Echinococci infections in detail
Reading File
Finding Sources
Searching PubMed
echinococcosis hydatid disease
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Searching Images
echinococcal hydatid cyst liver CT ultrasound
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks plus excellent imaging. Let me compile the full detailed response.
Echinococcal Infections (Echinococcosis / Hydatid Disease)
Echinococcosis is a zoonotic parasitic disease caused by larval tapeworms of the genus Echinococcus (family Taeniidae). It is classified by the WHO as one of 20 neglected tropical diseases, with over 1 million individuals estimated to be infected worldwide. — Tietz Textbook of Laboratory Medicine, 7th Ed.
1. Species and Forms of Disease
| Species | Disease | Character |
|---|---|---|
| E. granulosus complex (G1–G10) | Cystic echinococcosis (CE) | Single, enclosed cyst; most common |
| E. multilocularis | Alveolar echinococcosis (AE) | Tumor-like infiltrative, multi-cystic |
| E. vogeli | Polycystic echinococcosis | Rare; S. & C. America |
| E. oligarthrus | Polycystic echinococcosis | Rare; S. & C. America |
2. Life Cycle
The adult E. granulosus tapeworm lives in the small bowel of dogs, wolves, and other canines, surviving approximately 12 months. The entire worm measures only ~5 mm with just three proglottids (one immature, one mature, one gravid). The gravid segment releases eggs that are morphologically identical to Taenia saginata/solium eggs.
Transmission to humans (accidental intermediate hosts):
- Ingestion of embryonated eggs from dog feces (fecal-oral route; contaminated vegetables, soil, water)
- Eggs hatch in the intestine → oncospheres penetrate the intestinal wall
- Oncospheres travel via portal blood → liver (first filter; majority lodge here)
- Those traversing the liver enter pulmonary circulation → lungs (second filter)
- A small number pass into systemic circulation → brain, heart, bones, kidneys, spleen
Cyst development:
- Survivors form a cyst with an outer laminated cuticle (acellular) and inner germinal membrane (cellular)
- Cyst fills with clear fluid and expands: ~1 cm over 5–6 months; can reach >10 cm over years
- Germinal layer gives rise to brood capsules → protoscolices (immature tapeworms)
- Daughter cysts form within the mother cyst; degenerated protoscolices/membranes settle as hydatid sand
Completing the cycle: When a dog eats infected viscera of intermediate hosts (sheep, cattle, etc.), protoscolices are released in the intestine and develop into adult worms.
For E. multilocularis: Definitive hosts are foxes and coyotes; intermediate hosts are rodents (voles, mice). Larval forms bud externally (unlike E. granulosus), forming infiltrative multilocular cysts. Humans are infected by ingesting eggs from fox feces (via contaminated berries, soil, or domestic dogs that have eaten infected rodents). — Sherris & Ryan's Medical Microbiology, 8th Ed.
3. Epidemiology
-
Cystic echinococcosis (E. granulosus): Global distribution — highly endemic in eastern/southern Europe, northern Africa, Central Asia, southern South America, and sheep-raising regions of Australia. Predominantly a pastoral-cycle disease; highest rates where dogs feed on raw animal viscera. Up to 6.6% infection prevalence detected in endemic areas by community ultrasound surveys. — Goldman-Cecil Medicine
-
Alveolar echinococcosis (E. multilocularis): Northern hemisphere — western China, Tibet, central Asia, alpine Europe, and subarctic North America. Has recently emerged in western Canada. Less common but more dangerous.
-
Both are rare in the US; most US cases occur in Alaska, the southwestern sheep-raising states, and among foreign-born individuals from endemic regions.
