALL mild biliary pancreatitis = NOT recommended
- Early cholecystectomy (within 3 days) for mild biliary pancreatitis = standard of care
- Most resolve spontaneously
- Drain if: symptomatic, infected, expanding, causing obstruction
- Endoscopic internal drainage (EUS-guided transgastric stenting) preferred
- Delay intervention as long as possible to allow WON to develop (>4 weeks ideal)
- Step-up approach:
- IV antibiotics (carbapenems)
- Percutaneous drainage (CT/USS-guided)
- Endoscopic internal drainage (EUS-guided, through stomach wall) - preferred if collection adjacent to stomach
- Minimally invasive necrosectomy (video-assisted retroperitoneal debridement - VARD)
- Open surgical necrosectomy - last resort (high morbidity/mortality)
SYSTEMIC COMPLICATIONS
| Complication | Mechanism |
|---|---|
| Hypovolaemic shock | Massive third-space fluid loss into retroperitoneum and peritoneum |
| ARDS | TNF-α, IL-1 damage pulmonary endothelium → non-cardiogenic pulmonary oedema |
| AKI | Hypovolaemia → acute tubular necrosis |
| Hypocalcaemia | Fat saponification consumes Ca²⁺; also hypoalbuminaemia |
| Hyperglycaemia | Beta-cell destruction; glucagon release from inflamed islets |
| Coagulopathy / DIC | Activated enzymes trigger coagulation cascade |
| SIRS → MODS | Cytokine storm involving TNF-α, IL-1, IL-6 |
| Pleural effusion | Left-sided most common; from diaphragmatic lymphatic spread |
| Splenic vein thrombosis | Local inflammation; causes left-sided (sinistral) portal hypertension + gastric varices |
| Pseudoaneurysm | Splenic artery erosion by enzymes → torrential haemorrhage |
KEY EXAM POINTS
| Point | Fact |
|---|---|
| Most common cause | Gallstones (adults) |
| Most specific marker | Lipase (preferred if >48 h after onset) |
| Radiating pain character | Epigastric → BACK; constant, not colicky |
| Cullen + Grey Turner | Haemorrhagic pancreatitis; both RARE |
| AVOID this analgesic | Morphine (sphincter of Oddi spasm) |
| Best IV fluid | Lactated Ringer's (decreased SIRS vs. normal saline) |
| ERCP indication | Cholangitis OR proven biliary obstruction ONLY |
| Pseudocyst definition | Fluid collection with wall, NO solid debris, takes ≥4 weeks |
| WON vs Pseudocyst | WON = mixed solid/liquid content; harder to drain |
| CRP threshold for severe | >150 mg/L at 48-72 h |
| Ranson ≥3 | Severe pancreatitis |
| CTSI ≥7 | Mortality 17%, morbidity 92% |
| Antibiotic choice for infected necrosis | Carbapenems (best pancreatic penetration) |
| Surgery timing | Delay as long as possible; early surgery = worse outcomes |
| Late mortality cause | Sepsis from infected pancreatic necrosis |
| Early mortality cause | MODS from inflammatory cytokine storm |
Acute cholangitis secondary to obstructive jaundice likely due to choledocholithiasis
ACUTE CHOLANGITIS - COMPLETE GUIDE
DEFINITION
PATHOPHYSIOLOGY
Normal Biliary Defence Mechanisms (that protect against infection):
- Sphincter of Oddi - mechanical barrier preventing reflux of duodenal bacteria
- Laminar bile flow - continual flushing flushes ascending bacteria out of the biliary tree
- Bile salts - bacteriostatic properties that inhibit bacterial colonization
How Choledocholithiasis Causes Cholangitis:
Gallstone enters CBD (choledocholithiasis)
↓
Partial or complete biliary obstruction
↓
Bile flow disrupted → stasis of bile
↓
Bacteria enter biliary tree via:
1. Reflux from duodenum through incompetent/bypassed Sphincter of Oddi
2. Haematogenous spread via portal vein
↓
Bacteria proliferate in stagnant bile (bactibilia in 90% of CBD obstruction)
↓
Intraluminal pressure ↑ → cholangiovenous reflux → bacteria enter bloodstream
↓
Bacteraemia → sepsis → septic shock (Reynolds pentad)
↓
Pyogenic liver abscess (if not treated)
CAUSES OF ACUTE CHOLANGITIS
| Intrinsic Obstruction | Extrinsic Obstruction | Seeding of Biliary Tree |
|---|---|---|
| Choledocholithiasis (most common) | Mirizzi's syndrome | ERCP |
| Benign/malignant stricture | Pancreatic carcinoma | Sphincterotomy |
| Cholangiocarcinoma | Ampullary/gallbladder/duodenal cancer | Biliary stent insertion |
| Stent occlusion | Chronic pancreatitis | Biliary drain placement |
| Blood clot / polyp | Periampullary diverticulum (Lemmel syndrome) | Biliary-enteric anastomosis |
| Infectious parasites |
CLINICAL FEATURES
Charcot's Triad (classic but low sensitivity <50%):
- Fever (and/or rigors/shaking chills)
- Jaundice (obstructive - dark urine, pale stools, pruritus)
- Right upper quadrant (RUQ) pain
Jaundice is actually the least common of the three findings
Reynolds Pentad (= Charcot's triad + 2 additional ominous signs):
- Hypotension (septic shock)
- Altered mental status (confusion, drowsiness)
Reynolds pentad = suppurative (severe) cholangitis - mortality approaches 100% without prompt treatment
Additional Features:
- Tender hepatomegaly
- Signs of sepsis: tachycardia, tachypnoea, high fever
- Dark urine, pale/clay-coloured stools, pruritus (obstructive jaundice features)
INVESTIGATIONS
Laboratory Workup
| Test | Expected Finding |
|---|---|
| FBC | Leukocytosis (WBC >12,000) |
| LFTs | Cholestatic pattern: ↑↑ bilirubin (conjugated), ↑ ALP, ↑ GGT |
| Transaminases | Mildly elevated; significantly elevated if microabscesses form |
| PT/INR | May be elevated (hepatic dysfunction or coagulopathy) |
| Blood cultures | Positive in 20-70% of cases - take before antibiotics |
| Biliary cultures | Positive in 60-90% of cases (more sensitive than blood) |
| CRP | Elevated |
| Serum bilirubin | ≥2 mg/dL in definite diagnosis |
| CA19-9 | May be elevated with biliary obstruction - NOT specific for malignancy; recheck after obstruction resolves |
| Amylase/Lipase | If concurrent gallstone pancreatitis |
Microbiology - Common Pathogens
| Gram-negative rods (most common) | Gram-positive | Anaerobes |
|---|---|---|
| E. coli | Enterococcus | Bacteroides |
| Klebsiella | Streptococcal species | Clostridium |
| Enterobacter | ||
| Pseudomonas | ||
| Citrobacter |
ESBL-producing organisms (Extended-Spectrum Beta-Lactamase) are increasingly common - always consider local resistance patterns
Imaging
| Modality | Role | Sensitivity/Specificity |
|---|---|---|
| Abdominal USS | First-line - look for CBD dilation, cholelithiasis, gallbladder sludge | 40% sensitive but ~100% specific (when positive). Limited: operator-dependent, misses small stones, false-negative in acute obstruction before ducts dilate |
| CT abdomen | Identifies biliary dilation, site of obstruction, liver abscesses, portal vein thrombosis | Low sensitivity for choledocholithiasis specifically |
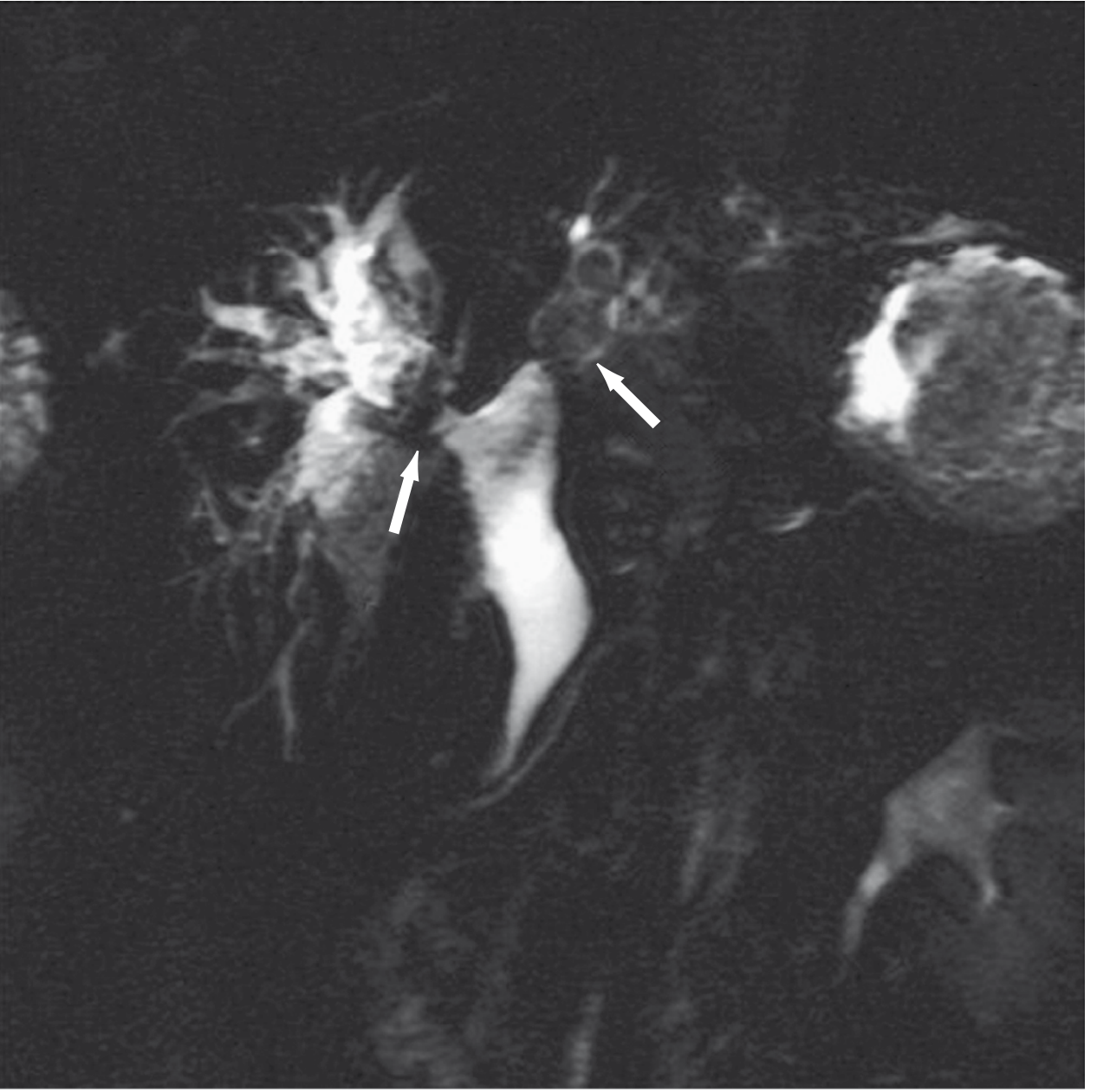
| MRCP | Best non-invasive modality for choledocholithiasis and biliary anatomy; increasingly first-choice | 90% sensitive, 95% specific for CBD stones; sensitivity drops for stones <6 mm |
| EUS | Better than MRCP for very small stones; used if high ERCP risk and MRCP unavailable | High accuracy; invasive |
| ERCP | Diagnostic AND therapeutic - gold standard; allows stone removal, sphincterotomy, stenting | Only use if treatment expected (not purely diagnostic) |
| PTC (Percutaneous Transhepatic Cholangiography) | When ERCP fails or not feasible | Allows drainage from above |
| HIDA scan | Not useful in cholangitis - biliary infection reduces radionuclide secretion, giving false results | Unreliable |
DIAGNOSTIC CRITERIA - TOKYO GUIDELINES 2018
Suspected Diagnosis: 1 item from A + 1 item from B or C
Definite Diagnosis: 1 item from A + 1 item from B + 1 item from C
| Category | Criteria |
|---|---|
| A - Systemic Inflammation | Fever and/or chills; elevated WBC or CRP |
| B - Cholestasis | Jaundice (clinically); OR bilirubin ≥2 mg/dL; OR elevated ALP, GGT, ALT, AST >1.5x ULN |
| C - Imaging | Biliary dilatation on imaging; OR evidence of cause (stone, stricture, stent) |
SEVERITY GRADING - TOKYO GUIDELINES 2018
| Grade | Criteria | Initial Management |
|---|---|---|
| Mild (Grade I) | Does not meet criteria for Grade II or III; clinically stable | IV antibiotics; low threshold for biliary drainage if no response within 24 h |
| Moderate (Grade II) | ≥2 of: WBC >12,000/mm³; fever >39°C; age ≥75; bilirubin ≥5 mg/dL; albumin <0.7x LLN | Early biliary drainage + antibiotics |
| Severe (Grade III) - Suppurative | Any organ dysfunction: cardiovascular (hypotension requiring norepinephrine or dopamine ≥5 µg/kg/min); neurologic (altered consciousness); respiratory (P/F <300); renal (oliguria, Cr >2 mg/dL); hepatic (INR >1.5); haematologic (Plt <100,000) | ICU resuscitation + broad-spectrum antibiotics + urgent biliary drainage once stabilised |
Severity should be reassessed at: time of diagnosis, within 24 hours, and at 24-48 hours
MANAGEMENT
Principles:
Step 1: Immediate Resuscitation
- IV access, IV fluids (aggressive crystalloid resuscitation)
- NBM
- Urinary catheter (monitor urine output ≥0.5 ml/kg/hr)
- ICU admission for severe/Grade III cholangitis
- Vasopressors if septic shock (norepinephrine first-line)
Step 2: Antibiotic Therapy
- Take blood cultures FIRST, then start antibiotics immediately
- Cover gram-negative rods (E. coli, Klebsiella) + gram-positive (Enterococcus) + anaerobes
| Severity | Antibiotic Regimen |
|---|---|
| Mild-Moderate | Piperacillin-tazobactam OR 3rd-gen cephalosporin + metronidazole |
| Severe | Carbapenem (meropenem/imipenem) ± vancomycin |
| ESBL suspected | Carbapenem |
- 4-7 days after source control obtained
- 14 days if bacteraemia is present (risk of endocarditis)
Step 3: Biliary Drainage
| Procedure | Description |
|---|---|
| ERCP + biliary sphincterotomy | Incises the sphincter of Oddi to allow stone passage |
| ERCP + stone extraction | Using balloon sweep or basket retrieval |
| ERCP + biliary stenting | Temporary stent inserted to re-establish bile flow; stone removal deferred if patient unstable |
| EUS-guided choledochoduodenostomy | Alternative to ERCP where available; avoids percutaneous access |
Biliary drainage within 24 h of diagnosis = associated with increased survival rate Delay >48 h = associated with higher costs and longer hospital stay
- PTC (Percutaneous Transhepatic Cholangiography) - access from above (liver) under imaging guidance
- Surgical biliary drainage - open common bile duct exploration + T-tube insertion (reserved for unstable patients where all other methods failed)
Step 4: Definitive Treatment
- After acute phase resolves → elective laparoscopic cholecystectomy (definitive; without this, risk of recurrent cholangitis is HIGH even after sphincterotomy)
- Early cholecystectomy during index admission is increasingly being studied and showing no increased complication rates
- Resectable: hepatic resection or Whipple's procedure (pancreaticoduodenectomy)
- Unresectable: palliative biliary bypass - Roux-en-Y hepaticojejunostomy (preferred) or choledochoduodenostomy
- Transduodenal sphincteroplasty - surgical incision of the ampulla; risk of pancreatic duct injury causing recurrent pancreatitis
COMPLICATIONS OF ACUTE CHOLANGITIS
| Complication | Mechanism |
|---|---|
| Septic shock | Bacteraemia → vasodilation → haemodynamic collapse |
| Pyogenic liver abscess | Direct extension of biliary infection into hepatic parenchyma |
| Portal pyaemia | Septic portal vein thrombosis |
| Acute renal failure | Sepsis + hypovolaemia → ATN |
| DIC | Endotoxin-mediated coagulation activation |
| Acute pancreatitis | Stone impaction at ampulla → pancreatic duct obstruction |
| Recurrent cholangitis | If underlying cause (stones) not addressed |
| Secondary biliary cirrhosis | Chronic obstruction |
OUTCOMES
- With improved ERCP techniques + antibiotics, mortality from acute cholangitis has fallen from 50% → ~10%
- 85% of cases resolve with antibiotics + non-surgical biliary drainage (ERCP)
- Mortality remains high in: elderly, immunocompromised, severe/Grade III cholangitis
- Without treatment of Reynolds pentad: mortality approaches 100%
QUICK EXAM SUMMARY
| Point | Key Fact |
|---|---|
| Most common cause | Choledocholithiasis |
| Classic triad | Charcot's triad: fever + jaundice + RUQ pain |
| Ominous pentad | Reynolds pentad: Charcot + hypotension + altered consciousness |
| Organism | E. coli, Klebsiella (most common gram-negative rods) |
| Bactibilia rate | 90% with complete CBD obstruction |
| First imaging | Abdominal USS |
| Best non-invasive imaging | MRCP (90% sensitive, 95% specific for stones) |
| Gold-standard treatment | ERCP + stone extraction ± sphincterotomy |
| Drain within | 24 hours - improved survival |
| Antibiotic duration | 4-7 days after source control; 14 days if bacteraemic |
| Definitive surgery | Laparoscopic cholecystectomy (after acute phase) |
| ERCP NOT indicated | In gallstone pancreatitis WITHOUT cholangitis/obstruction |
| Avoid HIDA scan | Unreliable in active biliary infection |
ASIATIC CHOLANGIOHEPATITIS
ASIATIC CHOLANGIOHEPATITIS (ACH)
DEFINITION
- Intrahepatic and/or extrahepatic biliary calculi (brown pigment stones)
- Biliary strictures (intrahepatic)
- Recurrent episodes of bacterial cholangitis
EPIDEMIOLOGY
- Endemic to East and Southeast Asia: China, Taiwan, Hong Kong, Korea, Japan, Vietnam, Philippines, Malaysia
- Prevalence >10% in parts of East Asia (especially Taiwan)
- Age: Predominantly 3rd-4th decade of life
- Sex: Males and females equally affected
- Risk factors: Low socioeconomic status; poor sanitation; areas where gastrointestinal parasitosis is endemic
- Now increasingly seen in Western countries due to migration from endemic areas
AETIOLOGY & PATHOGENESIS
Causative Organisms:
| Parasite | Type | Route |
|---|---|---|
| Clonorchis sinensis (Chinese liver fluke) | Trematode (fluke) | Ingestion of undercooked freshwater fish |
| Ascaris lumbricoides | Nematode (roundworm) | Faeco-oral; larvae migrate into bile duct |
| Opisthorchis viverrini | Trematode | Undercooked fish (Southeast Asia) |
Mechanism of Brown Pigment Stone Formation:
Parasites enter biliary tree
↓
Parasites + bacteria secrete β-glucuronidase enzyme
↓
β-glucuronidase hydrolyses water-soluble conjugated bilirubin glucuronides
↓
Free (unconjugated) bilirubin released → insoluble
↓
Free bilirubin precipitates with calcium
↓
CALCIUM BILIRUBINATE (brown pigment) stones form
↓
Stones + dead parasite fragments + bacteria accumulate in intrahepatic + CBD
↓
Partial/complete biliary obstruction → bile stasis
↓
Bacterial superinfection of stagnant bile (E. coli, Klebsiella most common)
↓
Recurrent episodes of acute cholangitis
↓ (chronic)
Intrahepatic strictures → segmental/lobar atrophy or hypertrophy
Pyogenic liver abscesses
Secondary biliary cirrhosis
Cholangiocarcinoma
It is still debated whether the primary event is infection causing inflammatory stricture, or inflammatory stricture causing infection of stagnant bile - likely a vicious cycle.
