Explain me penicillins group with each an every drugs and their mechanism indication dose contraindications drug of choice cases with example hoe to use this drugs each etc from basics to clinical
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative textbooks with structural diagrams. Let me now write the full, detailed clinical answer.
Penicillins - Complete Guide: Basics to Clinical
1. The Penicillin Nucleus - Understanding the Core Structure
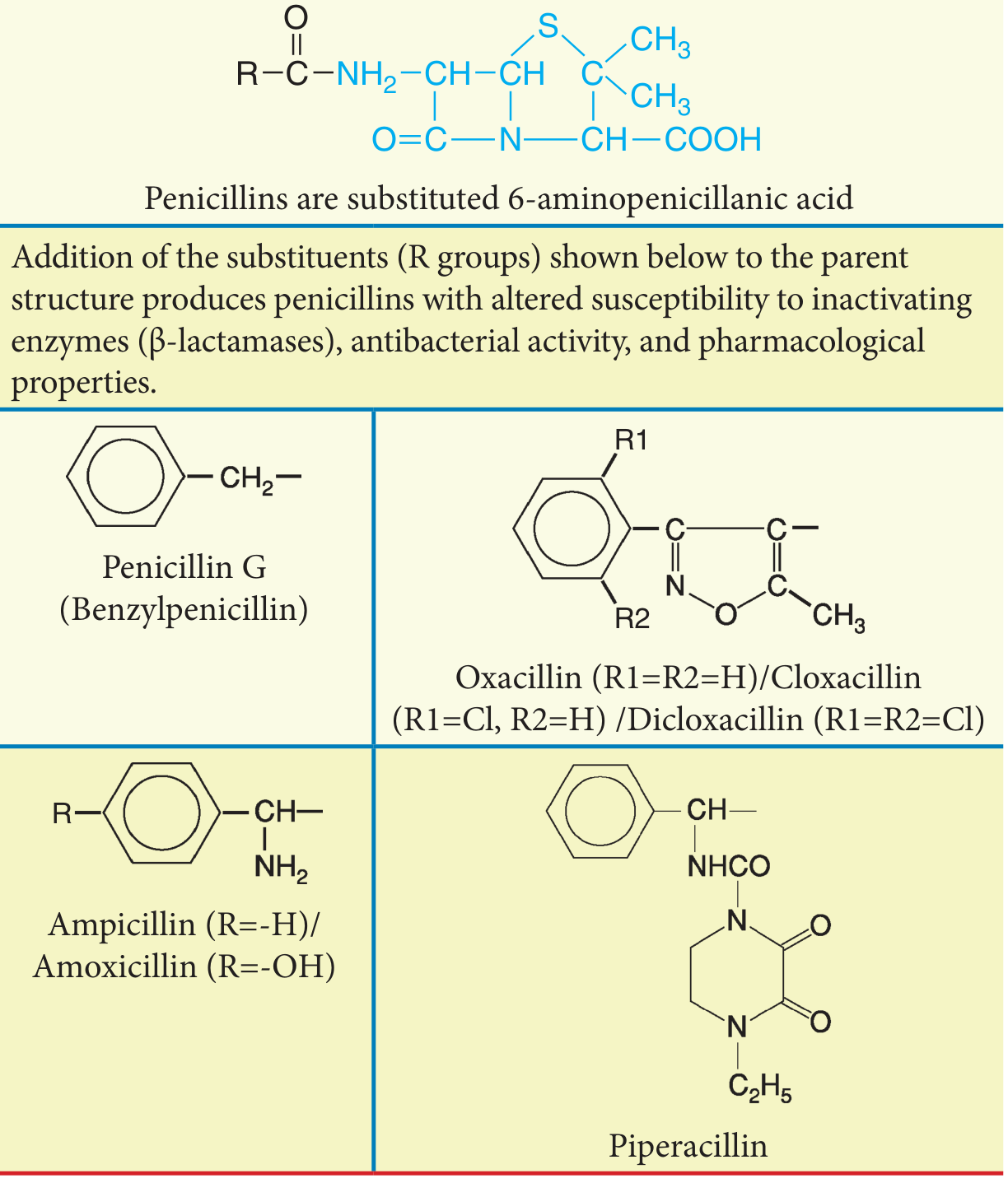
All penicillins are built on 6-aminopenicillanic acid (6-APA), which consists of two fused rings:
- Ring A = Thiazolidine ring
- Ring B = Beta-lactam ring (the pharmacologically active part)
- R group = Side chain that determines spectrum, acid stability, and resistance to beta-lactamases
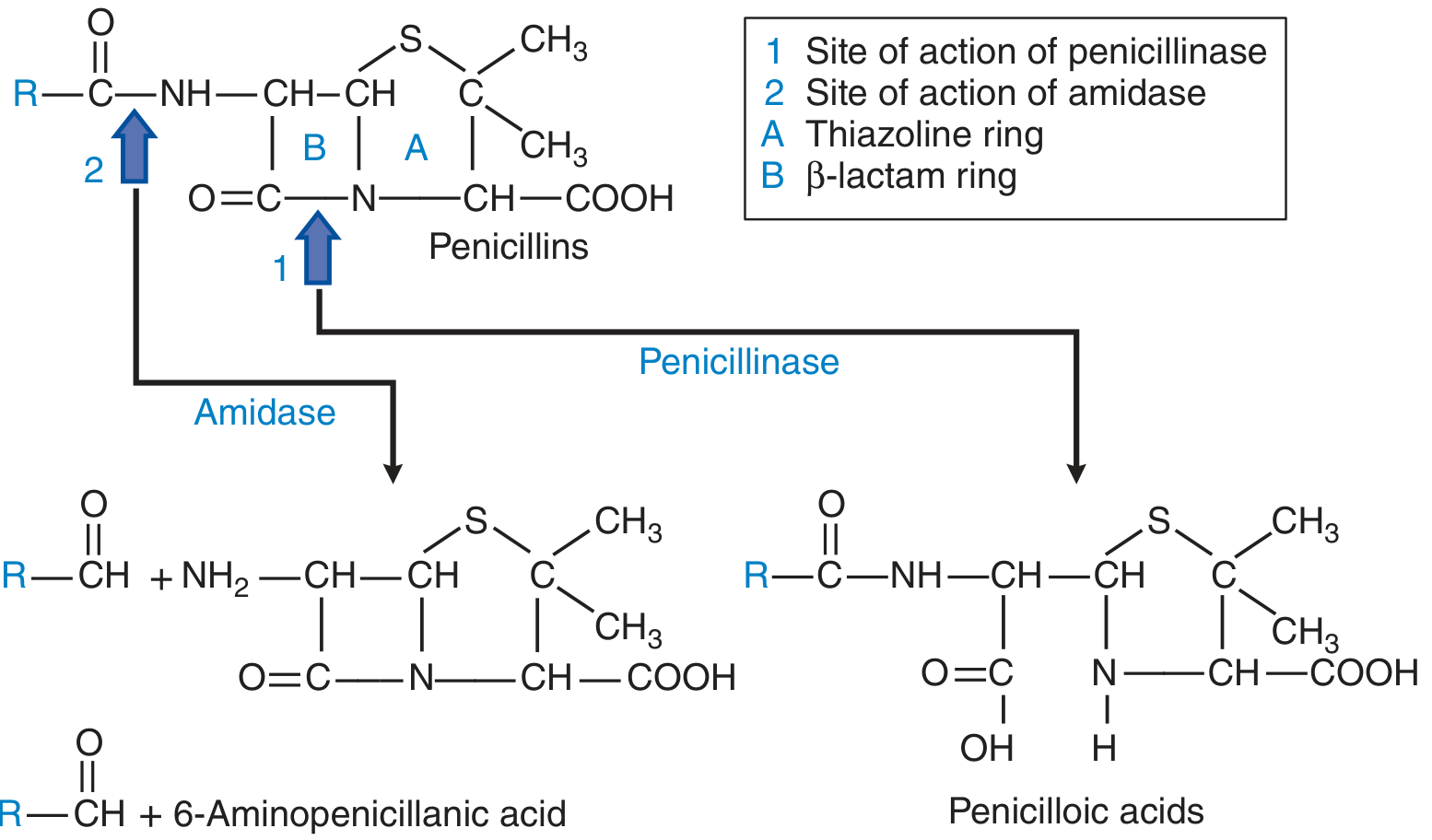
When penicillinase (beta-lactamase) cleaves the beta-lactam ring at site 1, the product is penicilloic acid - which has no antibacterial activity but IS antigenic (causing allergic reactions). When amidase cleaves at site 2, the free 6-APA nucleus is released.
2. Mechanism of Action
Penicillins are bactericidal (they kill bacteria, not just inhibit them). Here is the step-by-step mechanism:
Step 1 - Target identification:
Bacteria build their cell wall from peptidoglycan, a mesh of sugar chains (NAM-NAG) cross-linked by short peptide bridges.
Step 2 - Enzyme inhibition:
Cross-linking is performed by enzymes called Penicillin-Binding Proteins (PBPs) - specifically transpeptidases. Penicillin's beta-lactam ring mimics the D-Ala-D-Ala terminus of the peptide precursor. It binds irreversibly to the active site of PBPs, blocking transpeptidation.
Step 3 - Cell wall weakening:
Without cross-linking, new peptidoglycan cannot be synthesized. The growing cell wall becomes structurally defective.
Step 4 - Autolysis:
The bacteria's own autolytic enzymes (murein hydrolases) continue degrading old peptidoglycan while new synthesis is blocked. This leads to cell lysis and death.
Key points: Active only against actively dividing bacteria (you need ongoing cell wall synthesis). Completely ineffective against organisms without a cell wall (Mycoplasma, intracellular bacteria, fungi, viruses).