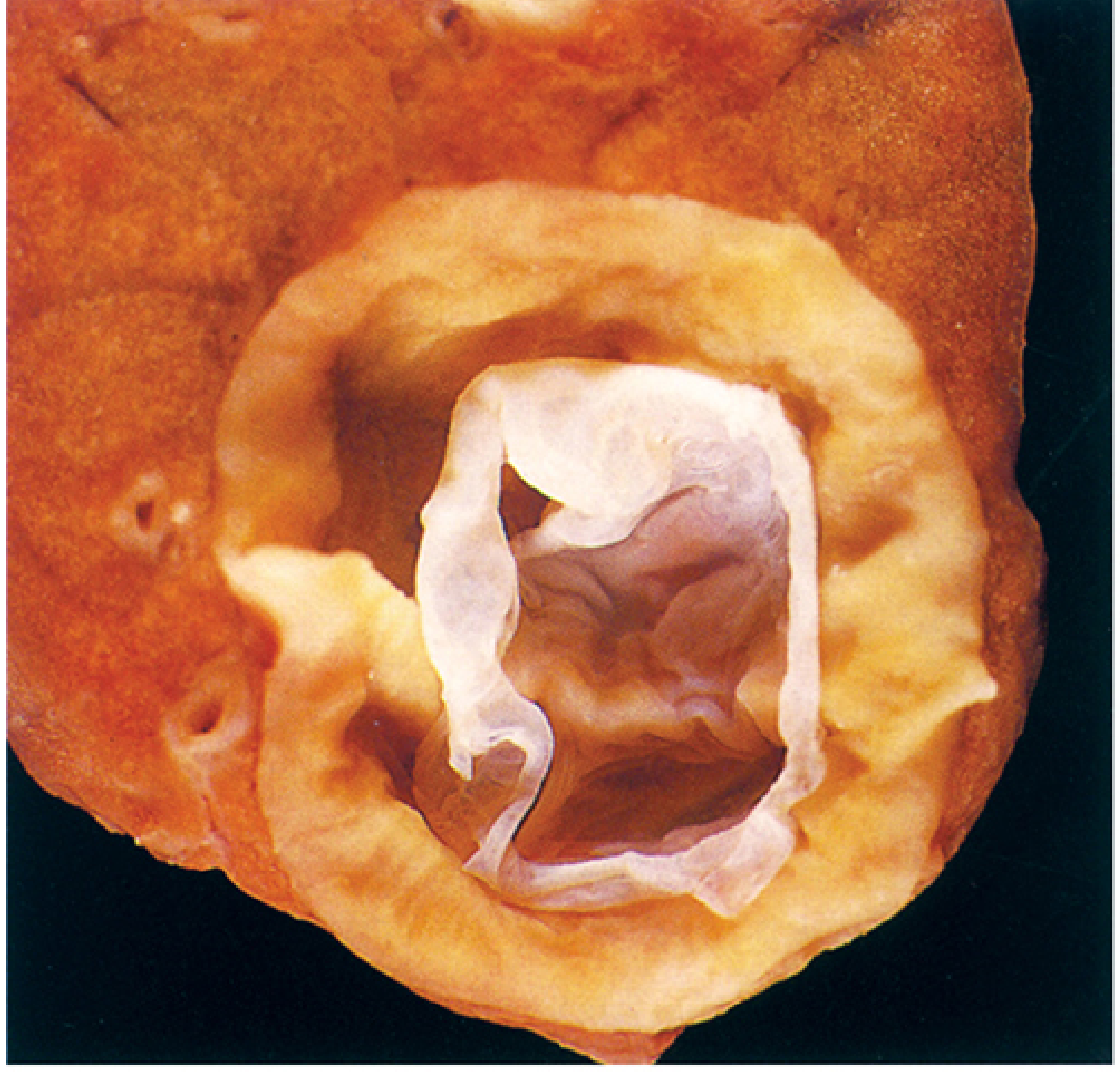
4. Pathology and Cyst Structure
The echinococcal cyst (endocyst) has three layers:
- Pericyst (adventitia) — host-derived fibrous outer layer
- Ectocyst (laminated membrane) — acellular, outer parasitic layer; lamellar appearance on H&E
- Germinal (inner/endogenous) layer — the living cellular layer; produces brood capsules, protoscolices, and daughter cysts
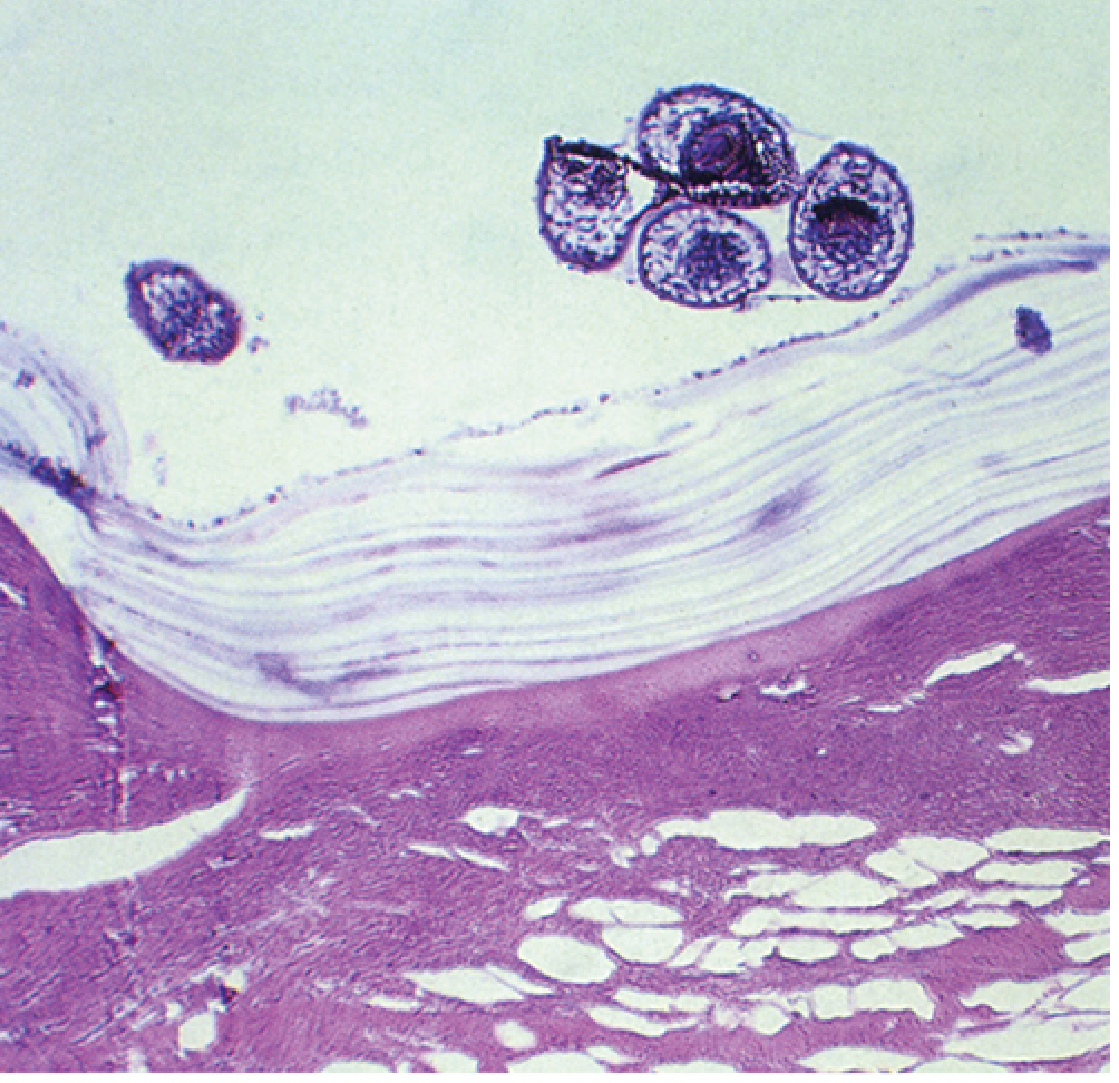
Key histological distinction:
- E. granulosus: thick outer laminated membrane + brood capsules with protoscolices — contained within a cyst
- E. multilocularis: infiltrative growth; back-to-back brood capsules without a thick containing laminated wall; protoscolices are usually absent in human infection
5. Clinical Manifestations
Cystic Echinococcosis (E. granulosus)
- Incubation/latency: 5–20 years (intervals up to 75 years reported) — most patients are asymptomatic until the cyst causes mechanical effects
- Liver (~70% of cases): upper abdominal discomfort/pain, nausea, hepatomegaly, palpable mass, jaundice (biliary compression/rupture), portal hypertension, ascites, IVC compression