Key Stone Type:
- Brown pigment stones (soft, earthy, friable) - found in intrahepatic + extrahepatic ducts
- Distinct from cholesterol stones (Western; in gallbladder) and black pigment stones (haemolysis)
DISTRIBUTION - ANATOMICAL PATTERN
- Predominantly involves intrahepatic bile ducts with focal strictures + dilations
- Left hepatic duct more commonly involved than right - due to its more acute angulation (the sharper bend predisposes to stasis and stone impaction)
- CBD may also be involved (choledocholithiasis)
- Disease may be unilateral (one lobe) or bilateral
- In chronic cases: lobar/segmental atrophy or hypertrophy due to longstanding ductal obstruction
CLINICAL FEATURES
Acute Presentation:
- Charcot's Triad: RUQ/epigastric pain + fever/rigors + jaundice
- Nausea, vomiting
- Tender hepatomegaly
- Signs of sepsis if severe (Reynolds pentad in suppurative cases)
- Jaundice tends to be MILD (because stones are segmental/lobar, not causing complete obstruction of the whole biliary tree)
Chronic/Atypical Presentation:
- Recurrent attacks of RUQ pain + fever, often for months-years before diagnosis
- Symptoms may be subtle and go unrecognised for long periods
- Progressive weight loss
- Features of portal hypertension if cirrhosis develops (splenomegaly, varices, ascites)
INVESTIGATIONS
Blood Tests:
| Test | Finding |
|---|---|
| WBC | Leukocytosis |
| Bilirubin | Elevated (conjugated); tends to be mild-moderate |
| ALP | Markedly elevated (cholestatic pattern) |
| GGT | Elevated |
| ALT/AST | Mildly elevated |
| Blood cultures | Positive in active cholangitis episodes |
Stool / Serology:
- Stool microscopy for ova and parasites (Ascaris, Clonorchis eggs)
- Serology for Clonorchis/Opisthorchis antibodies
Imaging:
| Modality | Findings |
|---|---|
| USS (Abdominal Ultrasound) | First-line; shows dilated intrahepatic ducts, intrahepatic calculi, cholangitic abscesses, segmental atrophy/hypertrophy |
| CT Abdomen | Shows dilated intrahepatic ducts, stones (may be hyperdense), ductal air (aerobilia from prior intervention or fistula), liver abscesses, atrophy |
| MRCP | Investigation of choice - non-invasive; shows entire biliary tree including proximal to strictures; identifies stones as filling defects; maps strictures; does NOT aggravate biliary sepsis |
| ERCP | Diagnostic AND therapeutic; limited by inability to visualise proximal to tight strictures |
| PTC (Percutaneous Transhepatic Cholangiography) | When ERCP insufficient; allows access to peripheral ducts |
| Cholangioscopy (POCS/PTCS) | Direct visualisation + biopsy of strictures; targeted lithotripsy |
COMPLICATIONS
| Complication | Notes |
|---|---|
| Pyogenic liver abscess | From cholangitic extension into hepatic parenchyma |
| Secondary biliary cirrhosis | Prevalence ~7%; from chronic biliary obstruction |
| Portal hypertension | Secondary to cirrhosis |
| Cholangiocarcinoma | Most feared complication; prevalence 3-5% (higher with Clonorchis sinensis); especially if predominantly one lobe involved |
| Septicaemia/septic shock | From acute cholangitis episodes |
| Hepatic atrophy | Of the affected lobe/segment (left > right) |
MANAGEMENT
Phase 1: Acute Attack Management
- IV antibiotics (broad-spectrum: cover gram-negatives + anaerobes)
- Piperacillin-tazobactam OR carbapenem (for severe)
- Metronidazole for anaerobic cover
- IV fluids + resuscitation
- Analgesia
- If no response → urgent biliary drainage (ERCP or PTC)
Phase 2: Definitive/Elective Management
A. Endoscopic (ERCP-based) - preferred for CBD + main intrahepatic ducts
- Biliary decompression - plastic stent or nasobiliary tube (NBT)
- Cholangiogram to localise stones and strictures
- Guidewire across stricture
- Balloon dilation of strictures
- Brush cytology of suspicious strictures (exclude cholangiocarcinoma)
- Stone fragmentation: mechanical lithotripsy OR electrohydraulic lithotripsy (EHL) OR laser lithotripsy
- Stone retrieval (balloon sweep / basket extraction)
- Plastic stent placement if residual stones/strictures
Complete ductal clearance achieved in only ~32-67% of cases - multiple sessions often needed Limitations: Cannot reach peripheral intrahepatic ducts; high recurrence rate
B. Cholangioscopy (Peroral or Percutaneous)
- Direct visualisation of biliary tree beyond ERCP limits
- Allows targeted intraductal lithotripsy and biopsy of strictures
- Peroral cholangioscopy (POCS) for main ducts; percutaneous transhepatic cholangioscopy (PTCS) for peripheral disease
C. Percutaneous Transhepatic Approach (PTC/PTCS)
- When strictures/stones are in peripheral biliary ducts inaccessible by ERCP
- Allows progressively larger dilations + stone extraction over weeks-months
D. Surgical Management - almost always required eventually
- Predominantly left-sided disease with left lobe atrophy
- Intrahepatic strictures not amenable to endoscopy
- Risk of cholangiocarcinoma in a diseased lobe
- Failure of endoscopic/percutaneous clearance
- Remove ALL stones (intraoperative choledochoscopy)
- Bypass, enlarge, or resect strictures
- Provide adequate long-term biliary drainage
| Procedure | Indication |
|---|---|
| Hepaticojejunostomy (Roux-en-Y) | For biliary-enteric drainage; if future endoscopic access needed, the Roux limb end brought out as a cutaneous stoma for choledochoscopy access |
| Hepatic resection (lobectomy/segmentectomy) | Left-sided or unilateral disease; atrophied lobe; risk of cholangiocarcinoma; when stone clearance not achievable |
| Choledochotomy + T-tube | Temporary drainage after CBD exploration |
| Transduodenal sphincteroplasty | Impacted ampullary stones; risk: pancreatic duct injury |
Left hepatectomy is commonly required because the left hepatic duct is disproportionately affected
"Sump Roux limb" - when a Roux limb is exteriorised as a stoma - allows repeated endoscopic access to intrahepatic ducts postoperatively for residual/recurrent stone removal
Antiparasitic Treatment
- Praziquantel - for Clonorchis sinensis and Opisthorchis viverrini (drug of choice)
- Albendazole/Mebendazole - for Ascaris lumbricoides
SURVEILLANCE FOR CHOLANGIOCARCINOMA
- All patients require long-term follow-up
- Annual or biannual MRCP or CT to monitor for malignant transformation
- Suspicious strictures → ERCP with brush cytology/cholangioscopy biopsy
- Disease predominantly in one lobe = resect (to remove at-risk tissue)
- Serum CA 19-9 as tumour marker (limited specificity)
QUICK SUMMARY TABLE
| Feature | ACH |
|---|---|
| Other names | Oriental cholangiohepatitis, Recurrent pyogenic cholangitis, Hepatolithiasis |
| Region | East/Southeast Asia |
| Key parasites | Clonorchis sinensis, Ascaris lumbricoides |
| Mechanism | β-glucuronidase → free bilirubin → brown pigment stones |
| Stone type | Soft brown calcium bilirubinate (intrahepatic + CBD) |
| Lobe predominantly affected | Left (acute angle of left hepatic duct) |
| Classic triad | Biliary stones + strictures + recurrent cholangitis |
| Best imaging | MRCP (initial non-invasive) |
| Jaundice character | Usually mild (segmental obstruction) |
| Worst complication | Cholangiocarcinoma (3-5%) |
| Cirrhosis rate | ~7% |
| Antiparasitic | Praziquantel (flukes), Albendazole (roundworms) |
| Definitive treatment | ERCP/PTC for drainage + stones; often surgery required |
| Surgery of choice | Hepaticojejunostomy ± hepatic resection |
| Left lobe atrophy | Resect |
Cholelithiasis
CHOLELITHIASIS - COMPLETE GUIDE
DEFINITION
EPIDEMIOLOGY
- Affects ~15-20% of adults in Western countries
- Second most common cause of surgical admission
- ~80% remain asymptomatic throughout life
- Women affected 2-3x more than men (oestrogen effect)
- Incidence increases with age
TYPES OF GALLSTONES
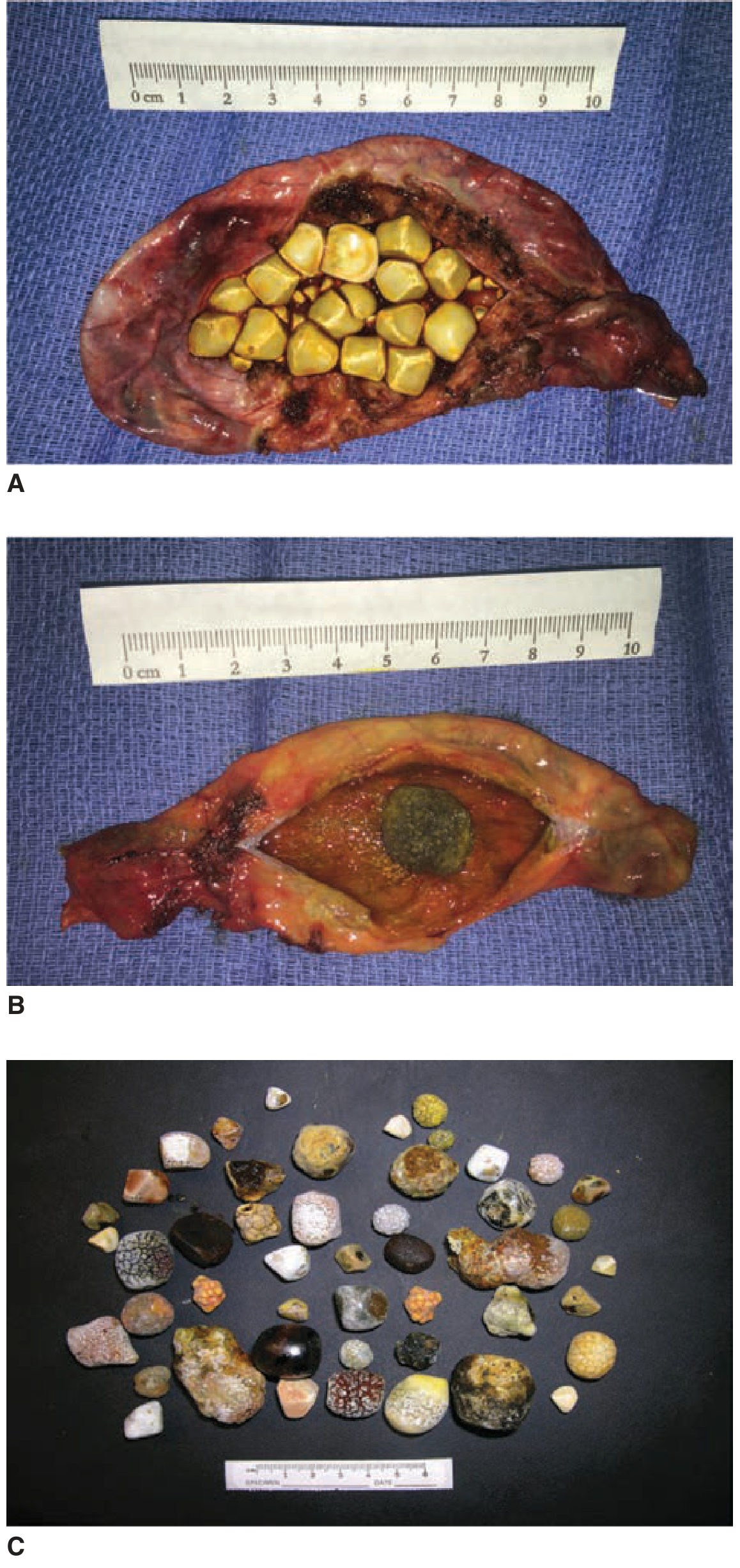
Comparison of Stone Types
| Feature | Cholesterol Stones | Black Pigment Stones | Brown Pigment Stones |
|---|---|---|---|
| Prevalence (West) | ~80% of all stones | ~15-20% | Uncommon in West |
| Colour | Whitish-yellow to green | Dark black, brittle, spiculated | Brownish-yellow, soft, mushy |
| Composition | ≥70% cholesterol | Calcium bilirubinate (polymerised) | Calcium bilirubinate + bacterial debris |
| Location | Gallbladder | Gallbladder | Bile ducts (intra + extrahepatic) |
| Radiopaque? | ~90% radiolucent (10% calcified = opaque) | Often radioopaque | Radiolucent |
| Number/size | Single large OR multiple mixed | Small, multiple | <1 cm, multiple |
| Aetiology | Cholesterol supersaturation | Haemolysis; cirrhosis; fasting | Bacterial infection + stasis (Ascaris, Clonorchis) |
| Association | Female, fat, forty, fertile, fair | Sickle cell, haemolytic anaemia, TPN | Asian populations; ACH/RPC |
PATHOGENESIS
Cholesterol Stone Formation - 3 Key Steps:
Step 1: SUPERSATURATION
Cholesterol hypersecretion into bile
→ cholesterol concentration exceeds capacity of bile salts
and phospholipids (lecithin) to keep it in solution
→ bile becomes LITHOGENIC (supersaturated)
Step 2: NUCLEATION
Cholesterol crystals precipitate out of supersaturated bile
→ enhanced by mucin glycoproteins (pronucleating agents)
→ inhibited by apolipoproteins A1 and A2
Step 3: STONE GROWTH / GALLBLADDER STASIS
Crystals aggregate and grow
→ impaired gallbladder motility = stasis → stone enlargement
- Cholesterol
- Bile salts (bile acids)
- Lecithin (phospholipid)
Black Pigment Stone Formation:
- Excess unconjugated bilirubin (from haemolysis) in bile
- Deconjugation of bilirubin → free bilirubin precipitates with calcium
- Occurs in: haemolytic anaemias (sickle cell, hereditary spherocytosis, thalassaemia), cirrhosis, prolonged TPN, ileal disease (Crohn's - impaired bile salt reabsorption), vagotomy
Brown Pigment Stone Formation:
- Bacterial β-glucuronidase hydrolyses conjugated bilirubin → free bilirubin + calcium bilirubinate = soft brown stones
- Associated with biliary stasis + infection (E. coli, Klebsiella) and parasites (Ascaris, Clonorchis)
- Form in bile DUCTS (not just gallbladder)
RISK FACTORS - "THE Fs" (for cholesterol stones)
| Risk Factor | Mechanism |
|---|---|
| Female | Oestrogen ↑ cholesterol secretion; progesterone ↓ gallbladder motility |
| Fat (obesity) | ↑ cholesterol synthesis and secretion |
| Forty (age >40) | Gallbladder motility decreases with age |
| Fertile (multiparous) | Pregnancy → oestrogen + progesterone effects; gallbladder stasis |
| Fair (Caucasian/Native American) | Genetic predisposition (LITH genes) |
| Fatty diet | ↑ cholesterol load |
| Family history | Genetic factors in cholesterol metabolism |
| Drugs | OCP, fibrates (↑ cholesterol secretion), octreotide, ceftriaxone |
| Rapid weight loss / TPN | Biliary stasis |
| Ileal disease or resection | ↓ bile salt reabsorption → depleted bile salt pool |
| Diabetes | Impaired gallbladder motility |
CLINICAL PRESENTATIONS
Asymptomatic (silent) gallstones → 80%
↓
Biliary colic (symptomatic cholelithiasis)
↓
Acute cholecystitis (cystic duct obstruction + inflammation)
↓
Complications:
├── Empyema of gallbladder
├── Perforation → bile peritonitis
├── Mucocele/Hydrops of gallbladder
├── Mirizzi syndrome
├── Choledocholithiasis (CBD stone) → obstructive jaundice
│ ↓
│ Acute cholangitis / Gallstone pancreatitis
├── Gallstone ileus (Bouveret syndrome)
└── Gallbladder carcinoma (long-term, rare)
1. Asymptomatic (Silent) Cholelithiasis
- ~80% of gallstone carriers
- Found incidentally on USS for other reasons
- Do NOT require cholecystectomy routinely
- Exceptions: porcelain gallbladder (calcified wall - controversial), immunocompromised patients, very large stones (>3 cm - increased CA risk)
2. Biliary Colic (Symptomatic Cholelithiasis)
- Pain: Constant (not truly "colic") - RUQ or epigastric, severe, rapid onset
- Radiation: To right scapula or between the shoulder blades (infrascapular)
- Duration: 1-5 hours, then resolves spontaneously
- Triggers: Fatty meal (CCK release → gallbladder contraction), often wakes patient at night
- Associated: Nausea, vomiting; may have mild RUQ tenderness
- Between attacks: Patient is completely well; normal WBC + LFTs
- Association with meals: only ~50% of patients
- If pain lasts >24 hours → suspect acute cholecystitis or impacted stone
3. Acute Cholecystitis
- Severe RUQ pain, constant, lasting >24 hours (unlike biliary colic)
- Fever, nausea, vomiting
- Murphy's sign - inspiratory arrest on deep palpation of RUQ (patient catches breath when inflamed GB hits examiner's fingers)
- Ultrasonographic Murphy's sign - tenderness directly over GB on USS probe pressure
- Guarding and rigidity if perforation
- Lab: Leukocytosis; mild ↑ bilirubin, ALP; ↑ CRP
- Empyema - gallbladder fills with pus; septic patient
- Gangrenous cholecystitis - ischaemia → wall necrosis; risk of perforation
- Perforation → biliary peritonitis or pericholecystic abscess
- Emphysematous cholecystitis - gas-forming organisms (Clostridium, E. coli) - seen in diabetics; surgical emergency
- Occurs in critically ill patients (ICU, burns, trauma, post-op, TPN)
- Mechanism: gallbladder ischaemia + stasis + infection
- Higher mortality than calculous cholecystitis
4. Choledocholithiasis (CBD Stones)
- Stones pass from gallbladder into CBD (secondary stones) or form in CBD (primary brown stones)
- Presents with: obstructive jaundice, dark urine, pale stools, pruritus
- ↑ bilirubin (conjugated), ↑ ALP, ↑ GGT; ± ↑ amylase
- Complications: acute cholangitis (Charcot's triad), gallstone pancreatitis
- Treatment: ERCP + sphincterotomy + stone extraction; then cholecystectomy