3. Classification of Penicillins
Penicillins fall into five groups based on their antimicrobial spectrum:
| Group | Drugs | Key Feature |
|---|---|---|
| 1. Natural Penicillins | Penicillin G, Penicillin V | Gram-positive, narrow spectrum |
| 2. Antistaphylococcal (Penicillinase-resistant) | Nafcillin, Oxacillin, Dicloxacillin, Cloxacillin | Resistant to staph beta-lactamase |
| 3. Aminopenicillins | Ampicillin, Amoxicillin | Extended to some gram-negatives |
| 4. Carboxypenicillins | Ticarcillin (largely discontinued) | Anti-Pseudomonal |
| 5. Ureidopenicillins | Piperacillin | Broadest spectrum, anti-Pseudomonal |
| +BLI combinations | Amoxicillin-clavulanate, Ampicillin-sulbactam, Piperacillin-tazobactam | Overcome beta-lactamase resistance |
4. Group-by-Group Drug Details
GROUP 1 - Natural Penicillins
A. Penicillin G (Benzylpenicillin)
Spectrum:
- Gram-positive cocci: Streptococcus pyogenes (Group A Strep), viridans streptococci, Streptococcus pneumoniae (penicillin-sensitive strains)
- Gram-positive rods: Clostridium spp., Actinomyces israelii, Listeria monocytogenes
- Gram-negative cocci: Neisseria meningitidis (meningococcus - almost always sensitive), some Neisseria gonorrhoeae (most are now resistant)
- Spirochetes: Treponema pallidum (syphilis), Leptospira spp., Borrelia burgdorferi (Lyme)
- Anaerobes (NOT Bacteroides fragilis)
Route: IV or IM only - acid labile, destroyed by stomach acid, cannot be given orally.
Formulations and Doses:
| Formulation | Route | Dose | Duration of Action | Use |
|---|---|---|---|---|
| Penicillin G aqueous | IV | 2-4 million units q4-6h (up to 24 million units/day for severe infection) | Minutes-hours | Serious/severe infections |
| Penicillin G procaine | IM | 600,000 units IM once or twice daily | 12-24 hours | Moderate infections, outpatient |
| Penicillin G benzathine | IM | 1.2-2.4 million units single dose | 10-21 days | Strep pharyngitis, syphilis prophylaxis |
How benzathine/procaine works: These are repository (depot) formulations. Procaine and benzathine are poorly soluble salts that dissolve slowly at the IM injection site, releasing penicillin G gradually. Benzathine gives detectable levels for up to 3-4 weeks from one injection.
Drug of Choice (DOC) clinical cases:
- Syphilis (all stages): Benzathine Pen G 2.4 million units IM x1 (primary/secondary), x3 weekly doses (latent/tertiary)
- Strep pharyngitis (Group A): Benzathine Pen G 1.2 million units IM x1
- Rheumatic fever prophylaxis: Benzathine Pen G 1.2 million units IM every 3-4 weeks
- Meningococcal meningitis: Penicillin G 4 million units IV q4h x 7-10 days
- Gas gangrene (Clostridium): Penicillin G 3-4 million units IV q4h + surgical debridement
- Leptospirosis (severe): Penicillin G 1.5 million units IV q6h
- Actinomycosis: Penicillin G 10-20 million units/day IV x 4-6 weeks, then oral Pen V
Contraindications/Precautions:
- Allergy to penicillin (anaphylaxis, urticaria, serum sickness) - ABSOLUTE
- Procaine allergy (for procaine Pen G)
- Electrolyte caution: Large IV doses contain sodium or potassium - monitor in renal failure and heart failure
B. Penicillin V (Phenoxymethylpenicillin)
Differs from Pen G: Acid-stable (can be given orally). Produces 2-5x higher plasma levels than oral Pen G. But bioavailability is still modest, requires QID dosing, narrow spectrum - so amoxicillin is often preferred.
Route: Oral only
Dose: 250-500 mg orally every 6 hours (take on empty stomach - food impairs absorption)
Uses:
- Mild streptococcal pharyngitis
- Mild odontogenic (dental) infections
- Step-down therapy after IV penicillin G
- NOT suitable for serious infections
DOC example:
- Mild strep throat in a child (who can swallow pills): Pen V 250 mg QID x 10 days
GROUP 2 - Penicillinase-Resistant (Antistaphylococcal) Penicillins
The isoxazolyl ring (in oxacillin, dicloxacillin, cloxacillin) creates steric hindrance that prevents beta-lactamase from cleaving the beta-lactam ring.
Spectrum:
- S. aureus (MSSA - methicillin-susceptible) - this is their main target
- Streptococci (but less active than Pen G)
- NOT effective against MRSA (different resistance mechanism - altered PBP2a)
- NOT active against gram-negatives, enterococci, Listeria
A. Nafcillin
- Route: IV only (oral absorption erratic)
- Dose: 1-2 g IV every 4-6 hours (total 8-12 g/day for serious infections)
- Unique pharmacology: Hepatic elimination (not renal) - preferred in renal failure
- Uses/DOC: Serious MSSA infections - bacteremia, endocarditis, osteomyelitis, septic arthritis, skin and soft tissue infections, meningitis
Clinical case example: 45-year-old IV drug user presents with fever, new murmur, and echocardiogram showing vegetation on tricuspid valve. Blood cultures grow MSSA. Treatment: Nafcillin 2 g IV q4h x 6 weeks for right-sided endocarditis.