- Lung (~25% of cases): cough, chest pain, hemoptysis; rupture into bronchi → vomiting of hydatid material (brood capsules, scolices), salty taste, pneumothorax, pleural effusion
- Brain (~4% of primary hepatic/pulmonary cases): seizures, blindness, raised ICP
- Bone: pathological fractures (bone cysts do not have a pericyst wall)
- Heart: cardiac mass, pericardial effusion, conduction disturbances, embolic metastases
- Rupture: fever, pruritus, urticaria, anaphylactic shock (major complication); seeding of protoscolices can cause secondary/disseminated echinococcosis
- Intrabiliary rupture: acute cholangitis, jaundice, signs mimicking acute cholecystitis
- Circulating immune complexes: rare membranous glomerulonephritis
Alveolar Echinococcosis (E. multilocularis)
- Almost invariably involves the liver
- Presents as a slowly expanding tumor-like mass over decades
- Symptoms: epigastric pain, obstructive jaundice, weight loss, malaise, liver failure
- Can metastasize hematogenously to lung and brain, closely mimicking hepatocellular carcinoma
- Fatal if untreated; 10-year mortality can exceed 90% without treatment
6. Diagnosis
Laboratory Tests
- Routine labs are nonspecific
- Eosinophilia: usually low-grade or absent unless cyst has ruptured (may reach up to 60% with rupture)