5. Mirizzi Syndrome
- Large stone in Hartmann's pouch or cystic duct extrinsically compresses the adjacent common hepatic duct
- Causes obstructive jaundice from OUTSIDE the duct (not choledocholithiasis)
- Can erode through and form a cholecystocholedochal fistula
- Difficult cholecystectomy; risk of bile duct injury
6. Gallstone Ileus
- Large gallstone erodes through GB wall into adjacent duodenum (cholecystoduodenal fistula) → passes into small bowel → obstructs at the terminal ileum (narrowest point)
- Classic plain AXR: Rigler's triad = (1) bowel obstruction, (2) ectopic gallstone, (3) pneumobilia (air in biliary tree from fistula)
- Treatment: enterotomy + stone extraction; fistula may be dealt with later
INVESTIGATIONS
Blood Tests
| Test | Finding |
|---|---|
| FBC | Normal (biliary colic); leukocytosis (cholecystitis/cholangitis) |
| LFTs | Normal (biliary colic); ↑ bilirubin + ALP (CBD obstruction) |
| Amylase/lipase | ↑ if concurrent pancreatitis |
| Serum bilirubin | Conjugated hyperbilirubinaemia in choledocholithiasis |
| ALT | Elevated ALT in gallstone pancreatitis = 95% PPV for biliary cause |
Imaging
| Modality | Use | Notes |
|---|---|---|
| Abdominal USS | First-line | Sensitivity 95% for gallbladder stones; 40% for CBD stones. Shows: echogenic foci with posterior acoustic shadowing, GB wall thickening (>3 mm), pericholecystic fluid, dilated CBD (>6 mm normal, >8 mm post-cholecystectomy) |
| Plain AXR | Limited | Only 10-15% of stones are radioopaque (calcified). Useful for gallstone ileus (Rigler's triad), emphysematous cholecystitis (gas in GB wall) |
| CT Abdomen | Complications | Identifies gangrenous cholecystitis, perforation, abscess, GB carcinoma; LOW sensitivity for soft cholesterol stones |
| MRCP | Best non-invasive for CBD | 90% sensitive, 95% specific for choledocholithiasis; maps biliary anatomy |
| ERCP | Diagnostic + therapeutic | For CBD stones; allows sphincterotomy + extraction |
| HIDA Scan | Functional study | Non-visualisation of GB = cystic duct obstruction = acute cholecystitis (when USS equivocal) |
| EUS | Small CBD stones | Better than MRCP for stones <6 mm |
MANAGEMENT
Asymptomatic Gallstones
- Watchful waiting - no treatment for most
- Annual incidence of developing symptoms: ~1-2%
- Prophylactic cholecystectomy considered for: porcelain gallbladder (debated), very large stones (>3 cm), immunocompromised, transplant patients, patients in remote areas
Biliary Colic (Symptomatic, Uncomplicated)
- Elective laparoscopic cholecystectomy - definitive treatment
- Analgesia: diclofenac (NSAID) or opioids for acute attacks
- Low-fat diet while awaiting surgery
- Ursodeoxycholic acid (UDCA) - medical dissolution of small cholesterol stones; only works in ~50%; stones recur after stopping; rarely used now given widespread laparoscopic cholecystectomy
Acute Cholecystitis
- NBM, IV fluids
- IV antibiotics (cephalosporin + metronidazole OR piperacillin-tazobactam)
- Analgesia (NSAIDs + opioids)
- Early laparoscopic cholecystectomy within 24-72 hours of symptoms = gold standard
- Shorter hospital stay, lower complication rate vs delayed surgery
- Morbidity 2-3%, mortality 0.1-0.5%
- Tokyo Guidelines recommend early lap cholecystectomy for Grade I (mild) and Grade II (moderate) cholecystitis in fit patients
- Percutaneous cholecystostomy (USS-guided drainage) for Grade III severe cholecystitis in unfit/unstable patients as a bridge to surgery
- Convert to open if critical view of safety not achieved, excessive bleeding, bile duct injury
Laparoscopic Cholecystectomy - Key Technical Points
- 4 ports: 12 mm umbilical (specimen extraction) + 3 × 5 mm (subxiphoid, RMC, RAAI)
- Triangle of Calot dissection: CBD (medially) + cystic duct (inferiorly) + inferior surface of liver (superiorly)
- Critical view of safety (CVS): Two and ONLY two structures entering GB, lower third of GB dissected off liver, cleared hepatocystic triangle - MUST be achieved before clipping
- Calot's node (Lund's node): Lymph node overlying cystic artery - useful landmark
- Intraoperative cholangiogram (IOC) if CBD stones suspected
- Clip cystic duct + cystic artery → divide → remove GB from liver bed
Choledocholithiasis
- ERCP + sphincterotomy + stone extraction - then cholecystectomy (ideally same admission or within 6 weeks)
- If ERCP fails: PTC or open CBD exploration + T-tube
- Retained CBD stones (post-cholecystectomy): ERCP first; if T-tube in situ, can extract through T-tube tract at 4 weeks
COMPLICATIONS OF CHOLECYSTECTOMY
| Complication | Notes |
|---|---|
| Bile duct injury | Most serious; 0.3-0.5% incidence; requires hepaticojejunostomy repair |
| Bile leak | From cystic duct stump or small ducts of Luschka |
| Retained CBD stone | Presents weeks-months post-op; treat with ERCP |
| Port site hernia | Especially at 12 mm umbilical port |
| Wound infection | More common if empyema/perforation |
| Post-cholecystectomy syndrome | Persistent symptoms; may be from retained stone, bile salt diarrhoea, or functional |
GALLBLADDER CARCINOMA (Association with Gallstones)
- Found in ~1% of cholecystectomy specimens
- Risk: long-standing gallstones (large stones >3 cm; porcelain GB), females, Native American
- Often presents late with advanced disease
- Prognosis poor if invasion beyond mucosa
QUICK SUMMARY TABLE
| Point | Key Fact |
|---|---|
| Most common stone type (West) | Cholesterol (80%) |
| Pathogenesis cholesterol stones | Supersaturation → nucleation → stasis/growth |
| Risk factor mnemonic | 5 Fs: Female, Fat, Forty, Fertile, Fair |
| 80% of gallstones | Asymptomatic - no treatment needed |
| Biliary colic pain | RUQ/epigastric → right scapula; 1-5 h, then resolves |
| Biliary colic vs cholecystitis | Colic <24 h and resolves; cholecystitis persists >24 h |
| First-line imaging | Abdominal ultrasound (USS) |
| Murphy's sign | Inspiratory arrest on RUQ palpation (acute cholecystitis) |
| Best for CBD stones non-invasively | MRCP (90% sensitive) |
| Definitive treatment | Laparoscopic cholecystectomy |
| CVS (Critical View of Safety) | Only TWO structures into GB; cleared hepatocystic triangle |
| Rigler's triad | Bowel obstruction + ectopic stone + pneumobilia = gallstone ileus |
| Mirizzi syndrome | External CBD compression by stone in Hartmann's pouch |
| Black pigment stones | Haemolysis, cirrhosis, TPN |
| Brown pigment stones | Bacterial infection + biliary stasis; Asian populations |
| Acalculous cholecystitis | Critically ill patients (ICU, burns); no stones; high mortality |
Breast cancer 10 including examination
Breast cancer 101 including examination
BREAST CANCER 101 - COMPLETE GUIDE
EPIDEMIOLOGY
- Most common cancer in women worldwide - ~2.3 million new cases in 2020 (~25% of all cancers in women)
- In Western Europe: 1 in 9 women will develop breast cancer in their lifetime
- Accounts for 3-5% of all deaths in women in high-income countries
- In resource-poor countries: 1 in 28 women affected; for every 2 diagnosed, 1 dies
- Median age of presentation: ~60 years (West); ~48 years in low/middle-income countries
- Male breast cancer: 0.5-1% of all breast cancers
RISK FACTORS
Modifiable Risk Factors
| Factor | Relative Risk |
|---|---|
| Obesity (BMI >30) | RR 1.29 (postmenopausal women) |
| HRT use >10 years | RR 1.2 |
| Late first pregnancy (>35 years) | Increased risk |
| Nulliparity | Increased risk |
| Tobacco ≥25 cigarettes/day | RR 1.14 |
| Alcohol (moderate 3-4 drinks/day) | RR 1.32 |
| Radiation exposure | RR 6 |
| Breastfeeding >12 months | Protective |
Non-Modifiable Risk Factors
| Factor | Details |
|---|---|
| Age | Risk increases with age |
| Female sex | 99-99.5% of cases |
| Early menarche / Late menopause | ↑ lifetime oestrogen exposure |
| BRCA1 mutation (17q21) | 50-85% lifetime risk of breast CA; 40% ovarian CA risk |
| BRCA2 mutation (13q12.3) | 50-60% lifetime risk; 20% ovarian CA; also prostate, pancreatic, gastric CA |
| Previous breast cancer or DCIS | High risk of second primary |
| Family history | First-degree relative significantly increases risk |
| Atypical ductal/lobular hyperplasia | 4-5x increased risk |
| Ethnicity | Ashkenazi Jews, African Americans <45, Native Americans |
- BRCA1 - mostly triple-negative breast cancers
- BRCA2 - associated with cancers of prostate, colon, gallbladder, bile duct, stomach, pancreas
PATHOLOGY - TYPES OF BREAST CANCER
In Situ Carcinomas (pre-invasive)
| Type | Features |
|---|---|
| DCIS (Ductal Carcinoma In Situ) | Confined within ducts; no basement membrane invasion; detected on mammography as microcalcifications; variable risk of progression to invasive cancer |
| LCIS (Lobular Carcinoma In Situ) | AJCC 8th ed. classifies as HIGH-RISK BENIGN LESION, not cancer; bilateral risk marker |
Invasive Carcinomas
| Type | Frequency | Key Features |
|---|---|---|
| Invasive Ductal Carcinoma - NST (No Special Type, formerly scirrhous) | 80% | Most common; hard, irregular mass; desmoplastic reaction; worst prognosis of all types; axillary LN metastases in 25-60% |
| Invasive Lobular Carcinoma | 10% | Often bilateral; multicentric; "Indian file" pattern histologically; subtle on mammography |
| Medullary Carcinoma | 4% | Soft, well-circumscribed, lymphocytic infiltrate; better prognosis |
| Mucinous (Colloid) Carcinoma | 2% | Mucin-secreting; better prognosis; soft, gelatinous |
| Tubular Carcinoma | 2% | Well-differentiated tubular structures; excellent prognosis |
| Papillary Carcinoma | 2% | Papillary fronds; usually elderly women |
| Paget's Disease of the Nipple | Rare | Eczematous nipple eruption; associated with underlying DCIS/invasive cancer; Paget cells (large pale vacuolated cells) in the rete pegs |
| Inflammatory Breast Cancer (IBC) | 1-5% | Peau d'orange + erythema + warmth (no discrete lump); from tumour emboli blocking dermal lymphatics; T4d; worst prognosis |
PATHOGENESIS - WHY SIGNS OCCUR
Tumour mass enlarges in breast parenchyma
↓
Releases growth factors:
- FGF (fibroblast growth factor)
- TGFα / TGFβ
- VEGF
↓
FGF stimulates adjacent fibrocytes → fibroblasts → collagen
(DESMOPLASTIC REACTION = hard, irregular mass)
↓
Collagen contracts → SHORTENS COOPER'S LIGAMENTS
↓
Pulls skin inwards:
Single ligament → DIMPLING
Many ligaments → PUCKERING / TETHERING
Nipple ligaments → NIPPLE RETRACTION
↓
Tumour obstructs dermal lymphatics → PEAU D'ORANGE
(skin oedema - skin over lymphatic pores looks like orange peel)
CLINICAL EXAMINATION OF THE BREAST
Step 1 - History Taking
- Onset, duration, change of lump
- Relationship to menstrual cycle (cyclical = likely benign)
- Nipple discharge (colour: bloody/serous/green/milky)
- Skin changes; pain
- Menstrual history: age at menarche, LMP, regularity
- Reproductive history: parity, age at first birth, breastfeeding
- Hormonal history: OCP use, HRT
- Family history: breast/ovarian/other cancers, affected relatives + age of onset
- Previous biopsies (histological result)
Step 2 - INSPECTION (Patient seated, arms by sides)
| Finding | Significance |
|---|---|
| Asymmetry in size/shape | Tumour causing contour change |
| Skin dimpling/puckering | Cooper's ligament shortening by underlying tumour |
| Skin tethering | Adherence of tumour to skin |
| Peau d'orange | Dermal lymphatic obstruction - locally advanced/inflammatory cancer |
| Erythema | Inflammatory breast cancer vs mastitis/abscess |
| Ulceration/satellite nodules | Advanced disease |
| Nipple inversion (new) | Tumour pulling retromammary tissue - HIGH suspicion |
| Nipple-areola eczema/ulceration | Paget's disease of the breast |
| Nipple discharge (assess) | Blood/serous = malignant until proven otherwise |
| Visible veins | Increased blood supply to tumour |
| Previous scars | Prior surgery |
- Arms raised - better view of lower breast and inframammary fold
- Hands on hips + pectoral muscle contraction - accentuates skin retraction/dimpling from deep tumours attached to Cooper's ligaments
Step 3 - PALPATION OF LYMPH NODES (still seated)
- Axillary nodes - with patient's ipsilateral arm supported by examiner to relax muscles
- Anterior (pectoral): palpate anterior axillary fold
- Posterior (subscapular): posterior axillary fold
- Lateral (humeral): medial arm
- Central: high axilla
- Apical: apex of axilla below clavicle
- Supraclavicular nodes - from behind patient, palpate above clavicle
- Infraclavicular nodes - below clavicle
- Cervical nodes
Step 4 - PALPATION OF BREASTS (patient supine)
- Use flat of the finger pads (not fingertips) in a systematic pattern
- Methods: concentric circles OR radial spokes from nipple OR grid/strip method
- Palpate all 4 quadrants + axillary tail of Spence
- Include the subareolar region (retroareolar area)
- Note: normal breasts have nodularity in the upper outer quadrant, inframammary ridge, and subareolar region - this is NORMAL
| Feature | Benign | Malignant |
|---|---|---|
| Site | Any | UOQ most common (50% of TDLUs) |
| Size | Variable | Variable |
| Shape | Round/oval | Irregular |
| Surface | Smooth | Irregular, lobulated |
| Consistency | Soft/firm | Hard, stony |
| Margins | Well-defined | Poorly defined |
| Mobility | Mobile | Fixed / tethered to skin or deep structures |
| Tenderness | Often tender (fibrocystic) | Usually NON-tender |
| Skin changes | Absent | Dimpling, peau d'orange, ulceration |
| Nipple involvement | Absent | Retraction, discharge |
| Number | Single/multiple | Usually single |
Step 5 - NIPPLE EXAMINATION
- Inversion: Present? Lifelong or new onset?
