Factors influencing glomerular filtration for 5 marks
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete 5-mark answer on the factors influencing glomerular filtration:
Factors Influencing Glomerular Filtration
The Starling Equation for GFR
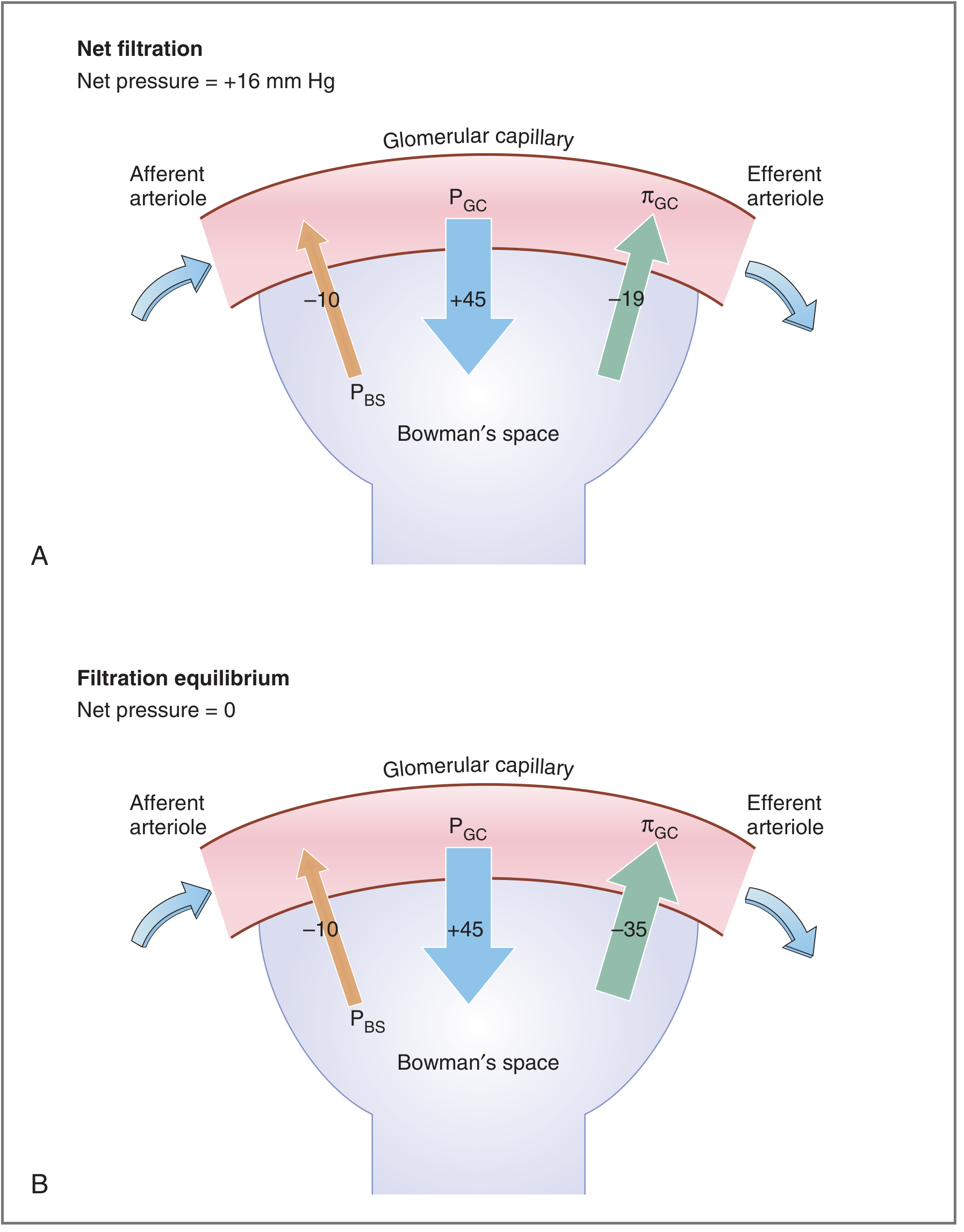
Glomerular filtration is governed by the Starling equation:
GFR = K_f [(P_GC - P_BS) - π_GC]
Where:
- K_f = filtration coefficient
- P_GC = hydrostatic pressure in glomerular capillary
- P_BS = hydrostatic pressure in Bowman's space
- π_GC = oncotic pressure in glomerular capillary
The net ultrafiltration pressure is the algebraic sum of these three Starling pressures, and GFR = K_f x net ultrafiltration pressure.
1. Filtration Coefficient (K_f)
K_f reflects the hydraulic permeability x total surface area of the glomerular capillary barrier. It is over 100-fold higher in glomerular capillaries than in systemic capillaries, which is why GFR (~180 L/day) far exceeds filtration in all other capillaries combined.