- Alkaline phosphatase elevation if biliary involvement
Imaging
Ultrasound is the primary diagnostic tool and the preferred modality for screening and follow-up in endemic areas.
The WHO/IWGE (Informal Working Group on Echinococcosis) standardized ultrasound classification:
| Stage | Description | Viability |
|---|---|---|
| CL | Cystic lesion, no distinct wall — may be non-parasitic | Unclear |
| CE1 | Unilocular cyst, distinct wall, may show "hydatid sand" (mobile echoes) | Active |
| CE2 | Multivesicular; internal septations ("rosette" / "honeycomb" pattern) | Active |
| CE3a | Detachment of endocyst ("water-lily sign") | Transitional |
| CE3b | Predominantly solid with daughter cysts; internal thickening | Transitional |
| CE4 | Heterogeneous; degenerated cyst contents (no daughter cysts) | Inactive |
| CE5 | Thick calcification (eggshell) | Inactive/dead |
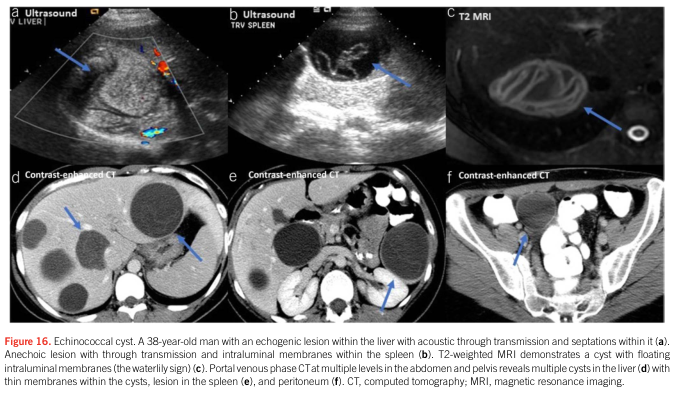
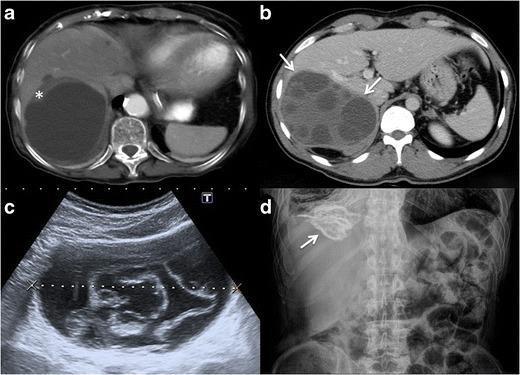
CT: superior for extrahepatic lesions, smaller cysts, precise localization, and surgical planning.
MRI: preferred for postsurgical residual assessment, cardiac/intracranial disease, and when ultrasound cannot be performed.