- Discharge: Elicit by gentle pressure around areola
- Unilateral, single-duct, bloody/serous discharge = HIGH SUSPICION for malignancy or duct ectasia/intraductal papilloma
- Bilateral multiduct milky = galactorrhoea (prolactinoma)
- Green/brown discharge = fibrocystic disease/duct ectasia
Summary: Signs of Malignancy on Examination
| Sign | What it means |
|---|---|
| Hard, irregular, poorly defined lump | Desmoplastic reaction |
| Skin dimpling/tethering | Cooper's ligament shortening |
| Peau d'orange | Dermal lymphatic obstruction |
| Fixed to skin | Direct skin invasion |
| Fixed to chest wall | Pectoralis/chest wall involvement |
| Nipple retraction (new) | Tumour pulling nipple inward |
| Paget's nipple (eczematous) | Underlying DCIS |
| Palpable hard axillary nodes | Lymph node metastasis |
| Supraclavicular nodes | N3 disease |
INVESTIGATIONS - TRIPLE ASSESSMENT
| Component | Method |
|---|---|
| 1. Clinical | History + physical examination |
| 2. Imaging | Mammography ± Ultrasound ± MRI |
| 3. Pathology | Core needle biopsy (CNB) / Fine needle aspiration cytology (FNAC) |
Imaging
- Views: Cranio-caudal (CC) + Mediolateral oblique (MLO)
- Features suggesting malignancy:
- Spiculated/stellate mass (irregular radiating margins)
- Microcalcifications (clustered/pleomorphic = DCIS)
- Asymmetric density
- Architectural distortion
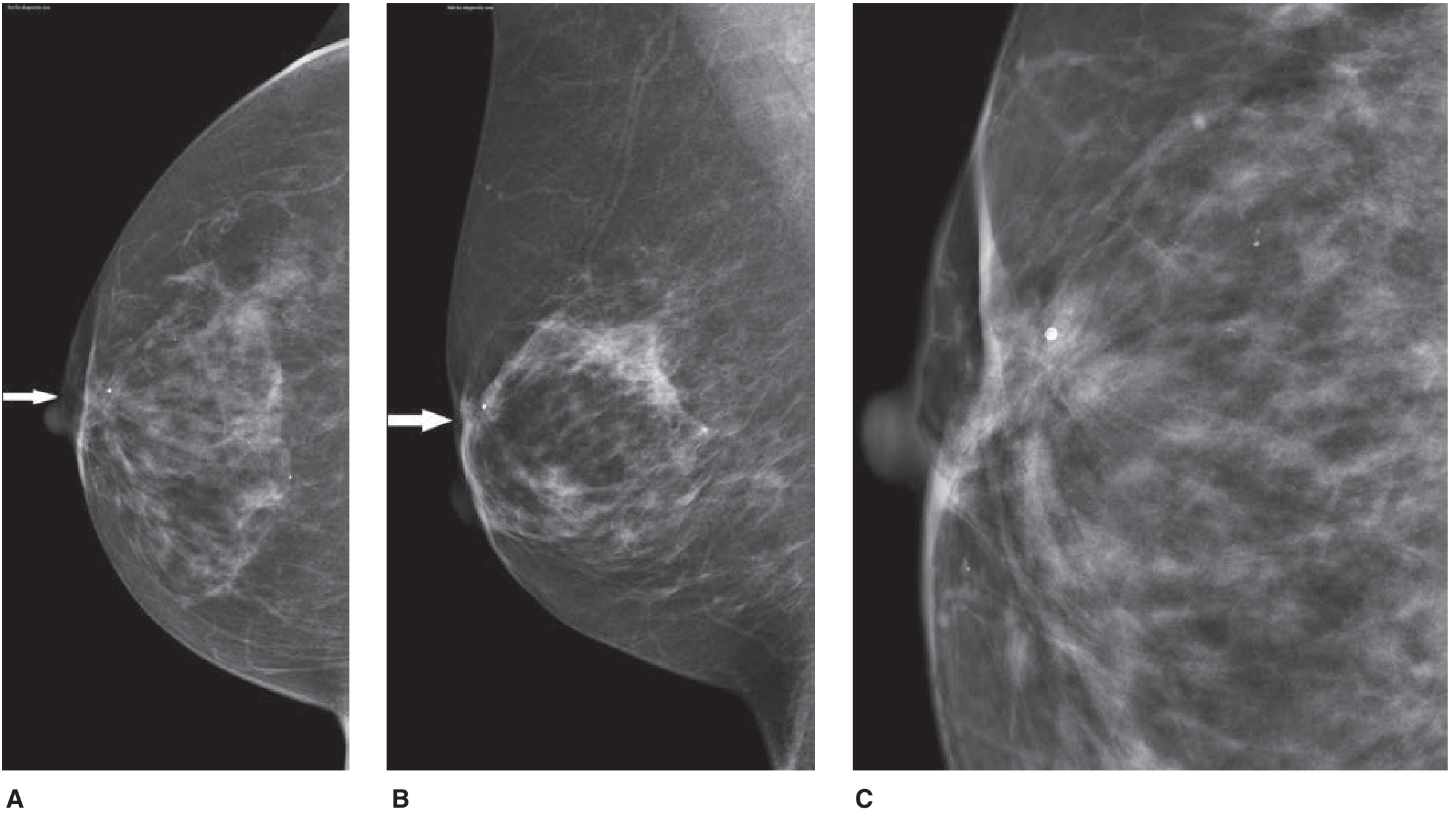
- Women <35 = dense breasts → start with USS rather than mammography
- For younger women (<35-40), pregnant women, or to characterise mammographic lesions
- Distinguishes solid from cystic lesions
- Features suggesting malignancy: irregular hypoechoic mass, spiculated margins, posterior acoustic shadowing, taller-than-wide shape
- For BRCA1/2 carriers (annual screening from age 30)
- Pre-operative staging: multifocal/multicentric disease assessment
- Post-lumpectomy - assess margins
- NOT first-line for all patients
- Core needle biopsy (CNB) - preferred; provides histology, receptor status (ER, PR, HER2), grade
- FNAC - cytology only; quicker but no architecture
- Vacuum-assisted biopsy for microcalcifications
MOLECULAR SUBTYPES (Receptor Status)
| Subtype | ER | PR | HER2 | Features/Treatment |
|---|---|---|---|---|
| Luminal A | + | + | - | Best prognosis; Hormonal therapy (tamoxifen/aromatase inhibitor) |
| Luminal B | + | ± | ± | Intermediate prognosis; chemo + hormonal |
| HER2-enriched | - | - | + | Aggressive; Trastuzumab (Herceptin) + chemo |
| Triple Negative (TNBC) | - | - | - | Worst prognosis; No targeted therapy; chemotherapy only; BRCA1-associated |
STAGING - AJCC TNM 8TH EDITION
T - Primary Tumour
| Stage | Description |
|---|---|
| Tis | DCIS (in situ) |
| T1mi | ≤1 mm |
| T1a | >1 mm - ≤5 mm |
| T1b | >5 mm - ≤10 mm |
| T1c | >10 mm - ≤20 mm |
| T2 | >20 mm - ≤50 mm |
| T3 | >50 mm |
| T4a | Extension to chest wall |
| T4b | Skin: ulceration, satellite nodules, peau d'orange |
| T4c | T4a + T4b |
| T4d | Inflammatory carcinoma |
N - Lymph Nodes
| Stage | Description |
|---|---|
| N0 | No nodes |
| N1 | Movable ipsilateral Level I-II axillary nodes |
| N2 | Fixed/matted Level I-II axillary nodes; or internal mammary nodes without axillary |
| N3 | Level III axillary (infraclavicular), internal mammary + axillary, or supraclavicular nodes |
M - Metastases
- M0 = No distant mets
- M1 = Distant mets
Overall Stage Groups
| Stage | Description | 5-Year Survival |
|---|---|---|
| Stage 0 | DCIS | ~99% |
| Stage I | T1 N0 | ~95-100% |
| Stage II | T2-T3 N0 or T1-T2 N1 | ~70-85% |
| Stage III | T3 N1, T4 any N, any T N2/N3 | ~40-60% |
| Stage IV | Any T, any N, M1 (metastatic) | ~20-25% |
METASTATIC SPREAD
- Axillary nodes - main pathway (lateral and upper outer tumours)
- Internal mammary nodes - inner half tumours
- Supraclavicular nodes - N3 disease
- Contralateral axilla (via subdermal or retrosternal lymphatics)
- Bone - lumbar vertebrae > neck of femur > thoracic vertebrae > ribs > skull
- Mostly osteolytic (can be osteosclerotic or mixed)
- In limbs: only above elbow and above knee (haematopoietic marrow distribution)
- Liver
- Lungs
- Brain
- Adrenal glands, ovaries
At tumour size 1-2 mm (10⁵ cells), neoangiogenesis begins - marks onset of rapid growth and metastatic potential
TREATMENT
Multimodal Approach - MDT Including:
Neoadjuvant Systemic Therapy (NAST) - before surgery
- Locally advanced cancer (T3, T4, N2/N3) - to downsize
- Early cancer: to enable BCS; HER2+ tumours; TNBC; premenopausal; node-positive
- NACT (neoadjuvant chemotherapy)
- Neoadjuvant targeted therapy - Trastuzumab + Pertuzumab for HER2+ >5 mm
- Neoadjuvant hormonal therapy - elderly/frail ER+/PR+ patients (takes 3-6 months for response)
Surgical Options
A. Breast Surgery
| Procedure | Indication |
|---|---|
| Breast Conservation Surgery (BCS) / Wide Local Excision (WLE) | Small tumours (in proportion to breast size); single focus; patient preference. Aim: no tumour on inked margins for invasive cancer; ≥2 mm clear for DCIS |
| Simple mastectomy | Large/multicentric tumours; diffuse DCIS; patient preference; BRCA+ |
| Modified Radical Mastectomy (MRM) | Mastectomy + Level I-II-III axillary clearance |
| Radical Mastectomy (Halsted) | Historical only; removes pectoralis major + minor - excessive morbidity, no survival benefit |
| Skin-sparing/Nipple-sparing mastectomy | With immediate reconstruction |
| Risk-reducing bilateral mastectomy | BRCA1/2 carriers; reduces risk by ~90% |
B. Axillary Surgery
| Procedure | Indication |
|---|---|
| Sentinel Lymph Node Biopsy (SLNB) | Clinically node-negative: blue dye + radioisotope → first draining node; if negative → no further axillary surgery |
| Axillary Lymph Node Dissection (ALND) | Clinically/pathologically node-positive |
Adjuvant Therapy (after surgery)
| Modality | Indication |
|---|---|
| Radiotherapy | After BCS (whole breast ± boost); after mastectomy for T3/T4 or N+ disease; palliative for bony mets |
| Chemotherapy | HER2+, TNBC, high-grade, node-positive; Regimens: FEC, AC-T (anthracycline + taxane-based) |
| Endocrine/Hormonal therapy | ER+ / PR+ tumours |
| - Premenopausal | Tamoxifen (SERM) 5-10 years |
| - Postmenopausal | Aromatase inhibitors (anastrozole, letrozole) |
| Targeted therapy | HER2+: Trastuzumab (Herceptin) 1 year; Pertuzumab; T-DM1 |
| CDK4/6 inhibitors | Luminal B metastatic HR+ disease (palbociclib, ribociclib) |
| PARP inhibitors | BRCA-mutated TNBC (olaparib) |
| Bisphosphonates | Bone metastases; pain relief; prevention of skeletal events |
Metastatic Disease (Stage IV) - Palliative Intent
- Endocrine therapy preferred for ER+ with bone mets + limited visceral involvement
- Chemotherapy for HR-negative, hormone-refractory, visceral crisis
- Palliative radiotherapy for painful bony mets (weight-bearing: vertebrae, femur)
- Bisphosphonates (zoledronic acid) for bone mets
- Pleural effusions: drain + pleurodesis
- Surgical resection only for solitary visceral mets in fit patients with favourable biology
SCREENING
| Method | Recommendation |
|---|---|
| Mammography | Women 50-69 (or 40-74 depending on guideline): every 2 years |
| MRI | BRCA1/2 carriers: annually from age 30 |
| Clinical breast examination | Part of routine health check |
| Breast self-examination (BSE) | Monthly; not shown to reduce mortality but helps detect interval cancers |
HEREDITARY MANAGEMENT
- Bilateral risk-reducing mastectomy → reduces risk by 90%
- Chemoprophylaxis: Tamoxifen or anastrozole → reduces risk by ~50%
- Bilateral salpingo-oophorectomy at 35-40 years (after completing family) → reduces ovarian CA risk
QUICK EXAM SUMMARY
| Point | Key Fact |
|---|---|
| Most common cancer in women | Breast (25% of all female cancers) |
| Most common site of primary | Upper outer quadrant (50% of TDLUs located there) |
| Most common type | Invasive ductal carcinoma NST (80%) |
| Skin changes cause | Cooper's ligament shortening (desmoplastic reaction) |
| Peau d'orange cause | Dermal lymphatic obstruction |
| Paget's disease | Eczematous nipple + Paget cells + underlying DCIS |
| Inflammatory BC | T4d; peau d'orange without mass; worst prognosis |
| BRCA1 → cancer type | Triple negative breast cancer |
| Triple assessment | Clinical + Imaging + Pathology (sensitivity ~99.6%) |
| Mammography views | CC (cranio-caudal) + MLO (mediolateral oblique) |
| Spiculated mass on mammo | Highly suspicious for malignancy |
| Microcalcifications on mammo | Suggests DCIS |
| First-line imaging <35 years | Ultrasound (dense breasts) |
| Sentinel node biopsy | Clinically node-negative; first draining node with blue dye + isotope |
| Tamoxifen mechanism | SERM - blocks ER in breast tissue (premenopausal) |
| Trastuzumab target | HER2/neu receptor (ErbB2) |
| Radical Halsted mastectomy | Historical; removes pec major + minor; NO survival benefit |
| BRCA risk reduction surgery | Bilateral mastectomy reduces risk by 90% |
| Bone mets: most common site | Lumbar vertebrae |
| Osteolytic vs osteosclerotic | Mostly osteolytic in breast cancer |
Hematemesis cc 101
HEMATEMESIS 101 - COMPREHENSIVE GUIDE
DEFINITIONS
| Term | Definition |
|---|---|
| Hematemesis | Vomiting of fresh/bright red blood - indicates ACTIVE, brisk upper GI bleeding |
| Coffee-ground emesis | Dark, coffee-ground vomitus - blood oxidised by gastric acid = bleeding has slowed or stopped |
| Melaena | Black, tarry, foul-smelling stool - degraded blood in the GI tract (needs ~50-100 mL blood to turn stool black) |
| Haematochezia | Fresh/maroon blood per rectum - typically LOWER GI bleeding; but can occur with massive UGIB (>1000 mL at a rapid rate) |
- UPPER GI = proximal to the Ligament of Treitz (duodenojejunal flexure)
- LOWER GI = distal to the Ligament of Treitz
EPIDEMIOLOGY
- Incidence: >100 per 100,000 population/year in Western countries; increases with age
- In-hospital mortality: 5-10%; rises to 33% when bleeding first occurs in patients already hospitalised for another condition
- Strongly associated with NSAID use
- UGIB accounts for up to 150 hospital admissions per 100,000 per year
CAUSES OF UPPER GI BLEEDING
Frequency Table (Bailey and Love)
| Cause | Frequency |
|---|---|
| Peptic ulcers (total) | 60% |
| - Duodenal ulcer | 33% |
| - Gastric ulcer | 21% |
| - Oesophageal ulcer | 6% |
| Erosions (total) | 26% |
| - Oesophageal | 13% |
| - Gastric | 9% |
| - Duodenal | 4% |
| Mallory-Weiss tear | 4% |
| Oesophageal varices | 4% |
| Tumour | 0.5% |
| Vascular lesions (Dieulafoy, AVM) | 0.5% |
| Others | 5% |
Full Causes List - Mnemonic: "PEPTIC VOMIT"
| Cause | Key Points |
|---|---|
| Peptic ulcer disease | Most common; H. pylori + NSAIDs; posterior duodenal ulcer bleeds from gastroduodenal artery |
| Erosions | Oesophagitis, gastritis, duodenitis - acute stress ulcers (Curling's ulcer = burns; Cushing's ulcer = head injury) |
| Portal hypertension / Varices | Oesophageal varices (most common portal cause); gastric varices |
| Tear - Mallory-Weiss | Mucosal tear at gastro-oesophageal junction from forceful retching/vomiting |
| Inflammatory / IBD | Crohn's involving upper GI |
| Carcinoma | Gastric cancer, oesophageal cancer; blood often darker |
| Vascular lesions | Dieulafoy's lesion (large submucosal artery), AVM, gastric antral vascular ectasia (GAVE/"watermelon stomach"), hereditary haemorrhagic telangiectasia |
| Other | Aortoenteric fistula (post-aortic graft - HERALD bleed before massive bleed), Haemobilia, Haemosuccus pancreaticus |
| Medications | NSAIDs, anticoagulants, steroids, SSRIs |
| Iatrogenic | Post-ERCP, post-sphincterotomy, post-polypectomy |
| Trauma | Oesophageal perforation (Boerhaave's), nasogastric tube trauma |
PATHOPHYSIOLOGY OF KEY CAUSES
1. Peptic Ulcer Bleeding
- H. pylori (prevalence 80%+ developing countries; 20-50% industrialised) → antral-predominant gastritis → duodenal ulcers
- NSAIDs → inhibit COX-mediated prostaglandin synthesis → impaired mucosal protection
- Pathology: 96% of surgically resected bleeding ulcers have an underlying artery (50% protruding above ulcer surface, 50% clot overlying breach in vessel wall)
- Deep posterior duodenal ulcer → erodes into gastroduodenal artery → exsanguinating haemorrhage
2. Mallory-Weiss Tear
- Mucosal (NOT full thickness) tear at the gastro-oesophageal junction
- Caused by sudden increase in intra-abdominal pressure: forceful retching/vomiting, coughing, lifting, pregnancy, trauma, bowel prep
- Extends distally into hiatal hernia sac (if present)
- Usually single tear, starts at GEJ
- Bleeding is typically self-limiting in 90% of cases
- Heals within 24-48 hours
- Contrast with Boerhaave's syndrome (full-thickness oesophageal rupture) - surgical emergency
3. Oesophageal Varices
- Portal hypertension (most commonly from liver cirrhosis) → portosystemic shunting → oesophageal submucosal veins dilate
- Variceal rupture triggered by: increased portal pressure, variceal size, bacterial infection (spontaneous bacterial peritonitis)
- High mortality - each bleed: 20-30% mortality
CLINICAL PRESENTATION
History
- Character of vomit: Bright red (active, brisk) vs coffee-ground (slower/stopped bleeding)
- Amount and frequency
- NSAID / aspirin / anticoagulant / steroid use
- Alcohol use / liver disease (suggests varices)
- Preceding nausea and retching before haematemesis (suggests Mallory-Weiss)
- History of peptic ulcer disease (PUD), heartburn, epigastric pain
- Previous similar episodes, previous endoscopy
- Melaena (suggests upper GI source; blood in GI tract >6 hours)
- Dysphagia, weight loss, anorexia (malignancy)
- Family history of GI cancer or polyposis
Symptoms of Haemodynamic Compromise (blood loss)
| Blood Loss | % Volume Lost | Symptoms/Signs |
|---|---|---|
| <750 mL | <15% | Minimal symptoms; mild anxiety |