B. Oxacillin
- Route: IV only
- Dose: 1-2 g IV every 4-6 hours
- Eliminated by: Both hepatic and renal routes
- Uses: Same as nafcillin - serious MSSA infections
C. Dicloxacillin
- Route: Oral (acid stable, good bioavailability)
- Dose: 250-500 mg orally every 6 hours (taken 1 hour before meals - food reduces absorption)
- Uses/DOC: Mild-moderate localized MSSA infections - cellulitis, mild skin and soft tissue infections, step-down from IV nafcillin/oxacillin
Clinical case example: Patient is discharged after 5 days of IV nafcillin for MSSA cellulitis. Step-down: Dicloxacillin 500 mg PO q6h x 10 days total.
D. Cloxacillin / Flucloxacillin
- Available in many countries (not US), same spectrum as dicloxacillin
- Flucloxacillin 500 mg QID PO or IV, widely used in UK/Australia for MSSA
Why not use these for MRSA? MRSA has acquired the mecA gene, which encodes an altered PBP called PBP2a with very low affinity for all penicillins (and most beta-lactams). No modification of the R-group overcomes this - hence vancomycin is used for MRSA.
GROUP 3 - Aminopenicillins
An amino group (-NH₂) is added to the R side chain. This allows penetration through the outer membrane of gram-negative bacteria, extending the spectrum. However, these drugs ARE susceptible to beta-lactamases.
Spectrum (compared to Pen G - adds):
- E. coli, Proteus mirabilis, Haemophilus influenzae, Shigella, Salmonella, Enterococcus faecalis
- Still active against Strep, Listeria
- NOT Pseudomonas, Klebsiella, most gram-negative nosocomial pathogens
A. Ampicillin
- Route: IV/IM (oral absorption poor and variable)
- Dose: 1-2 g IV q4-6h for moderate infections; up to 12 g/day for meningitis
- Half-life: ~1 hour; renal excretion (dose adjust in renal failure)
DOC cases:
- Listeria monocytogenes meningitis (especially neonates and immunocompromised/elderly): Ampicillin 2 g IV q4h + gentamicin
- Enterococcal endocarditis: Ampicillin 2 g IV q4h + gentamicin x 4-6 weeks
- Neonatal meningitis (empiric, covers Listeria + GBS + gram-negatives): Ampicillin + cefotaxime
Clinical case example: 70-year-old diabetic with fever and CSF showing gram-positive rods, confirmed as Listeria monocytogenes. Treatment: Ampicillin 2 g IV q4h x 21 days + gentamicin for synergy.
B. Amoxicillin
- Route: Oral only (much better absorbed than ampicillin - 80% vs 40%)
- Dose:
- Standard: 500 mg PO TID or 875 mg PO BID
- High-dose (for drug-resistant Strep pneumoniae): 1 g TID
- H. pylori: 1 g BID (as part of triple/quadruple therapy)
- Food effect: Can be taken with food (unlike most penicillins) - this is clinically useful for compliance
- Same spectrum as ampicillin but oral bioavailability is the key advantage
DOC cases:
- Community-acquired pneumonia (outpatient, mild): Amoxicillin 1 g TID x 5-7 days (adults) or 90 mg/kg/day (children)
- Acute otitis media: Amoxicillin 80-90 mg/kg/day divided BID x 10 days (high dose for penicillin-resistant Strep pneumo)
- Strep pharyngitis (preferred oral agent): Amoxicillin 500 mg BID x 10 days
- H. pylori eradication: Amoxicillin 1 g BID + clarithromycin 500 mg BID + PPI x 14 days
- Lyme disease (early localized): Amoxicillin 500 mg TID x 14-21 days
- Dental infections (mild-moderate): Amoxicillin 500 mg TID x 5-7 days
Clinical case example: 5-year-old with fever, ear pulling, and bulging tympanic membrane (otitis media). First episode, no antibiotics in past month. Treatment: Amoxicillin 90 mg/kg/day in 2 divided doses x 10 days (high dose because up to 40% of Strep pneumoniae has reduced sensitivity).
GROUP 4/5 - Extended-Spectrum: Carboxypenicillins & Ureidopenicillins
Piperacillin (Ureidopenicillin)
This is the clinically relevant member (carbenicillin, ticarcillin largely discontinued in US).