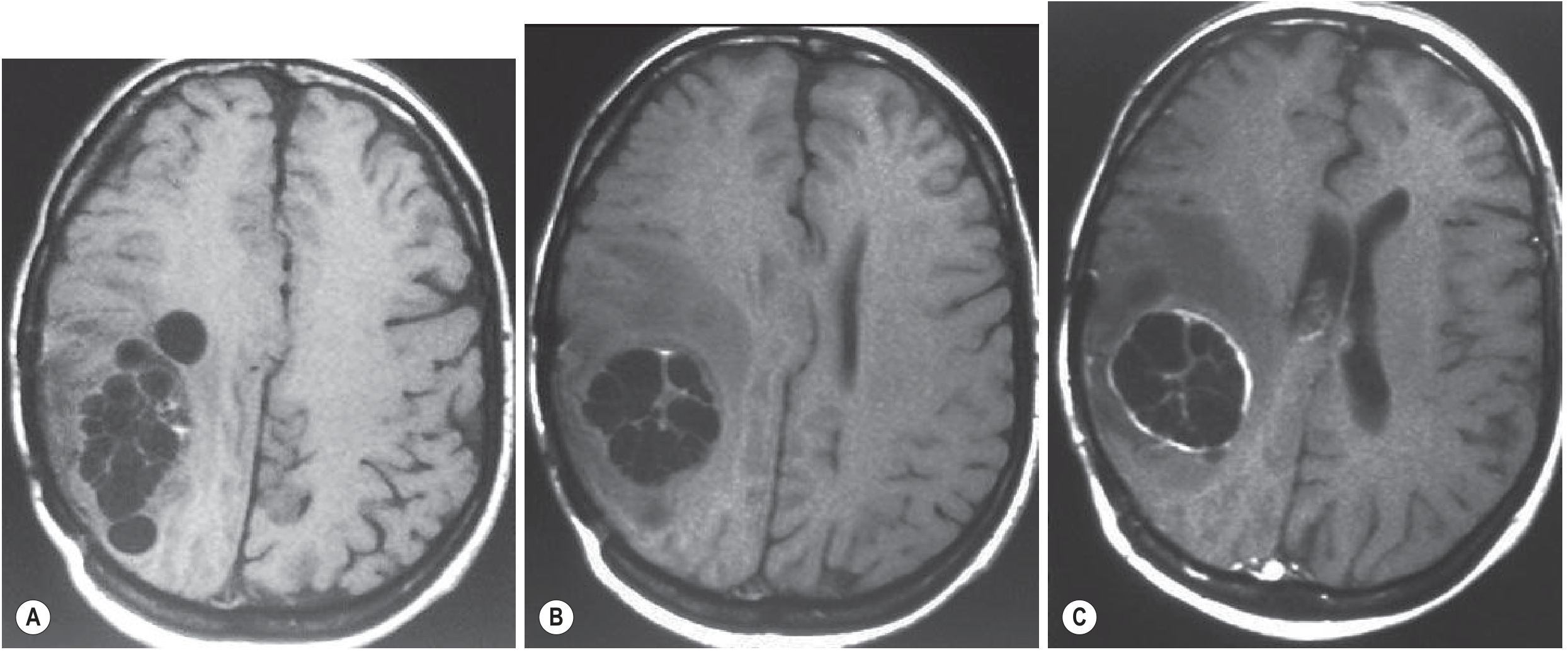
Brain MRI (CE): well-defined unilocular cysts with CSF-like fluid; thin rim enhancement and perifocal edema indicate active cyst.
Serology
- Useful as confirmatory, not primary diagnostic tool
- Sensitivity depends on cyst location: hepatic > pulmonary > splenic/brain/bone
- Indirect hemagglutination/latex agglutination: ~90% sensitivity for hepatic, ~60% for pulmonary lesions
- Generally negative in inactive cysts (CE4/CE5); titers rise after cyst disruption (surgery/PAIR)
- E. multilocularis patients are usually seropositive on E. granulosus assays; E. multilocularis-specific assays available in Europe
- False positives in neurocysticercosis (up to 25%)
PCR
- Can detect picogram quantities of Echinococcus genomic DNA from fine-needle biopsy material
- Valuable when serology is equivocal
Caution re: aspiration
- Blind needle aspiration is contraindicated due to risk of anaphylaxis and dissemination; however, ultrasound-guided PAIR is a therapeutic procedure (see below)
7. Treatment
Treatment selection depends on cyst species, anatomic location, stage (CE classification), cyst size, patient factors, and available expertise.