| 750-1500 mL | 15-30% | Tachycardia, anxiety, mild hypotension |
| 1500-2000 mL | 30-40% | Tachycardia >120, hypotension, confusion |
| >2000 mL | >40% | BP <90, severely confused/unconscious - Class IV = EXSANGUINATION |
EXAMINATION
General
- Pallor (anaemia)
- Jaundice / stigmata of chronic liver disease - if varices suspected: spider naevi, palmar erythema, gynaecomastia, caput medusae, hepatosplenomegaly, asterixis (hepatic encephalopathy), parotid enlargement, Dupuytren's contracture, leukonychia
- Alcohol smell
- Peripheral access availability
Vital Signs (Shock Assessment)
- Pulse rate (tachycardia >100 bpm = significant blood loss)
- Blood pressure (systolic <100 = haemodynamic compromise)
- Postural hypotension - BP drop >20 mmHg on standing = significant haemorrhage
- Respiratory rate, GCS, urine output (oliguria = end-organ hypoperfusion)
Abdomen
- Epigastric tenderness - peptic ulcer
- Hepatomegaly/splenomegaly - portal hypertension
- Ascites - cirrhosis
- Rectal examination - confirm melaena vs haematochezia; assess for anorectal sources
INVESTIGATIONS
Immediate (A-E assessment simultaneously)
| Investigation | Purpose |
|---|---|
| FBC | Haemoglobin (may not drop acutely - haemodilution takes time), WCC, platelets |
| U&E / Creatinine | Urea:Creatinine ratio >100 suggests UGIB (protein from luminal blood absorbed) |
| LFTs | Liver disease, coagulopathy |
| Coagulation (PT/INR, APTT) | Anticoagulation, liver disease |
| Group and crossmatch | Prepare for transfusion |
| ABG | Acidosis = poor tissue perfusion |
| ECG | Cardiac stress from blood loss |
| Chest X-ray | Perforation (free air under diaphragm) if bowel sounds absent |
Definitive Investigation
- Diagnostic AND therapeutic
- Timing:
- Severe/ongoing bleeding: immediate OGD
- Stabilised patients with mild bleeding: next morning (guided by local policy)
- No evidence for IV PPI prior to endoscopy (does not improve outcomes)
RISK STRATIFICATION SCORES
A. Glasgow-Blatchford Score (GBS) - PRE-ENDOSCOPY
| Variable | Points |
|---|---|
| BUN ≥6.5 mmol/L | 2-6 |
| Haemoglobin <130 g/L (men) | 1-6 |
| Haemoglobin <120 g/L (women) | 1-6 |
| Systolic BP <110 mmHg | 2-3 |
| Pulse ≥100 bpm | 1 |
| Melaena | 1 |
| Syncope | 2 |
| Hepatic disease | 2 |
| Cardiac failure | 2 |
- GBS = 0 → safe for outpatient management (very low risk)
- GBS ≥6 → 50% likelihood of requiring treatment (high risk)
- Range: 0-23; higher = higher risk
B. Rockall Score - PRE + POST-ENDOSCOPY - Predicts rebleeding and mortality
| Variable | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Age | <60 | 60-79 | ≥80 | - |
| Shock | HR <100, SBP ≥100 | HR >100 | SBP <100 | - |
| Comorbidity | None | - | IHD, CCF, other major illness | Renal failure, liver failure, metastatic cancer |
| Endoscopic diagnosis | Mallory-Weiss / no lesion | PUD, erosions, oesophagitis | UGI malignancy | - |
| Stigmata of haemorrhage | Clean base, flat pigmented spot | - | Blood/active bleeding/visible vessel/adherent clot | - |
- Clinical Rockall score = Age + Shock + Comorbidity (pre-endoscopy)
- Clinical Rockall 0 = 0% mortality
- Complete Rockall ≤2 = low risk; safe early discharge
- Complete Rockall 5 = ~10% mortality
- Complete Rockall ≥8 = ~40% mortality
C. Forrest Classification - Endoscopic stigmata of bleeding peptic ulcer
| Forrest Class | Appearance | Rebleed Risk | Management |
|---|---|---|---|
| Ia | Active spurting arterial bleed | 55-90% | Urgent endoscopic therapy |
| Ib | Active oozing | 10-27% | Endoscopic therapy |
| IIa | Visible vessel (non-bleeding) | 43-51% | Endoscopic therapy |
| IIb | Adherent clot | 22-36% | Endoscopic therapy (remove clot, treat base) |
| IIc | Flat pigmented haematin spot | 5-10% | Conservative |
| III | Clean-based ulcer | 0-2% | Conservative / safe discharge |
MANAGEMENT
Step 1 - RESUSCITATION (ABCDE - simultaneous with assessment)
- Airway - protect airway in obtunded/actively vomiting patients; consider intubation before OGD if haematemesis with altered GCS
- 2 large-bore IV cannulae (≥16G) or central venous access
- IV fluids - isotonic crystalloid (NS or Hartmann's) for immediate resuscitation
- Blood transfusion - trigger: Hb <7 g/dL (target Hb 7-9 g/dL); higher threshold (Hb <8-9) in patients with coronary artery disease; >30% blood volume loss is a transfusion indication
- RESTRICTED transfusion strategy in variceal bleeding reduces rebleeding and mortality (Harrison's)
- Correct coagulopathy - FFP for elevated PT/INR (especially liver disease, anticoagulants); platelets if <50
- Urinary catheter - monitor urine output (target >0.5 mL/kg/hr)
- CVP monitoring - for severe bleeding
Step 2 - PHARMACOLOGICAL THERAPY
| Drug | Indication | Rationale |
|---|---|---|
| IV PPI (omeprazole 80 mg bolus then 8 mg/hr infusion) | After endoscopic haemostasis for PUD | Prevents re-bleeding; acid suppression promotes clot stability |
| Octreotide/Somatostatin | Variceal bleeding | Reduces splanchnic blood flow and portal pressure |
| Terlipressin | Variceal bleeding | Vasoconstrictor; reduces portal pressure |
| Prophylactic antibiotics (ceftriaxone) | Variceal bleeding / cirrhosis | Reduces SBP, recurrent bleeding, and mortality - start before endoscopy |
| Tranexamic acid | UGIB | Anti-fibrinolytic; meta-analysis suggests reduction in overall mortality |
| H. pylori eradication | Confirmed H. pylori + PUD | After index bleed; prevents recurrence |
Step 3 - ENDOSCOPIC THERAPY (OGD)
- Immediate OGD for: haemodynamic instability, suspected varices, ongoing active bleeding
- Within 24 hours for stable patients
- Adrenaline injection (1:10,000) - slows bleeding; never used alone (high re-bleed rate)
- Thermal coagulation - heater probe, multipolar electrocoagulation (MPEC)
- Haemoclip - mechanical occlusion of vessel
- Best evidence: Combination of adrenaline injection + haemoclip and/or heater probe
- Therapeutic endoscopy achieves haemostasis in ~70% of cases
- Endoscopic Variceal Ligation (EVL) / Band ligation - first-line for oesophageal varices
- Endoscopic sclerotherapy - injection of sclerosant (ethanolamine oleate) - second-line
- Gastric varices: tissue glue (cyanoacrylate) injection or thrombin
- Active bleeders: haemoclips (first-line) or adrenaline injection + MPEC
- Spontaneously stops in ~90%
Step 4 - ANGIOGRAPHIC INTERVENTION (if endoscopy fails)
- Mesenteric angiography → selective catheterisation → transcatheter arterial embolisation (TAE)
- Valuable alternative to surgery in expert centres
- Celiac axis + SMA angiograms (with CO2 or iodinated contrast)
- Can identify bleeding at rates >0.5 mL/min
- Prophylactic embolisation of gastroduodenal artery for duodenal ulcer bleeding
Step 5 - SURGICAL INTERVENTION
- Persistent bleeding despite 2 attempts at endoscopic haemostasis
- Haemodynamic instability with ongoing bleeding
- Rebleeding after endoscopy
- Transfusion requirement >6 units of RBC
- Frail/elderly patients should have EARLY surgery (paradox: they are more likely to die from bleeding, not surgery)
- Oversewing/underrunning alone - emergency damage control; ligate GDA with 3-point U-stitch (superior, inferior, pancreatic branch)
- Oversewing + vagotomy and pyloroplasty (V+D) - reduces acid secretion
- Vagotomy and antrectomy (V+A) - lowest rebleed rate but higher morbidity
Kocher manoeuvre is performed FIRST at surgery - mobilises duodenum to allow posterior approach and manual compression of GDA from behind.
- Longitudinal duodenotomy/pyloroduodenotomy
- Expose ulcer (usually posterior/superior)
- Under-run the bleeding vessel with heavy sutures (U-stitch/figure-of-8) in ulcer base
- Close pylorotomy transversely (Heineke-Mikulicz)
- If large ulcer destroys first part of duodenum: distal gastrectomy with Roux-en-Y
- Anterior gastrotomy → underrun vessel → biopsy ulcer margins (exclude malignancy) → local excision if feasible
- TIPS (Transjugular Intrahepatic Portosystemic Shunt) - decompresses portal system
- Complication: encephalopathy in up to 20%
- Used as bridge to transplantation
- Balloon tamponade (Sengstaken-Blakemore tube or Minnesota tube) - temporary bridge to definitive therapy
- Inflates oesophageal + gastric balloons to compress varices
- MAX 24 hours (risk of oesophageal necrosis/rupture)
- Surgical shunts (Warren selective splenorenal shunt) - rarely used
SPECIFIC CONDITIONS IN DETAIL
Stress Ulceration
- ICU patients with major illness/injury/surgery
- Incidence reduced by enteral nutrition and prophylactic PPI/H2 blockers
- Curling's ulcer = burns; Cushing's ulcer = raised ICP/head injury (vagal stimulation)
Dieulafoy's Lesion
- Large, tortuous submucosal artery (usually left gastric artery branch) erodes through mucosa
- Tiny mucosal defect with MASSIVE, recurrent, arterial bleeding
- Location: within 6 cm of GEJ, on lesser curve
- Diagnosis: endoscopy (may be missed if not actively bleeding); can require repeated OGDs or angiography
- Treatment: endoscopic haemoclip or band ligation
Aortoenteric Fistula
- After aortic graft surgery → fistula between aortic graft and duodenum (3rd/4th part)
- Presents with herald bleed (small self-limiting haematemesis/melaena) before catastrophic exsanguinating haemorrhage
- Diagnosis: CT angiography; OGD (blood in D3/D4)
- Treatment: emergency vascular surgery
Haemobilia
- Bleeding into biliary tract → blood exits via ampulla of Vater
- Causes: trauma (most common - hepatic artery pseudoaneurysm), liver biopsy, ERCP, hepatic artery aneurysm
- Quincke's triad: haemobilia + obstructive jaundice + RUQ colic
- Diagnosis: OGD (blood from ampulla); angiography
- Treatment: hepatic artery embolisation
VARICEAL BLEEDING ALGORITHM
Acute variceal bleed
↓
Resuscitate:
- Hb target 7-9 g/dL (RESTRICTED strategy)
- FFP only if evidence of coagulopathy
- DO NOT correct PT with FFP routinely
↓
Pharmacology (BEFORE endoscopy):
- Octreotide / Terlipressin IV
- Prophylactic antibiotics (ceftriaxone IV)
↓
Urgent OGD + Band ligation (EVL)
↓
┌──────────────────────┐
Controlled Failed
↓ ↓
Prevention: Balloon tamponade
- Repeated EVL (Sengstaken-Blakemore)
until obliterated ↓
- Non-selective BB TIPS
(propranolol/ ↓
carvedilol) Consider transplant
evaluation (Child's B/C)
PEPTIC ULCER DISEASE - MANAGEMENT OVERVIEW
Medical (Non-bleeding)
- H. pylori eradication - Triple therapy: PPI + amoxicillin + clarithromycin x 7-14 days
- PPI (omeprazole, lansoprazole) - long-term if NSAID cannot be stopped
- Stop NSAIDs if possible
Surgical Indications for PUD (4 Cs):
- Continuous/persistent bleeding despite medical and endoscopic therapy
- Complications - perforation, obstruction
- Cancer exclusion for gastric ulcer
- Can't comply with medical therapy / recurrent despite treatment
SUMMARY TABLE - QUICK EXAM POINTS
| Key Fact | Answer |
|---|---|
| Most common cause of UGIB | Peptic ulcer disease (60%) |
| Urea:creatinine ratio in UGIB | >100 (blood protein absorption from gut) |
| Anatomical landmark UGIB vs LGIB | Ligament of Treitz |
| Cause of Mallory-Weiss | Forceful retching/vomiting → tear at GEJ |
| Forrest Ia | Active spurting arterial bleed - highest rebleed risk |
| Safe discharge Rockall score | ≤2 (complete) or 0 (clinical) |
| Transfusion trigger | Hb <7 g/dL (target 7-9 g/dL) |
| Endoscopic haemostasis rate | ~70% for PUD |
| Surgery threshold | >6 units RBC transfused, rebleed after endoscopy |
| Surgical approach to DU | Pyloroduodenotomy + underrun vessel (U-stitch) + Heineke-Mikulicz closure |
| Kocher manoeuvre | Mobilises duodenum - allows GDA control |
| Dieulafoy's lesion | Large submucosal artery, within 6 cm of GEJ, massive bleed from tiny defect |
| Haemobilia triad | Quincke's triad: haemobilia + jaundice + RUQ colic |
| Aortoenteric fistula warning sign | Herald bleed before catastrophic haemorrhage |
| Varices: pre-endoscopy drug | Terlipressin or octreotide + ceftriaxone antibiotics |
| Varices: endoscopic treatment | EVL (band ligation) first-line |
| Varices: failed endoscopy | TIPS |
| Sengstaken-Blakemore tube | Bridge to TIPS; max 24 hours use |
| Stress ulcer: Curling's vs Cushing's | Curling's = burns; Cushing's = head injury |
| UGIB mortality | 5-10% overall; 33% if bleeding occurs in hospitalised patients |
Upper gi bleeding 101
- ✅ Definition + anatomical landmark (Ligament of Treitz)
- ✅ Epidemiology (>100/100,000/year, 5-10% mortality)
- ✅ Full causes table with frequencies (PUD 60%, erosions 26%, Mallory-Weiss 4%, varices 4%)
- ✅ Pathophysiology of PUD, Mallory-Weiss, oesophageal varices
- ✅ Clinical presentation + haemodynamic shock classification
- ✅ Examination (stigmata of liver disease, postural hypotension)
- ✅ Investigations (Urea:Creatinine ratio, FBC, coags, crossmatch)
- ✅ Glasgow-Blatchford Score (pre-endoscopy triage)
- ✅ Rockall Score (complete with table + mortality thresholds)
- ✅ Forrest Classification (Ia → III with rebleed % and management)
- ✅ Management stepwise: Resuscitation → Pharmacology → OGD → Angioembolisation → Surgery
- ✅ Surgical technique for bleeding DU (Kocher, pyloroduodenotomy, U-stitch, Heineke-Mikulicz)
- ✅ Variceal algorithm (octreotide/terlipressin + ceftriaxone → EVL → TIPS → transplant evaluation)
- ✅ Special conditions: Dieulafoy's, aortoenteric fistula, haemobilia, stress ulcers
- Non-variceal vs variceal UGIB - side-by-side comparison
- H. pylori - pathogenesis, diagnosis and eradication regimens in depth
- Portal hypertension - pathophysiology, Child-Pugh/MELD scoring, TIPS procedure
- Acute management OSCE/exam station - step-by-step clinical approach script
- Lower GI bleeding - as the complementary topic
Burns 101
BURNS 101 - COMPREHENSIVE GUIDE
DEFINITION AND EPIDEMIOLOGY
- Burns are a leading cause of accidental death worldwide
- Scald injuries (hot liquids) are most common in children <2 years (accidental or non-accidental)