Spectrum: The broadest of all penicillins:
-
All of ampicillin's coverage PLUS
-
Pseudomonas aeruginosa
-
More gram-negatives: E. coli, Klebsiella, Proteus, Enterobacter, many Bacteroides
-
Retains activity against enterococci and Listeria
-
Route: IV only
-
Dose: 3-4 g IV q4-6h (typically given as piperacillin-tazobactam combination - see below)
-
Alone it is susceptible to beta-lactamases, so rarely used without tazobactam
GROUP 6 - Beta-Lactamase Inhibitor Combinations
These add a beta-lactamase inhibitor (BLI) that has weak or no intrinsic antibacterial activity but protects the penicillin from enzymatic destruction. They bind irreversibly to beta-lactamases, acting as "suicide inhibitors."
| Drug | Penicillin | BLI | Route |
|---|---|---|---|
| Amoxicillin-clavulanate (Augmentin) | Amoxicillin | Clavulanic acid | Oral |
| Ampicillin-sulbactam (Unasyn) | Ampicillin | Sulbactam | IV/IM |
| Piperacillin-tazobactam (Pip-Tazo, Zosyn) | Piperacillin | Tazobactam | IV |
| Ticarcillin-clavulanate | Ticarcillin | Clavulanic acid | IV (not available US) |
A. Amoxicillin-Clavulanate (Augmentin)
- Doses:
- Standard: 875/125 mg PO BID
- High-dose: 2000/125 mg (Augmentin XR) BID for resistant Strep pneumo
- Pediatric: 45 mg/kg/day (amoxicillin component) divided BID using 600/42.9 mg/5mL suspension
- Spectrum adds (beyond amoxicillin): Beta-lactamase-producing H. influenzae, Moraxella catarrhalis, S. aureus (MSSA), many gram-negatives
- GI side effects are common - take with food to minimize diarrhea (clavulanate causes GI upset)
DOC cases:
- Acute bacterial sinusitis (first choice): Amox-clav 875/125 mg BID x 5-7 days
- Animal/human bites: Amox-clav 875/125 mg BID x 5 days (covers Pasteurella, oral flora)
- Community-acquired pneumonia in patients with comorbidities: Amox-clav + macrolide
- Acute otitis media, failed first-line amoxicillin: Amox-clav high dose
Clinical case example: 8-year-old with dog bite on hand, moderate depth wound. Treatment: Amoxicillin-clavulanate 45 mg/kg/day BID x 5 days (covers Pasteurella multocida from dog saliva + skin flora).
B. Ampicillin-Sulbactam (Unasyn)
- Dose: 3 g (2 g ampicillin + 1 g sulbactam) IV q6h; adjust for renal failure
- Special feature: Sulbactam itself has intrinsic activity against Acinetobacter baumannii - important in high-dose use for MDR Acinetobacter
- Spectrum: Amoxicillin-clav spectrum but parenteral; covers oral and GI flora well, NOT Pseudomonas
DOC/Common use cases:
- Intra-abdominal infections (mild-moderate): Amp-sulbactam 3 g IV q6h
- Aspiration pneumonia/lung abscess: Amp-sulbactam 3 g IV q6h (covers oral anaerobes)
- Pelvic inflammatory disease: Part of inpatient regimen
- Soft tissue infections with mixed flora
Clinical case example: 55-year-old alcoholic, found obtunded, chest X-ray shows right lower lobe infiltrate with cavitation, sputum has foul odor. Diagnosis: aspiration pneumonia/lung abscess. Treatment: Ampicillin-sulbactam 3 g IV q6h x 4-6 weeks (covers mouth anaerobes including Bacteroides, Peptostreptococcus).
C. Piperacillin-Tazobactam (Pip-Tazo / Zosyn)
- Dose: 3.375 g (3 g pip + 0.375 g tazo) IV q6h standard; 4.5 g q6h or q8h for Pseudomonas; 4.5 g extended infusion over 3-4 hours q8h (pharmacokinetic optimization for serious gram-negative infections)
- Spectrum: The broadest penicillin available: gram-positives, gram-negatives, anaerobes, Pseudomonas. Covers most hospital-acquired pathogens except MRSA, Acinetobacter, ESBL-producers
- Adjust: Renal dosing required (renally cleared); monitor for hypokalemia (nephrotoxicity with vancomycin)
DOC/Common use cases:
- Healthcare-associated pneumonia / ventilator-associated pneumonia (VAP): Pip-Tazo 4.5 g q8h extended infusion
- Febrile neutropenia (empiric): Pip-Tazo 4.5 g q6h as monotherapy
- Intra-abdominal infection (severe/hospital-acquired): Pip-Tazo 3.375 g q6h
- Diabetic foot infection (moderate-severe): Pip-Tazo 4.5 g q8h
- Hospital-acquired urinary tract infection
- Sepsis of unknown source in hospitalized patients
Clinical case example: A 60-year-old on chemotherapy develops fever (38.9°C) and absolute neutrophil count of 200 cells/µL. Diagnosis: Febrile neutropenia. Empiric treatment: Piperacillin-tazobactam 4.5 g IV q6h (or q8h extended infusion) until cultures return or fever resolves and ANC recovers.
5. Pharmacokinetics Summary
| Property | Details |
|---|---|
| Distribution | Wide - joints, pleura, pericardium, bile |
| Protein binding | Nafcillin highest (>90%) → lower free drug; Pen G, ampicillin lower binding |
| CNS penetration | <1% normal meninges; up to 5% with inflamed meninges |
| Prostate/eye | Poor penetration |
| Elimination | Primarily renal (tubular secretion ~90%, GF ~10%); half-life ~30 min for Pen G |
| Exception | Nafcillin - hepatic elimination (safe in renal failure without dose adjustment) |
| Time-dependent killing | Penicillins are TIME-dependent bactericidals - what matters is the % of time free drug is above MIC (not peak concentration). This is why extended infusions or frequent dosing intervals are used. |
Probenecid: Blocks renal tubular secretion of penicillins → increases and prolongs serum levels. Historically used to boost levels (e.g., in syphilis treatment where benzathine was scarce).