A. "Watch and Wait" (Inactive Cysts)
- Inactive liver cysts (CE4/CE5) free of complications can be monitored without intervention, with serial imaging
B. Chemotherapy (Albendazole — drug of choice)
- Dose: 10–15 mg/kg/day orally (continuous, no interruptions)
- Best for: CE1 and CE3a cysts (small/medium) — induces solidification
- Limited efficacy: giant CE1/CE3a (>10 cm), CE2 and CE3b (little effect alone)
- Adverse effects: hepatotoxicity, leukopenia, thrombocytopenia, alopecia
- Avoid in pregnancy (teratogenic risk theoretical, but standard precaution)
- For E. multilocularis: indefinite albendazole if not resectable; post-curative-surgery: 2 years to reduce relapse risk
C. PAIR (Percutaneous Aspiration–Injection–Re-aspiration)
- Indications: CE1 and CE3a cysts
- Procedure: ultrasound-guided percutaneous puncture → aspiration of cyst fluid → injection of scolicidal agent (hypertonic saline, ethanol) → re-aspiration
- Risk of anaphylaxis: 0.03% lethal; 1.7% reversible allergic reaction
- Always combined with albendazole (≥30 days post-procedure)
- PAIR is generally ineffective for multivesicular cysts (CE2, CE3b) — tend to relapse
- Various catheter drainage modifications exist for complex cysts
D. Surgery
Indications:
- Complicated cysts (rupture, biliary fistula, compression of vital structures, superinfection, hemorrhage)
- Large cysts with many daughter vesicles not amenable to PAIR
- High risk of rupture
- E. multilocularis (primary modality when feasible)
Peri-operative care: Albendazole 10–15 mg/kg/day from 1 week preoperatively to 4 weeks post-operatively (to minimize risk of secondary dissemination from spillage). Some add praziquantel (50 mg/kg/day or per week). Note: most experts avoid preoperative antiparasitic drugs for lung and CNS disease due to increased rupture risk.
For E. multilocularis: Radical excision of all infected tissue is the goal; may require liver transplantation in advanced cases.
E. Summary by Cyst Stage
| Stage | First-line |
|---|---|
| CL | No treatment or monitor |
| CE1 (small/medium) | Albendazole or PAIR + albendazole |
| CE2, CE3b | Surgery or modified percutaneous drainage + albendazole |
| CE3a (small/medium) | PAIR + albendazole or albendazole alone |
| CE4, CE5 (inactive, no complications) | Watch and wait |
| Complicated any stage | Surgery |
| E. multilocularis | Surgery + albendazole (±lifelong if inoperable) |
8. Prognosis
- Cystic echinococcosis: significant morbidity, death rare — long-term follow-up (>5 years) needed to assess for recurrence
- Alveolar echinococcosis: fatal if untreated; with benzimidazole treatment, survival approaches that of the age/sex-matched general population. Prognosis is poor if not diagnosed early.
9. Prevention and Control
- Deworming of dogs (praziquantel) in endemic areas
- Avoiding feeding raw viscera to dogs
- Hand hygiene; avoiding contamination from dog feces
- Food hygiene (washing vegetables; avoiding raw berries in fox-endemic areas)
- Surveillance and slaughterhouse control programs
- Vaccination of sheep (EG95 vaccine) has shown promise in breaking the pastoral cycle
Recent Evidence (PubMed)
A 2024 Cochrane systematic review (PMID: 38994714) assessed treatments for uncomplicated hepatic cystic echinococcosis and remains the most current high-level evidence synthesis on treatment outcomes. A 2023 systematic review (PMID: 37080264) covered diagnostic methods from 1999–2021.
Sources:
- Goldman-Cecil Medicine, International Edition — Chapters on Cystic and Alveolar Hydatid Disease
- Sherris & Ryan's Medical Microbiology, 8th Edition — Chapter 56: Cestodes
- Tietz Textbook of Laboratory Medicine, 7th Edition — Chapter 88: Echinococcus
- Grainger & Allison's Diagnostic Radiology — Chapters on CNS and Renal Hydatid Disease
Thrichecocci infection in detail
Checking Date & Time
Finding Sources
Finding Sources
Searching the Web
Thrichecocci infection parasitology medical
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.