- Flame burns are more common in teenagers and adults
- Children have thinner skin → more severe burns from same thermal exposure; larger BSA-to-mass ratio → greater insensible fluid losses
- Inhalation injury has now become the main cause of mortality in burn patients as resuscitation has improved
TYPES OF BURNS BY AETIOLOGY
| Type | Common Causes | Key Features |
|---|---|---|
| Thermal | Flame, scald (most common), contact (hot objects) | Depth depends on temperature × duration / blood flow |
| Chemical | Acids, alkalis, industrial solvents | Alkalis (e.g. NaOH) cause liquefactive necrosis → deeper; Acids cause coagulative necrosis → self-limiting |
| Electrical | Low voltage (<1000V), High voltage (>1000V), Lightning | Entry + exit wounds; internal deep tissue injury > external appearance; arrhythmia, rhabdomyolysis |
| Radiation | Sunburn (UV), radiotherapy, nuclear | Usually superficial except nuclear/radiation therapy |
| Friction | Road rash, rope burn | Mixed abrasion + thermal |
BURN DEPTH CLASSIFICATION
Depth of injury = Temperature × Duration
─────────────────────
Blood Flow
| Degree | Old Name | Layers Involved | Appearance | Sensation | Blisters | Healing |
|---|---|---|---|---|---|---|
| Superficial (1st degree) | Superficial | Epidermis only | Red, dry, no blisters | Painful, hyperaesthetic | None | <7 days, NO scar |
| Superficial partial-thickness (2nd degree superficial) | Superficial dermal | Epidermis + papillary dermis | Red, moist, blanches on pressure | Very painful | YES | <14 days, minimal scar |
| Deep partial-thickness (2nd degree deep) | Deep dermal | Epidermis + reticular dermis | Pale/mottled, does NOT blanch | Reduced sensation (nerve endings damaged) | May be present | 14-21 days, significant scarring; may need grafting |
| Full thickness (3rd degree) | Full thickness | Entire skin + ± subcutaneous fat | White/grey/black, leathery, dry | PAINLESS (nerve endings destroyed) | None | Cannot self-heal (except from margins); ALWAYS needs grafting |
| 4th degree | Deep/subdermal | Skin + muscle, tendon, bone | Charred, black | None | None | Amputation/complex reconstruction |
- Superficial burns = NOT included in TBSA% calculation (only partial + full thickness)
- Scalds → usually partial thickness
- Clothes catching fire → usually full thickness
- Wounds healing in <14 days = no significant scar
- Wounds healing in 14-21 days = some scarring
- Wounds taking >21 days = deep dermal/full thickness → unacceptable scarring → surgery
ESTIMATION OF BURN SIZE - % TBSA
Rule of Nines (Adults)
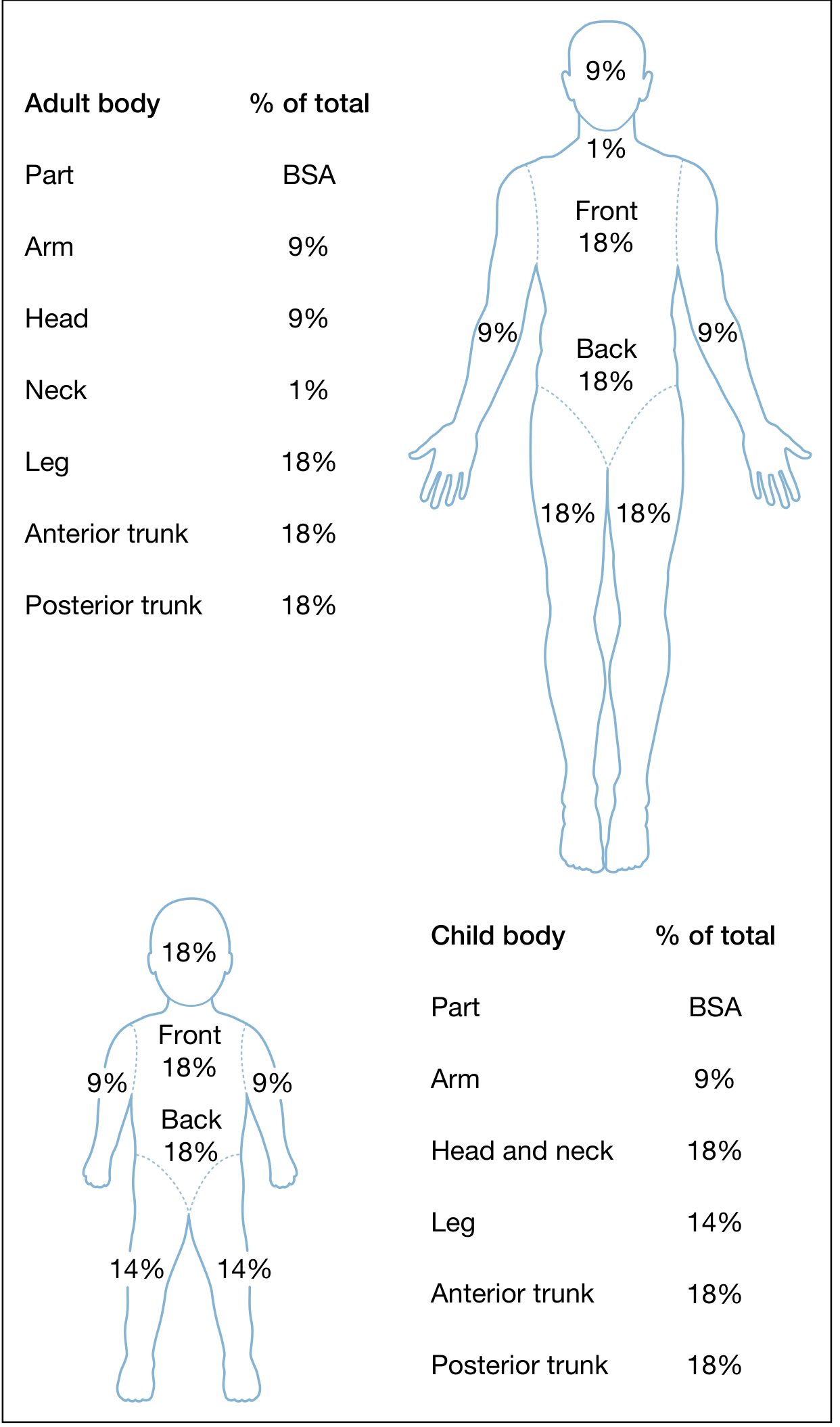
| Body Part | Adult | Child |
|---|---|---|
| Head | 9% | 18% (head + neck) |
| Neck | 1% | (included above) |
| Each arm | 9% | 9% |
| Anterior trunk | 18% | 18% |
| Posterior trunk | 18% | 18% |
| Each leg | 18% | 14% |
| Genitalia/perineum | 1% | 1% |
| TOTAL | 100% | 100% |
Why different in children? Head is proportionately larger; lower limbs proportionately smaller.
Lund and Browder Chart
- More accurate than Rule of Nines, especially in children
- Accounts for age-related body proportion changes (Berkow formula)
Palm Method
- Patient's palm (fingers together) = approximately 1% TBSA in all ages
- Useful for scattered/irregular burns
INITIAL ASSESSMENT - ATLS APPROACH
Primary Survey
- Signs of inhalation injury requiring immediate intubation:
- Full-thickness burns of face/perioral area
- Circumferential neck burns
- Acute respiratory distress / stridor
- Progressive hoarseness or air hunger
- Carbonaceous (sooty) sputum
- Supraglottic oedema on bronchoscopy
- Respiratory depression / altered GCS
- Delay leads to progressive oedema → loss of airway → cannot intubate
- Fibreoptic bronchoscopy = gold standard if uncertain
- Cover burn with DRY sheet during primary survey; defer debridement
- 100% humidified oxygen by non-rebreather mask for ALL suspected inhalation injury
- CO poisoning falsely elevates SpO2 on pulse oximetry → ABG with carboxyhaemoglobin mandatory
- Circumferential chest burns → restrict chest wall expansion → may need escharotomy
- 2 large-bore IV cannulae (ideally through unburnt skin - but can be placed through burns if necessary)
- Urinary catheter (monitor urine output)
- Target UO: 0.5 mL/kg/hr (adults and children >30 kg)
- Target UO: 1 mL/kg/hr (children <30 kg)
- Check for circumferential limb burns → compartment syndrome
INHALATION INJURY
- Closed-space fires
- Decreased mentation (alcohol, drugs, head injury, overdose)
Three Components of Inhalation Injury
| Level | Mechanism | Presentation | Timing |
|---|---|---|---|
| Carbon monoxide (CO) poisoning | CO binds haemoglobin (250x affinity of O2) → tissue hypoxia | Headache, confusion, cherry-red skin, coma; SpO2 falsely NORMAL | Immediate |
| Upper airway thermal injury | Direct heat → mucosal oedema above cords | Stridor, hoarseness, facial burns | Rapidly progressive (hours) |
| Lower airway/parenchymal injury | Toxic gases + particulates → bronchospasm, mucosal sloughing, ARDS | Bronchospasm, wheeze, ARDS; may not be evident for 24 hours | Delayed |
CO Poisoning
- SpO2 probe CANNOT detect CO - always get ABG
- Treatment: 100% oxygen (displaces CO from haemoglobin - half-life reduced from 5h → 60-90 min)
- Consider hyperbaric oxygen for severe CO poisoning (GCS <8, pregnant patients, cardiac involvement)
Cyanide Poisoning
- From combustion of nitrogen-containing polymers: wool, silk, polyurethane, vinyl
- Binds cytochrome oxidase → uncouples oxidative phosphorylation → histotoxic hypoxia
- Suspect when: profound metabolic acidosis + high lactate + low response to O2
- Treatment: hydroxocobalamin (Cyanokit) IV; sodium thiosulfate
Diagnosis of Inhalation Injury
- History: enclosed-space fire, LOC at scene
- Signs: facial burns, singed nasal hair, soot in mouth/nose, hoarseness, carbonaceous sputum, expiratory wheeze
- ABG + carboxyhaemoglobin levels
- CXR (may be normal initially)
- Bronchoscopy - direct visualisation (gold standard)
FLUID RESUSCITATION - PARKLAND FORMULA
When to start?
- Burns >15-20% TBSA in adults, >10% TBSA in children
Parkland Formula (Baxter Formula)
Total 24-hour fluid = 4 mL × Weight (kg) × %TBSA burned
- Fluid used: Hartmann's solution (Lactated Ringer's) - crystalloid
- Count only 2nd and 3rd degree burns (not superficial/1st degree burns) in TBSA calculation
Administration Schedule
| Time Period | Volume |
|---|---|
| First 8 hours (from TIME OF BURN, not time of arrival) | Half of 24-hour total |
| Next 16 hours | Remaining half |
Critical point: the 8 hours is counted from time of injury, not from time of arrival at hospital. If a patient arrives 3 hours after the burn, the first 8 hours worth of fluid must be delivered in the remaining 5 hours.
Worked Example
- 70 kg adult with 40% TBSA burns
- Total = 4 × 70 × 40 = 11,200 mL
- First 8 hours = 5,600 mL (700 mL/hr)
- Next 16 hours = 5,600 mL (350 mL/hr)
Monitoring Adequacy
- Urine output (primary guide): 0.5 mL/kg/hr adults; 1 mL/kg/hr children
- Heart rate, blood pressure, mental status
- Serum lactate (tissue perfusion)
Pitfalls
- Parkland formula = estimate only; titrate to urine output
- Can lead to over-resuscitation ("fluid creep") → abdominal compartment syndrome, pulmonary oedema
- Do NOT forget to add maintenance fluids (especially in children)
- Children also need dextrose-containing maintenance fluid alongside Parkland resuscitation (to prevent hypoglycaemia)
Modified Brooke Formula (alternative)
2 mL × Weight (kg) × %TBSA = 24-hour crystalloid
Paediatric addition
- Add 5% dextrose in 0.45% NaCl at maintenance rate alongside Parkland formula
- Monitor glucose closely
BURN CENTRE REFERRAL CRITERIA (American Burn Association)
- Partial-thickness burns >10% TBSA
- Burns involving face, hands, feet, genitalia, perineum, or major joints
- Full-thickness burns of any age
- Electrical burns
- Chemical burns
- Inhalation injury
- Burns with preexisting medical comorbidities
- Burns with concomitant trauma where burn poses greater risk
- Burned children in hospitals without appropriate paediatric facilities
- Burns requiring specialised social/emotional/rehabilitative intervention
WOUND MANAGEMENT
Topical Antimicrobial Agents
| Agent | Spectrum | Advantages | Disadvantages |
|---|---|---|---|
| Silver sulfadiazine 1% (SSD) | Broad spectrum (Gram+, Gram-, Candida) | Most widely used; painless; good infection control | Neutropenia (transient); does not penetrate eschar; contraindicated in sulfa allergy + pregnancy |
| Mafenide acetate | Broad spectrum; penetrates eschar | Best for infected burns + electrical burns | Painful on application; carbonic anhydrase inhibitor → metabolic acidosis |
| Silver nitrate 0.5% | Broad spectrum | Useful for SSD-resistant organisms | Stains everything black; hyponatraemia, hypokalaemia, hypochloraemia (leaches electrolytes) |
| Bacitracin/Mupirocin | Gram+ | Face/small burns | Limited Gram- coverage |
| Honey/Vaseline gauze | Antimicrobial; moist healing | Face, superficial burns |
Dressings
- Small superficial burns → moist non-adherent dressings (e.g. Mepitel, Mepilex)
- Larger partial thickness → silver-containing foam dressings; change every 3-5 days
- For transfer → large wounds: dry dressings (limit heat loss); small wounds: clean moist dressings
ESCHAROTOMY AND FASCIOTOMY
Escharotomy
- Indicated for circumferential full-thickness burns of limb or chest
- Circumferential burns create a rigid, non-compliant eschar → tourniquet effect → compartment syndrome
- Chest escharotomy: bilateral mid-axillary line incisions ± transverse incision = improves chest wall excursion + ventilation
- Increasing pain / paresthesia / pallor / pulselessness
- Compartment pressure >30 mmHg (or within 30 mmHg of diastolic BP)
- Doppler signals absent in digits
- Incision through eschar to fat (NOT fascia) in medial and lateral mid-axial lines of limb
- Extend across involved joints
- Digit escharotomies in lateral mid-axial lines
Fasciotomy
- For high-voltage electrical burns and crush injuries → myonecrosis + compartment syndrome despite escharotomy
- Can be performed through the bed of the escharotomy incision
SURGICAL MANAGEMENT OF BURN WOUNDS
Goals of Surgery (three interdependent goals):
- Closure - wound closure (life-saving for large burns)
- Function - preserve/restore range of movement
- Cosmesis - acceptable appearance
Timing of Excision
- Early excision and grafting = proven to improve survival in large burns and improve cosmesis in smaller burns
- Wounds that will take >21 days to heal → benefit from excision and grafting
- Wounds estimated to heal within 17 days → observe in most patients
- Burns >40% TBSA → rapid closure is life-saving (best defence against sepsis + catabolism)
Tangential Excision (most common method)
- Sequential shaving of burned tissue until viable bleeding dermis/fat is reached
- Signs of viability at surgery:
- Healthy dermis: pearly white appearance after exsanguination under tourniquet
- Healthy fat: bright yellow
- Nonviable dermis: red-to-purple staining after exsanguination
- Compromised fat: dull yellow-to-orange/brown
- Extremity burns excised under tourniquet (minimises blood loss)
Fascial Excision
- Burns of great depth over large area → excise to fascial level
- Greater blood loss reduction + efficiency, but marked functional and cosmetic impact
Wound Coverage Options
| Method | Description | Indication |
|---|---|---|
| Split-thickness skin graft (STSG) | Epidermis + partial dermis harvested (0.008-0.014 inch) from donor site | Large burn wounds; most common |
| Full-thickness skin graft (FTSG) | Entire dermis harvested | Small areas; face; hands - better cosmesis |
| Meshed STSG | STSG passed through mesher → expanded 1.5:1 to 6:1 ratio | Large TBSA burns (limited donor sites) |
| Sheet STSG | Unmeshed graft | Face, hands - cosmetically important areas |
| Biological dressings | Allografts (cadaveric skin), xenografts (pig skin), amnion | Temporary coverage while preparing definitive wound |
| Dermal substitutes | Integra (collagen-GAG matrix) | Deep burns with exposed tendons/bone; staged reconstruction |
| Flaps | Local/regional/free flaps | Exposed bone/tendon; special areas |
SYSTEMIC COMPLICATIONS OF MAJOR BURNS
Early (<48 hours) - Burn Shock Phase
| Complication | Mechanism | Management |
|---|---|---|
| Hypovolaemic shock | Massive capillary leak → plasma loss | Parkland resuscitation |
| Hyperkalaemia | Cell lysis + metabolic acidosis | Monitor ECG; treat if severe |
| Hypothermia | Loss of skin thermoregulation | Warming blankets, warm IV fluids |
| CO/Cyanide poisoning | Inhalation injury | 100% O2, hydroxocobalamin |
| Myoglobinuria | Electrical burns → rhabdomyolysis | Forced diuresis; alkalinise urine; consider mannitol |
Late (>48 hours) - Hyperdynamic/Septic Phase
| Complication | Details |
|---|---|
| Sepsis / invasive burn wound infection | Most common cause of death after inhalation injury; organisms: Pseudomonas, Staph aureus, Candida |
| ARDS | ~50% of intubated burn patients; lung-protective ventilation (TV <7 mL/kg, plateau pressure <31 cmH2O) |
| Ileus | Universal in major burns; early enteral nutrition preferred (NG tube) |
| Curling's ulcer | Stress ulceration; prophylaxis: enteral feeds + PPI/H2 blocker |
| Renal failure | From hypovolaemia or myoglobinuria |
| Hypermetabolic state | Tachycardia, fever, hyperdynamic circulation; driven by neurohormonal changes; persists until wound closed; managed with nutrition support |
| Heterotopic ossification | Calcium deposition at joints (especially elbow) in large burns |
| Hypertrophic scarring + contracture | Occurs when wounds take >21 days to heal |
ELECTRICAL BURNS