Oral absorption tips:
- Amoxicillin: Take with OR without food
- Dicloxacillin, penicillin V, ampicillin: Take on empty stomach (1 hour before or 2 hours after food)
6. Resistance Mechanisms
There are four ways bacteria resist penicillins:
-
Beta-lactamase production (most common) - enzyme cleaves the beta-lactam ring. Countered by: penicillinase-resistant penicillins (Group 2), or BLI combinations.
-
Altered PBPs (target modification) - MRSA has PBP2a (low affinity for all beta-lactams). Penicillin-resistant Strep pneumoniae has altered PBP2b/2x. Cannot be overcome by any penicillin.
-
Efflux pumps - bacteria pump the drug out (e.g., Pseudomonas). Piperacillin partially overcomes this.
-
Reduced outer membrane permeability - gram-negatives lose porin channels that allow penicillin entry (e.g., Pseudomonas, imipenem-resistant Enterobacter).
7. Adverse Effects
Allergy (most important adverse effect)
| Type | Presentation | Timing | Management |
|---|---|---|---|
| Immediate (Type I, IgE-mediated) | Anaphylaxis, urticaria, angioedema, bronchospasm | Within 1 hour | Stop drug; epinephrine 0.3 mg IM; ICU |
| Accelerated urticarial | Urticaria, fever | 1-72 hours | Stop drug; antihistamines |
| Late (Type III/IV) | Serum sickness, maculopapular rash, hemolytic anemia | >72 hours | Stop drug; steroids if severe |
- Cross-reactivity with cephalosporins: ~1-2% (older estimates of 10% were overestimates). Related to shared R1 side chain, not the beta-lactam ring. If true anaphylaxis to penicillin, avoid cephalosporins with similar side chains; carbapenems have ~1% cross-reactivity.
- Maculopapular rash with ampicillin/amoxicillin: ~5-10% of patients; up to 80-100% in patients with EBV mononucleosis or CLL. NOT a true allergic reaction - do NOT label as penicillin allergy. Due to immune complex deposition.
- Antibiotic allergy delabeling: Many patients labeled "penicillin allergic" are NOT truly allergic. Penicillin skin testing + graded challenge is the standard approach to delabel.
Other Adverse Effects
| Effect | Drug(s) | Notes |
|---|---|---|
| Diarrhea | Amoxicillin-clavulanate most common | Clavulanate causes GI upset; take with food |
| C. difficile colitis | All (any antibiotic) | Particularly with broad-spectrum agents |
| Neurotoxicity/seizures | High-dose IV Pen G | Especially in renal failure - can't clear drug fast enough |
| Hypokalemia | Piperacillin-tazo | Monitor electrolytes |
| Interstitial nephritis | Methicillin (major reason discontinued), nafcillin | Immune-mediated |
| Hepatotoxicity | Oxacillin | Transaminase elevation |
| Neutropenia | Nafcillin | With prolonged use |
| Jarisch-Herxheimer reaction | Penicillin G (syphilis) | Fever, chills, myalgias 2-8 hours after first dose; due to cytokine release from dying spirochetes; NOT allergy; managed with NSAIDs |
8. Contraindications
| Contraindication | Details |
|---|---|
| Prior severe penicillin allergy | Anaphylaxis, Stevens-Johnson syndrome - absolute contraindication to any penicillin |
| Renal failure (without dose adjustment) | Dose must be reduced for all renally cleared penicillins (exception: nafcillin) |
| High-dose Pen G in hypokalemia/hypernatremia | Large IV doses contain significant sodium - caution in heart failure, hypertension |
| Infectious mononucleosis | Avoid ampicillin/amoxicillin (causes severe rash) |
| MRSA infection | No penicillin is effective against MRSA |
9. Drug Interactions
| Interaction | Mechanism | Clinical significance |
|---|---|---|
| Probenecid | Blocks tubular secretion | Raises/prolongs penicillin levels - used therapeutically |
| Methotrexate | Penicillins reduce MTX renal clearance | Increased MTX toxicity - monitor |
| Warfarin | Altered gut flora, reduced vitamin K | Enhanced anticoagulation - monitor INR |
| Oral contraceptives | Disruption of enterohepatic cycling (theoretical, clinically minor) | Counsel patients |
| Aminoglycosides | Chemical inactivation if mixed in same IV line | Never mix in same syringe; synergistic if given separately |
| Bacteriostatic antibiotics | May antagonize penicillin's bactericidal action (theoretical) | Usually clinically insignificant |
10. Pregnancy and Special Populations
- Pregnancy: Penicillins are Category B - considered safest antibiotics in pregnancy. Used for GBS prophylaxis in labor (Pen G 5 million units IV load, then 2.5-3 million units IV q4h until delivery).