- Factors reducing K_f: Contraction of mesangial cells (in response to angiotensin II, vasopressin, endothelin) reduces the available filtration surface area and decreases GFR.
- Factors increasing K_f: Relaxation of mesangial cells increases surface area and raises GFR.
- Glomerular diseases (e.g., membranous nephropathy, glomerulosclerosis) reduce K_f structurally.
2. Glomerular Capillary Hydrostatic Pressure (P_GC) - FAVORS filtration
Normal P_GC is ~45 mm Hg. This is the primary driving force for filtration and is determined by:
a) Afferent arteriolar resistance:
- Afferent constriction (sympathetic activation, high angiotensin II) → reduces blood flow into the glomerulus → decreases P_GC → decreases GFR
- Afferent dilation (prostaglandins, nitric oxide) → increases P_GC → increases GFR
b) Efferent arteriolar resistance:
- Efferent constriction (low-level angiotensin II) → restricts outflow, blood "backs up" into glomerulus → increases P_GC → increases GFR
- Efferent dilation (ACE inhibitors, which block angiotensin II) → lowers P_GC → decreases GFR
c) Systemic arterial pressure: Over the autoregulatory range (80-180 mmHg), myogenic reflexes and tubuloglomerular feedback keep GFR stable. Outside this range, GFR follows perfusion pressure directly.
| Change | RPF | GFR | Filtration Fraction |
|---|---|---|---|
| Afferent constriction | ↓ | ↓ | No change |
| Efferent constriction | ↓ | ↑ | ↑ |
| Increased plasma protein | No change | ↓ | ↓ |
| Ureteral obstruction | No change | ↓ | ↓ |
3. Hydrostatic Pressure in Bowman's Space (P_BS) - OPPOSES filtration
Normal P_BS is ~10 mm Hg, generated by the fluid already present in the tubule.
- Ureteral/tubular obstruction (e.g., kidney stones, prostatic hypertrophy) increases P_BS → reduces net ultrafiltration pressure → decreases GFR
- Renal edema or increased interstitial pressure can also raise P_BS.
4. Oncotic Pressure in Glomerular Capillaries (π_GC) - OPPOSES filtration
Normal π_GC is ~19 mmHg at the afferent end, rising to ~35 mmHg at the efferent end (as protein-free filtrate is removed and protein is concentrated). When π_GC equals the net hydrostatic driving force, filtration equilibrium is reached and filtration stops.
- Increased plasma protein concentration → higher π_GC → opposes filtration → decreases GFR
- Decreased plasma protein (e.g., nephrotic syndrome, malnutrition, liver failure) → lower π_GC → increases net ultrafiltration pressure → increases GFR
- Reduced renal blood flow → protein concentrates faster along the capillary length → filtration equilibrium is reached sooner → decreases GFR
5. Renal Blood Flow (RBF)
RBF determines how much plasma is presented to the glomerulus per unit time.
- Normal RBF = ~1200 mL/min (25% of cardiac output)
- Increased RBF delays the rise in π_GC along the capillary, allowing filtration to continue over a greater capillary length → increases GFR
- Decreased RBF (e.g., hemorrhage, heart failure, renal artery stenosis) accelerates π_GC rise → filtration equilibrium reached earlier → decreases GFR
6. Properties of the Glomerular Filtration Barrier
The three-layered barrier (endothelium with 70-100 nm pores → basement membrane → podocyte epithelium with 25-60 nm filtration slits) influences what is filtered:
- Size selectivity: Molecules larger than ~8 nm are excluded. The basement membrane is the principal size barrier.
- Charge selectivity: Fixed negative charges (glycoproteins) on all layers repel anionic macromolecules (e.g., albumin is both large and negatively charged, hence excluded). Loss of these charges in glomerulonephritis → proteinuria.
Summary Table
| Factor | Normal Value | Effect if Increased | Effect if Decreased |
|---|---|---|---|
| K_f (filtration coefficient) | High | ↑ GFR | ↓ GFR |
| P_GC (glomerular hydrostatic pressure) | 45 mmHg | ↑ GFR | ↓ GFR |
| P_BS (Bowman's space pressure) | 10 mmHg | ↓ GFR | ↑ GFR |
| π_GC (capillary oncotic pressure) | 19-35 mmHg | ↓ GFR | ↑ GFR |
| Renal blood flow | ~1200 mL/min | ↑ GFR | ↓ GFR |
Sources: Costanzo Physiology 7th Ed., pp. 267-270; National Kidney Foundation Primer on Kidney Diseases 8e, p. 21; Tietz Textbook of Laboratory Medicine 7th Ed., p. 1857; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.