- High-voltage (>1000V): entry wound + exit wound; internal damage far exceeds external appearance
- Current follows path of least resistance: nerves, blood vessels, muscle
- Complications:
- Cardiac arrhythmias (ECG monitoring mandatory for 24 hours in high-voltage)
- Rhabdomyolysis → myoglobinuria → acute renal failure
- Compartment syndrome (may require fasciotomy even without visible burn)
- Cataracts (if current passes through head)
- Neurological injury, spinal cord injury
- Management: aggressive fluid resuscitation to maintain UO 1-1.5 mL/kg/hr to flush myoglobin; consider mannitol
CHEMICAL BURNS
| Alkalis (e.g. NaOH, Ca(OH)2) | Acids (e.g. HF, H2SO4) |
|---|---|
| Liquefactive necrosis - continues penetrating | Coagulative necrosis - self-limiting eschar |
| No fixed endpoint to damage | Damage limited by eschar |
| Often DEEPER than initially appears | |
| Management: copious water irrigation (30+ minutes) | Copious water irrigation |
| DO NOT neutralise (exothermic reaction worsens injury) | |
| Hydrofluoric acid (HF) special case: binds calcium/magnesium → hypocalcaemia + cardiac arrest → treat with topical calcium gluconate gel; IV calcium gluconate for systemic toxicity |
PROGNOSTIC SCORING
Baux Score
Baux Score = Age + %TBSA burned
- Scores >100-120 historically associated with ~50% mortality
- Revised Baux Score = Age + %TBSA + 17 (if inhalation injury present)
- Simple bedside predictor of mortality
Rule for Lethal Burns (50% mortality - LD50)
- Varies with age and burn centre
- Modern burn centres: LD50 ≈ 60-70% TBSA in healthy adults
NON-ACCIDENTAL INJURY (NAI) IN BURNS - RED FLAGS
- Stocking/glove distribution of scald injury (immersion burns - bilateral, sharply demarcated)
- Halo of spared buttocks skin (child held down during forced immersion)
- Delay in seeking medical attention
- History inconsistent with burn pattern or developmental stage
- Previous history of burn injury
- Unburned adults present at time of injury
- Bilateral/symmetric burns
NUTRITION IN BURNS
- Burns induce the highest metabolic rate of any injury (hypermetabolism)
- Early enteral nutrition (within 6 hours of burn) is preferred:
- Maintains gut mucosal integrity
- Reduces bacterial translocation
- Reduces catabolism
- Formulas used: Curreri formula for caloric requirements
- Adults: 25 kcal/kg/day + 40 kcal × %TBSA/day
- High protein requirement: 2-3 g/kg/day
- Glutamine supplementation has shown benefit in major burns
- Parenteral nutrition only if enteral route is unavailable
QUICK SUMMARY TABLE
| Key Fact | Answer |
|---|---|
| Burn depth formula | Depth = Temp × Duration / Blood flow |
| Superficial burn - included in TBSA? | NO |
| Partial + full thickness - included in TBSA? | YES |
| Rule of Nines - adult head | 9% |
| Rule of Nines - child head | 18% |
| Parkland formula | 4 mL × kg × %TBSA burned (Hartmann's/LR) |
| Parkland timing | ½ in first 8h (from time of burn), ½ in next 16h |
| UO target (adult) | 0.5 mL/kg/hr |
| UO target (child <30 kg) | 1 mL/kg/hr |
| CO poisoning - SpO2 | Falsely NORMAL - always check ABG |
| CO poisoning treatment | 100% oxygen (hyperbaric if severe) |
| Cyanide treatment | Hydroxocobalamin IV |
| Inhalation injury signs | Singed nasal hair, carbonaceous sputum, hoarseness, facial burns |
| Escharotomy indication | Circumferential full-thickness burn → compartment syndrome |
| Electrical burns: special concern | Rhabdomyolysis → renal failure; arrhythmia; damage > visible |
| HF acid: systemic toxicity | Hypocalcaemia → cardiac arrest; treat with calcium gluconate |
| Main cause of death after resuscitation | Inhalation injury / sepsis |
| Baux score | Age + %TBSA (+ 17 if inhalation injury) |
| Wound healing >21 days = | Surgical excision + grafting required |
| Best skin graft for face/hands | Sheet STSG or FTSG (cosmetically important) |
| Tangential excision viable dermis | Pearly white appearance (under tourniquet) |
| Curling's ulcer | Stress ulcer in burns (prophylaxis: enteral feeds + PPI) |
| Topical agent best for penetrating eschar | Mafenide acetate |
| Silver nitrate side effect | Hyponatraemia, hypokalaemia (electrolyte leaching) |
| Non-accidental burn pattern | Stocking/glove distribution, halo sparing |
Plastic surgery
PLASTIC SURGERY 101 - COMPREHENSIVE GUIDE
DEFINITION AND SCOPE
- Congenital anomalies
- Trauma
- Infection
- Oncological resection
- Burns
- Ageing
- Reconstructive surgery - restoring normal form and function
- Aesthetic (cosmetic) surgery - improving appearance in a normally functioning individual
WOUND HEALING - FOUNDATIONAL KNOWLEDGE
Types of Wound Healing
| Type | Description | Example |
|---|---|---|
| Primary intention | Wound edges reapproximated soon after injury - sutures, staples, glue, tape | Clean surgical incision |
| Secondary intention | Wound left open; heals by granulation tissue + wound contraction + re-epithelialisation | Infected wound, abscess cavity |
| Tertiary intention (delayed primary closure) | Wound left open initially, then closed after 3-5 days once infection/contamination controlled | Contaminated traumatic wound |
Phases of Wound Healing (4 phases, overlapping continuum)
INJURY
│
▼
1. HAEMOSTASIS (immediate - minutes)
Platelet activation → platelet plug → clotting cascade
Platelets release: PDGF, TGF-β, VEGF, PF4, CD40L
Vasoconstriction (catecholamines, thromboxane A2)
│
▼
2. INFLAMMATION (hours to days 1-4)
Vasodilation + capillary permeability ↑ (histamine, VEGF)
PMNs arrive first (hours) → clear bacteria + debris
Macrophages arrive (day 2-3) → 'DIRECTOR of repair'
- Phagocytosis + secrete cytokines: TNF-α, IL-1, IL-6, TGF-β, EGF, FGF, PDGF
- Orchestrate transition to proliferative phase
│
▼
3. PROLIFERATION (days 4 to ~3 weeks)
Fibroblast migration + collagen synthesis (Type III first → then Type I)
Angiogenesis (VEGF) → granulation tissue
Re-epithelialisation - keratinocytes migrate from wound edges
Wound contraction - myofibroblasts (contain α-smooth muscle actin)
│
▼
4. REMODELLING / MATURATION (weeks to 1+ year)
Type III collagen replaced by Type I collagen
Cross-linking of collagen → tensile strength ↑
Maximum tensile strength = 80% of original (never reaches 100%)
Vascularity ↓ (scar becomes pale and less raised)
Key Growth Factors in Wound Healing
| Growth Factor | Source | Role |
|---|---|---|
| PDGF (Platelet-derived) | Platelets, macrophages | Fibroblast + SMC proliferation; chemotaxis |
| TGF-β | Platelets, macrophages | Collagen synthesis; fibrosis; scar formation |
| VEGF | Macrophages, keratinocytes | Angiogenesis |
| EGF | Platelets, macrophages | Epithelial + fibroblast proliferation |
| FGF | Fibroblasts, macrophages | Angiogenesis; fibroblast proliferation |
Factors Impairing Wound Healing
| Local Factors | Systemic Factors |
|---|---|
| Infection | Diabetes mellitus (↓ WBC function, ↓ collagen synthesis, neuropathy, ischaemia) |
| Poor blood supply / ischaemia | Malnutrition (especially Vitamin C and Zinc deficiency) |
| Foreign body | Anaemia |
| Irradiated tissue | Steroids / immunosuppressants |
| Haematoma | Renal/hepatic failure |
| Excessive tension on wound | Chemotherapy |
| Denervation | Smoking |
THE RECONSTRUCTIVE LADDER (and Reconstructive Elevator)
MOST COMPLEX
║
╠══ Free tissue transfer (free flap + microsurgical anastomosis)
║
╠══ Pedicled distant flap (e.g. groin flap, pectoralis major flap)
║
╠══ Pedicled local flap (advancement, transposition, rotation)
║
╠══ Tissue expansion
║
╠══ Full-thickness skin graft (FTSG)
║
╠══ Split-thickness skin graft (STSG)
║
╠══ Secondary intention healing (granulation + contraction)
║
╚══ Primary closure (direct suture)
SIMPLEST
SKIN ANATOMY (relevant to grafts and flaps)
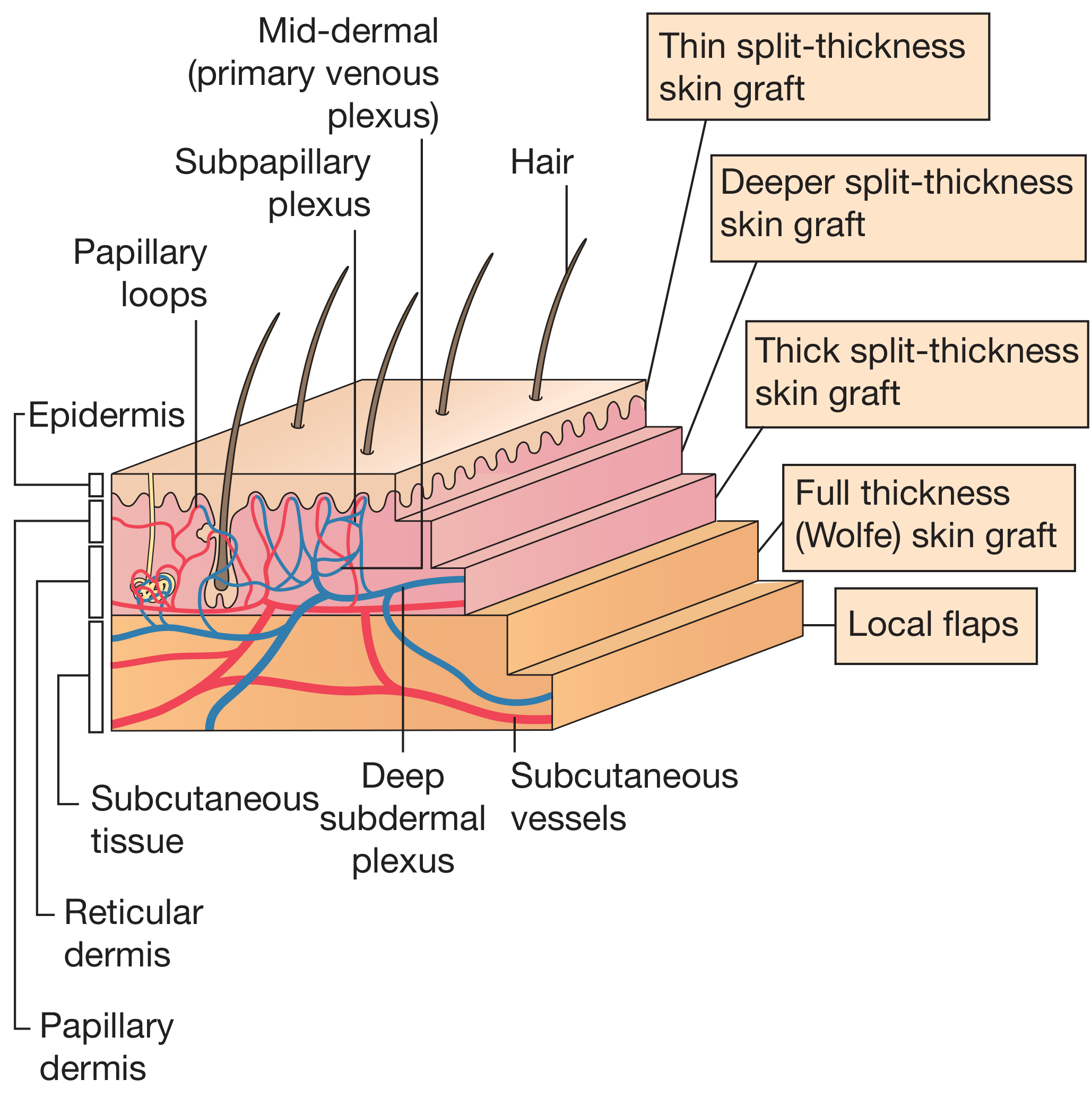
GRAFTS
Stages of Graft Take
1. PLASMATIC IMBIBITION (0-48h)
Serum diffuses from wound bed into graft → graft survives by diffusion
Graft appears pale/oedematous
↓
2. INOSCULATION (24-48h)
New capillaries from recipient bed "kiss" (inosculate) existing graft vessels
Random anastomoses form
↓
3. REVASCULARISATION (48-72h)
True vascular ingrowth from bed into graft
Graft becomes pink - indicates successful take
Causes of Graft Failure (remember: SHI)
- Shear forces - lifts graft off bed (most common)
- Haematoma/seroma - fluid between graft and bed prevents contact
- Infection (especially Group A β-haemolytic Streptococcus - lyses fibrin that anchors graft)
- Bone without periosteum
- Tendon without paratenon
- Cartilage (avascular)
- Irradiated tissue
- Infected wound
Split-Thickness Skin Graft (STSG) vs Full-Thickness Skin Graft (FTSG)
| Feature | STSG | FTSG (Wolfe Graft) |
|---|---|---|
| Layers harvested | Epidermis + part of dermis | Epidermis + entire dermis |
| Thickness | 0.008-0.014 inch (0.2-0.4 mm) | Variable by site |
| Tool | Dermatome (Watson, Humby) | Scalpel |
| Donor site healing | Re-epithelialises from adnexa (hair follicles, sweat glands) - 10-14 days | Must be closed primarily (limits size) |
| Contraction | Significant (more) | Minimal (less) |
| Cosmesis | Poorer - thinner, often hyperpigmented | Better - colour/texture match |
| Take rate | Higher (thinner = easier diffusion) | Lower (thicker dermis = harder plasmatic imbibition) |
| Can be meshed? | YES - expand 1.5:1 to 6:1 for large areas | NO |
| Indications | Large burn wounds; donor-site limited reconstruction | Face, hands, eyelids, cosmetically important areas |
| Common donor sites | Lateral thigh, buttock, medial upper arm | Groin, retroauricular (behind ear), supraclavicular, inner upper arm |
- Passed through a mesher → expanded lattice pattern
- Advantages: covers larger areas; allows fluid drainage from beneath graft
- Disadvantage: "crocodile skin" appearance - poor cosmesis
- No meshing → better cosmesis
- Reserved for face, hands, cosmetically important areas
Other Graft Types
| Graft Type | Origin | Clinical Use |
|---|---|---|
| Autograft | Same individual | Gold standard |
| Allograft | Same species, different individual (cadaveric) | Temporary coverage - extensive burns, necrotising fasciitis |
| Xenograft | Different species (porcine/pig skin) | Temporary wound coverage |
| Composite graft | Skin + cartilage (e.g. from ear) | Nasal alar reconstruction |
| Cartilage graft | Conchal bowl ear, nasal septum, costal cartilage | Nasal/auricular reconstruction |
| Bone graft | Iliac crest, calvarium, fibula | Bony reconstruction |
| Nerve graft | Sural nerve, medial cutaneous nerve of forearm | Bridging nerve gaps |
| Tendon graft | Palmaris longus, plantaris | Tendon reconstruction |
| Fat graft (lipotransfer) | Abdomen, thigh, buttock | Volume augmentation; scar remodelling |
Skin Substitutes
- Integra (bovine collagen-GAG matrix + silastic membrane): used for deep burns; staged (first apply Integra, later apply thin STSG)
- AlloDerm (decellularised human dermis): provides dermal layer in staged reconstruction
- Epicel (autologous cultured keratinocytes): for extensive burns with limited donor sites
FLAPS
Classification of Flaps
1. By Tissue Composition
| Type | Contents | Examples |
|---|---|---|
| Cutaneous | Skin + subcutaneous fat | Rotation flap |
| Fasciocutaneous | Skin + fascia | Radial forearm flap, ALT flap |
| Musculocutaneous | Skin + muscle | TRAM flap, latissimus dorsi flap |
| Muscle only | Muscle ± skin grafted on top | Pectoralis major, gastrocnemius |
| Osseous | Bone ± soft tissue | Fibula free flap (mandible), iliac crest |
| Osteomyocutaneous | Bone + muscle + skin | Free fibula with skin paddle |
| Chimeric | Multiple independent flaps on common source vessel | ALT + vastus lateralis chimeric flap |
2. By Blood Supply Pattern
| Type | Blood Supply | Features | Examples |
|---|---|---|---|
| Random pattern | Dermal/subdermal plexus - no specific named vessel | Length:width ratio ≤1.5:1 (otherwise tip necrosis risk) | Advancement, rotation, transposition local flaps |
| Axial pattern | Named cutaneous artery runs along axis of flap | Higher length:width ratio possible | Groin flap (superficial circumflex iliac artery), forehead flap (supratrochlear artery), deltopectoral flap |
| Perforator | Single perforating vessel from deep source | Spares underlying muscle | ALT perforator flap (anterolateral thigh) |
3. By Movement Type (Local Flaps)
| Movement | How It Works | Use |
|---|---|---|
| Advancement flap | Flap slides forward in one direction | Scalp, forehead, digit |
| Rotation flap | Semicircular flap rotates about a pivot point | Scalp, buttock (pressure sore) |
| Transposition flap | Flap rotates and jumps over normal skin | Z-plasty, rhomboid (Limberg) flap |
| Interpolation flap | Pedicle crosses over normal skin; divided at 3 weeks | Forehead flap to nose (staged) |
| Bipedicle flap | Supplied from both ends ("bucket handle") | Lower eyelid reconstruction |
4. By Location Relative to Defect
| Type | Description |
|---|---|
| Local flap | Adjacent to the defect |
| Regional/pedicled distant flap | Nearby but not adjacent; pedicle left intact |
| Free flap | Completely detached and reattached via microsurgical anastomosis |
Muscle Flap Classification (Mathes and Nahai)
| Type | Pedicle | Examples |
|---|---|---|
| I | Single vascular pedicle | Tensor fascia lata (TFL), Gastrocnemius |
| II | One dominant + one or more minor pedicles | Gracilis, Biceps femoris, Sternocleidomastoid, Soleus, Trapezius |
| III | Two dominant pedicles | Gluteus maximus, Rectus abdominis, Pectoralis minor, Serratus anterior |
| IV | Segmental pedicles | Sartorius, Tibialis anterior, Flexor hallucis longus |
| V | One dominant + segmental minor pedicles | Latissimus dorsi, Pectoralis major (can survive on minor pedicles) |
Fasciocutaneous Flap Classification (Cormack and Lamberty)