- Neonates: Dose by gestational age and postnatal age (different tables for PMA <34 weeks). Ampicillin + gentamicin is standard neonatal sepsis empiric therapy.
- Renal failure: Reduce dose/extend interval for all penicillins EXCEPT nafcillin. Rule of thumb: if CrCl <10 mL/min, give 1/4 to 1/3 of normal dose.
- Hepatic failure: Nafcillin requires dose adjustment (hepatic clearance); others are generally safe.
- Dialysis patients: Give after dialysis (penicillins are dialyzable).
11. Quick Reference - Drug of Choice Summary
| Infection | Preferred Penicillin | Dose / Duration |
|---|---|---|
| Streptococcal pharyngitis | Penicillin V PO or Amoxicillin PO | Pen V 500 mg QID x 10d or Amox 500 mg BID x 10d |
| Strep throat (single shot) | Benzathine Pen G IM | 1.2 million units IM x1 |
| Rheumatic fever prophylaxis | Benzathine Pen G IM | 1.2 million units IM q3-4 weeks |
| Syphilis (primary/secondary) | Benzathine Pen G IM | 2.4 million units IM x1 |
| Syphilis (neurosyphilis) | Penicillin G IV | 3-4 million units q4h x 10-14 days |
| Meningococcal meningitis | Penicillin G IV | 4 million units q4h x 7-10 days |
| Pneumococcal pneumonia (sensitive) | Penicillin G or Amoxicillin | Pen G 1-2 million units IV q4h or Amox 500 mg TID |
| Enterococcal endocarditis | Ampicillin IV + gentamicin | Ampicillin 2 g q4h x 4-6 weeks |
| Listeria meningitis | Ampicillin IV + gentamicin | Ampicillin 2 g q4h x 21 days |
| MSSA bacteremia/endocarditis | Nafcillin or Oxacillin IV | 2 g q4h x 4-6 weeks |
| MSSA cellulitis (outpatient) | Dicloxacillin PO | 500 mg q6h x 5-10 days |
| Strep pharyngitis + sinusitis | Amoxicillin-clavulanate | 875/125 mg BID x 5-7 days |
| Animal bites | Amoxicillin-clavulanate | 875/125 mg BID x 5-7 days |
| Aspiration pneumonia | Ampicillin-sulbactam IV | 3 g q6h x 7-10 days |
| Febrile neutropenia | Piperacillin-tazobactam IV | 4.5 g q6h until ANC recovery |
| Hospital-acquired pneumonia | Piperacillin-tazobactam IV | 4.5 g q8h extended infusion |
| Community-acquired UTI | Amoxicillin-clavulanate or Amoxicillin | 500 mg TID x 3-7 days (check local susceptibility) |
| H. pylori (triple therapy) | Amoxicillin + clarithromycin + PPI | Amox 1 g BID x 14 days |
| GBS prophylaxis in labor | Penicillin G IV | 5 million units load, then 2.5-3 million units q4h |
| Gas gangrene | Penicillin G IV + surgical debridement | 3-4 million units q4h x 10-14 days |
| Lyme disease (early) | Amoxicillin | 500 mg TID x 14-21 days |
| Otitis media | Amoxicillin high dose | 90 mg/kg/day BID x 10 days (children) |
12. How to Think About Penicillin Choice Clinically
Ask these 4 questions:
-
What organism am I treating?
- Strep/meningococcus/spirochete → Pen G or Pen V or Amoxicillin
- Staph (MSSA) → Nafcillin/Oxacillin (IV) or Dicloxacillin (oral)
- MRSA? → No penicillin works; use vancomycin/daptomycin
- Mixed gram-negative (non-Pseudomonal) → Ampicillin-sulbactam or Amox-clav
- Pseudomonas risk → Piperacillin-tazobactam
-
What site is infected (and what route can I use)?
- CNS/meningitis → High-dose IV Pen G (if sensitive organism) for CSF penetration
- Oral outpatient → Amoxicillin, Amox-clav, Pen V, Dicloxacillin
- Serious systemic → IV route required (Pen G, Nafcillin, Ampicillin, Pip-Tazo)
-
What is the local resistance pattern?
- Check antibiogram for local MSSA rate, ESBL rates, Pseudomonas susceptibility
- High-dose amoxicillin for Strep pneumo (overcomes intermediate resistance by achieving levels above MIC)
-
What are the patient's limitations?
- Renal failure → Nafcillin preferred; adjust others
- Pen allergy → Use azithromycin (strep throat), vancomycin (MSSA), fluoroquinolones (respiratory), or do penicillin allergy workup/delabeling
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Katzung's Basic and Clinical Pharmacology 16th Ed., Jawetz Melnick & Adelberg's Medical Microbiology 28th Ed., The Harriet Lane Handbook 23rd Ed.
I don't want like this I don't want textbook things i need only clinical knowledge which helps me in my OPD
Asking for Preferences
Here's your pure OPD clinical guide - no theory, just real decisions.