| Type | Blood Supply | Examples |
|---|---|---|
| A | Multiple perforators along base | Pontén flap |
| B | Single perforator along axis | Scapular flap, Parascapular flap |
| C | Segmental perforators from same source vessel | Radial forearm flap, Lateral arm flap |
| D | Type C + bone component | Free fibula flap (osteomyofasciocutaneous) |
Common Named Flaps and Their Uses
| Flap | Blood Supply | Tissue | Common Use |
|---|---|---|---|
| Latissimus dorsi (LD) | Thoracodorsal artery (Type V) | Muscle ± skin paddle | Breast reconstruction, back wounds, scalp |
| TRAM (Transverse Rectus Abdominis Myocutaneous) | Superior epigastric artery (pedicled) or inferior epigastric (free) | Muscle + skin | Breast reconstruction |
| DIEP (Deep Inferior Epigastric Perforator) | Deep inferior epigastric perforators | Fat + skin (no muscle) | Breast reconstruction (spares muscle) |
| Pectoralis major | Thoracoacromial artery (Type V) | Muscle ± skin | Head and neck reconstruction, sternal wound |
| Radial forearm free flap | Radial artery | Fasciocutaneous | Oral/pharyngeal reconstruction, hand |
| ALT (Anterolateral thigh) free flap | Descending branch lateral circumflex femoral artery | Fasciocutaneous/perforator | Large defects - head and neck, perineum |
| Free fibula | Peroneal artery | Osteomyocutaneous | Mandibular reconstruction |
| Gastrocnemius | Sural arteries (Type I) | Muscle | Knee, upper tibia coverage |
| Soleus | Posterior tibial artery (Type II) | Muscle | Middle third tibia |
| Gracilis | Medial circumflex femoral artery (Type II) | Muscle | Perineal reconstruction, facial reanimation |
| Gluteus maximus | Superior/inferior gluteal arteries (Type III) | Muscle ± skin | Pressure sore (ischial, sacral) |
| Forehead flap | Supratrochlear artery (axial) | Skin | Nasal reconstruction |
| Groin flap | Superficial circumflex iliac artery (axial) | Skin | Hand reconstruction, pedicled coverage |
| Deltopectoral flap | Internal mammary perforators (axial) | Skin | Head and neck reconstruction |
Free Flap Microsurgery
- Recipient artery and vein at/near defect
- Microsurgical expertise (operating microscope, 8-0 to 10-0 sutures)
- Anastomosis types: end-to-end or end-to-side
- Clinical: colour (pink = good; pale = arterial failure; blue/congested = venous failure), capillary refill, turgor
- Temperature monitoring
- Doppler (hand-held or implantable)
- Hourly observations for first 72 hours
- Arterial thrombosis → pale, cold, non-bleeding flap → return to theatre urgently
- Venous congestion → blue, congested, brisk dark bleeding on pin-prick → return to theatre
- Window of salvage: typically 6 hours from onset of ischaemia
LOCAL TISSUE REARRANGEMENT
Z-Plasty
- Lengthen a scar or contracture (primary use)
- Reorient a scar along LORST
- Break up a straight scar (prevents recurrence of contracture)
Design:
- Central limb = scar/contracture
- Two diagonal arms at 60° angles (standard Z-plasty)
- Transpose the two triangular flaps
Effect of 60° Z-plasty = 75% lengthening of central limb
| Angle | % Lengthening |
|---|---|
| 30° | 25% |
| 45° | 50% |
| 60° | 75% (standard; most commonly used) |
| 75° | 100% |
| 90° | 120% |
W-Plasty
- Multiple small triangular cuts along scar edges
- Breaks up a straight scar into a zigzag pattern
- Does NOT lengthen the scar (unlike Z-plasty)
- Used to reorient a scar crossing LORST
Rhomboid (Limberg) Flap
- 60° rhomboid design
- Single transposition flap for small defects
- Commonly used for: cheek, forehead, scalp defects
WOUND CLOSURE TECHNIQUES (in order of complexity)
| Method | Indication | Notes |
|---|---|---|
| Tape/steri-strips | Small superficial wounds, additional support after suture removal | No tensile strength |
| Tissue glue (cyanoacrylate) | Small, superficial, low-tension wounds | Children; face |
| Staples | Scalp, trunk, limbs - rapid closure | Not suitable for face |
| Interrupted sutures | Most wounds; allows individual suture removal if infection | |
| Continuous suture | Long wounds; haemostasis | |
| Subcuticular (intradermal) | Cosmetic closure; no suture marks | Remove at 5-7 days (face) or 10-14 days (trunk/limb) |
| Mattress sutures | Tension/eversion | Vertical mattress = everting; horizontal mattress = tension closure |
| Retention sutures | High-tension, obese, re-do laparotomy | Through all layers |
| Negative pressure wound therapy (NPWT/VAC) | Complex wounds; wound bed preparation pre-grafting; open abdomen | 125 mmHg sub-atmospheric pressure promotes granulation |
ABNORMAL SCARRING
Hypertrophic Scar vs Keloid
| Feature | Hypertrophic Scar | Keloid |
|---|---|---|
| Extent | Within original wound boundaries | EXTENDS beyond original wound boundaries |
| Timing | Within weeks of injury | Months after injury |
| Spontaneous regression | May occur over 1-2 years | Does NOT regress |
| Site predilection | Flexor surfaces, burns | Earlobes, deltoid, presternal, face |
| Skin type | Any | More common in darker skin types (Fitzpatrick III-VI) |
| Symptoms | Itching, tenderness | Itching, pain - can be debilitating |
| Recurrence after excision | Lower | High recurrence - treat with adjuvants |
Treatment of Keloid/Hypertrophic Scars
| Treatment | Notes |
|---|---|
| Topical silicone sheets/gel | First-line; applied for 12+ hours/day for months; mechanism unclear (possibly pressure + hydration) |
| Intralesional corticosteroid (triamcinolone) | Reduces collagen synthesis; repeated every 4-6 weeks |
| Pressure therapy | Compression garments; used especially post-burn; maintained for 12-24 months |
| Surgical excision | Risk of recurrence (up to 80% for keloids) - must be combined with adjuvant |
| Radiotherapy (post-excision) | Given within 24-48h of excision; reduces recurrence to ~15% for keloids |
| Laser therapy | CO2 or pulsed dye laser; improves colour, texture, symptoms |
| Intralesional 5-fluorouracil | Anti-proliferative; adjunct |
| Cryotherapy | Freezing; useful for small keloids |
PRESSURE ULCERS (Pressure Sores / Decubitus Ulcers)
Pathophysiology
- Prolonged pressure → capillary occlusion → ischaemia → tissue necrosis
- Pressure >32 mmHg (capillary closing pressure) for >2 hours → tissue breakdown
- Shear forces, moisture (incontinence), friction all contribute
- Most commonly over bony prominences: sacrum, ischium, greater trochanter, heel, lateral malleolus
Staging (NPUAP Classification)
| Stage | Description |
|---|---|
| Stage 1 | Non-blanchable erythema on intact skin |
| Stage 2 | Partial-thickness skin loss; shallow open ulcer or blister; into epidermis/superficial dermis |
| Stage 3 | Full-thickness skin loss down to subcutaneous fat; no bone/tendon/muscle visible |
| Stage 4 | Full-thickness loss with exposed bone, tendon, or muscle |
| Unstageable | Full-thickness ulcer obscured by slough/eschar |
| Deep tissue injury (DTI) | Purple/maroon intact skin or blood-filled blister |
Prevention
- Regular repositioning (every 2 hours)
- Pressure-relieving mattresses/cushions (alternating pressure, foam)
- Skin care (moisture barrier creams, incontinence management)
- Nutritional optimisation
- Early mobilisation
Management
- Relieve pressure (absolutely)
- Wound debridement (enzymatic/autolytic/surgical)
- Appropriate wound dressings (moist healing environment)
- Nutritional support (protein + Vitamin C + Zinc)
- Debridement of all necrotic tissue first
- Local muscle or myocutaneous flap reconstruction (NOT just a skin graft - scar would be at point of maximum pressure; muscle obliterates dead space)
- Common flaps by site:
| Site | Preferred Flap |
|---|---|
| Sacral | Gluteus maximus rotation/advancement flap |
| Ischial | Gluteus maximus, Biceps femoris, Gracilis flap |
| Trochanteric | Tensor fascia lata (TFL) flap |
| Heel | Sural flap |
TISSUE EXPANSION
- Silicone balloon expander inserted under skin adjacent to defect
- Gradually inflated over weeks/months with saline → skin stretches (biological creep + mechanical creep)
- Creates extra skin of IDENTICAL colour, texture, thickness, sensibility
- Used for: scalp reconstruction, breast reconstruction, scar revision
- Complication: infection, extrusion, rupture, implant exposure
NEGATIVE PRESSURE WOUND THERAPY (NPWT/VAC)
- Foam dressing sealed with airtight membrane → connected to suction device
- Applied at -125 mmHg continuous or intermittent
- Mechanism:
- Removes interstitial oedema
- Increases local blood flow
- Promotes granulation tissue
- Reduces bacterial load
- Draws wound edges together
- Indications: complex wounds, open abdomen, wound bed preparation before grafting, sternal wounds, diabetic foot ulcers, split-thickness graft fixation
LIPOTRANSFER (Autologous Fat Grafting)
- Harvest - liposuction from abdomen/thigh/buttock using cannula under local anaesthetic
- Preparation - centrifugation of fat aspirate (removes oil, blood, debris)
- Injection - at recipient site with specialised cannula (microdroplets)
- Breast reconstruction volume augmentation
- Facial rejuvenation
- Scar remodelling (especially post-radiotherapy - adipose-derived stromal cells modulate healing)
- Progressive hemifacial atrophy (Parry-Romberg syndrome)
- Buttock augmentation (Brazilian Butt Lift)
ALLOPLASTIC IMPLANTS
| Implant | Material | Use |
|---|---|---|
| Breast implants | Outer silicone shell + saline or silicone gel filling | Augmentation + reconstruction |
| Cranioplasty plates | Titanium or PEEK | Replace cranial bone defects |
| Medpor (porous polyethylene) | Porous polyethylene | Facial skeletal augmentation (cheek, chin, orbital floor) |
| Bone substitutes | Hydroxyapatite, calcium phosphate | Small bony defects |
- Capsular contracture (scar tissue contracts around implant → hard, distorted breast)
- Rupture (silicone: silent; saline: deflates)
- Implant-associated ALCL (anaplastic large-cell lymphoma) - rare, linked to textured implants
- Interference with mammographic cancer surveillance
SPECIFIC CONGENITAL CONDITIONS
Cleft Lip and Palate
| Type | Incidence | Associated |
|---|---|---|
| Cleft lip alone | 1 in 1000 | 20% of clefts |
| Cleft lip + palate | 1 in 700 | 45% of clefts |
| Cleft palate alone | 1 in 2000 | 35% of clefts |
- More common in males (cleft lip ± palate); females (cleft palate alone)
- Unilateral (more common) or bilateral
- Associated with: Pierre-Robin sequence (cleft palate + micrognathia + glossoptosis)
- Cleft lip: failure of fusion of medial nasal process + maxillary process
- Cleft palate: failure of fusion of palatal shelves
| Repair | Timing | Rationale |
|---|---|---|
| Cleft lip | 3 months (10 weeks, 10 lbs/4.5 kg, Hb >10) | Before social milestone |
| Cleft palate | 6-18 months (before speech development) | Allows speech; if delayed, velopharyngeal insufficiency |
- Cleft lip: Millard rotation-advancement repair (most common); Tennison-Randall (geometric)
- Cleft palate: Von Langenbeck, Furlow double-opposing Z-plasty (lengthens palate)
QUICK EXAM SUMMARY TABLE
| Fact | Answer |
|---|---|
| Plastic surgery derives from | Greek "plassein" = to mould/shape |
| 4 phases of wound healing | Haemostasis → Inflammation → Proliferation → Remodelling |
| First cell in inflammation phase | PMNs (neutrophils) |
| "Director of repair" cell | Macrophage |
| Collagen type in early wound | Type III (later replaced by Type I) |
| Maximum tensile strength of scar | 80% of original |
| Reconstructive elevator | Modern concept - optimal technique for each patient, not just simplest |
| STSG donor site heals by | Re-epithelialisation from adnexal remnants (10-14 days) |
| FTSG donor site | Must be closed primarily |
| Graft take - three stages | Plasmatic imbibition → Inosculation → Revascularisation |
| Most common cause of graft failure | Shear forces (also: haematoma, Group A Strep) |
| Graft will not take on | Avascular bone, tendon without paratenon, cartilage, irradiated tissue |
| Z-plasty 60° = | 75% lengthening |
| W-plasty purpose | Reorient scar, break straight line; does NOT lengthen |
| Keloid vs hypertrophic | Keloid extends BEYOND wound; hypertrophic stays within |
| Keloid common sites | Earlobes, deltoid, presternal region, face |
| Keloid treatment | Silicone + steroid injection + excision + post-op radiotherapy |
| Mathes-Nahai Type V muscle | Latissimus dorsi, Pectoralis major (dominant + segmental pedicles) |
| Type I muscle (single pedicle) | Tensor fascia lata, Gastrocnemius |
| Random flap L:W ratio | ≤1.5:1 (otherwise tip necrosis) |
| Sacral pressure sore flap | Gluteus maximus rotation flap |
| Ischial pressure sore flap | Gluteus maximus or Biceps femoris flap |
| NPWT pressure | -125 mmHg |
| Cleft lip repair timing | 3 months (Rule of Tens: 10 weeks, 10 lbs, Hb 10) |
| Cleft palate repair timing | 6-18 months (before speech) |
| Fat graft disadvantage | 20-80% resorption; fat embolism risk |
| Integra layers | Bovine collagen-GAG matrix + silastic membrane (temporary) |
| Free flap arterial failure appearance | Pale, cold, non-bleeding flap → return to theatre within 6 hours |
| Free flap venous failure appearance | Blue, congested, dark blood on pin-prick |
Choledocolethiasis 101
Abdomen 101- preclinicals, clinically, diseases, investigations, management from cpg, nice
Intestinal Obstruction and perforation presentation
Presentation: Clinical Features of Intestinal Obstruction + Neonatal Causes - Hema Cardinal features: History: Pain, vomiting, distension, constipation Examination: Distension, bowel sounds, dehydration Acute intestinal obstruction in newborn: Intestinal atresia Meconium ileus Meckel’s diverticulum Foreign body
Presentation: Definition of intestinal obstruction ● Classification: ○ Dynamic (mechanical) ○ Adynamic (non-mechanical) ● Overview of importance and complications
Thyroid ca 101