Penicillins in Your OPD - What to Prescribe and How
The 5 Penicillins You Actually Use in OPD
Forget the rest. These are the ones in your hands:
| Drug | Brand examples | Form | When you reach for it |
|---|---|---|---|
| Amoxicillin | Mox, Novamox, Amoxil | Capsule, syrup | Your most-used penicillin |
| Amoxicillin-Clavulanate | Augmentin, Clavam | Tablet, syrup | When amoxicillin alone won't work |
| Phenoxymethylpenicillin (Pen V) | Ospen | Tablet | Step-down after IV, simple strep |
| Dicloxacillin / Cloxacillin | Distaclor, Bioclox | Capsule | Skin infections, boils, MSSA |
| Ampicillin | Penbritin | Capsule (rarely oral now) | Mostly replaced by amoxicillin |
OPD Scenario 1 - Patient with Throat Pain, Fever, No Cough
Your diagnosis: Streptococcal tonsillitis / pharyngitis
Prescribe:
Amoxicillin 500 mg - 1 capsule 3 times a day x 10 days
(Take any time, with or without food)
Pediatric version:
Amoxicillin syrup 250 mg/5 mL
Weight under 20 kg: 40 mg/kg/day in 3 divided doses x 10 days
Practical: 5 mL three times a day for a 15 kg child
Tell the patient: "Take the full 10 days even if you feel better in 3 days. Stopping early causes relapse and can damage the heart (rheumatic fever)."
If they come back after 3 days - not better:
Switch to Amoxicillin-Clavulanate (beta-lactamase producing organisms from the throat flora are blocking amoxicillin).
If they are allergic to penicillin: Azithromycin 500 mg day 1, then 250 mg days 2-5.
OPD Scenario 2 - Ear Pain, Child Crying, Bulging Eardrum (Otitis Media)
Prescribe:
Amoxicillin 80-90 mg/kg/day in 2 divided doses x 10 days
(High dose - important, don't underdose)
Example for a 12 kg child:
Amoxicillin 250 mg/5 mL syrup
7 mL twice daily x 10 days (= ~87 mg/kg/day)
Why high dose? 30-40% of Strep pneumoniae in India/South Asia has reduced penicillin sensitivity. High-dose amoxicillin still kills them by pushing drug concentration above MIC.
If no improvement in 48-72 hours or child had amoxicillin recently:
Switch to Amoxicillin-Clavulanate (covers beta-lactamase producing H. influenzae and Moraxella that are a second cause of treatment failure).
OPD Scenario 3 - Runny Nose + Facial Pain/Heaviness + Fever > 10 Days (Sinusitis)
Prescribe:
Amoxicillin-Clavulanate 625 mg (500/125 mg) - 1 tablet twice daily x 5-7 days
(Take WITH food - reduces stomach upset from clavulanate)
Or high-dose for worse cases / previous treatment failure:
Amoxicillin-Clavulanate 1000/62.5 mg (Augmentin XR or Clavam 1000) - 1 tablet twice daily x 7 days
Do NOT prescribe amoxicillin alone for sinusitis - the main pathogens here (H. influenzae, Moraxella) often produce beta-lactamase.
OPD Scenario 4 - Skin Infection: Cellulitis, Abscess, Boil, Infected Wound
This is where many doctors go wrong. There are TWO very different bugs:
A. Streptococcal cellulitis (spreading redness, warmth, no central pus, no fluctuance)
Amoxicillin-Clavulanate 625 mg twice daily x 7 days
OR
Cloxacillin / Dicloxacillin 500 mg four times a day x 7 days
(Take on EMPTY stomach - 1 hour before meals)
B. Staphylococcal abscess/boil (pus, fluctuant, central necrosis)
- First: drain it. The antibiotic is secondary.
- After drainage:
Cloxacillin 500 mg 4 times a day x 5 days
OR Dicloxacillin 500 mg 4 times a day x 5 days
Important: If the patient was on regular amoxicillin or amoxicillin-clavulanate and is NOT improving - think MRSA. Switch to co-trimoxazole (TMP-SMX) or clindamycin. Refer if systemic signs.
Red flags that need IV/hospital:
- Fever > 38.5°C + cellulitis spreading fast
- Periorbital/orbital cellulitis
- Necrotizing features (dusky skin, crepitus, extreme pain)
OPD Scenario 5 - Chest Infection / Community-Acquired Pneumonia (CAP)
Mild CAP (patient can walk in, no hypoxia, no confusion):
Amoxicillin 1 g - 1 tablet 3 times a day x 5 days
If the patient has diabetes, COPD, or was recently on antibiotics:
Amoxicillin-Clavulanate 625 mg twice daily x 5-7 days
+ Azithromycin 500 mg once daily x 3-5 days (to cover atypicals)
When to send to hospital (not for OPD penicillin):
Use CURB-65: Confusion + Urea >7 mmol/L + RR >30 + BP <90/60 + Age >65. Score 2+ → refer.
OPD Scenario 6 - Urinary Tract Infection (UTI)
Be careful here. Penicillins are NOT first-line for UTI in most regions now because E. coli resistance is very high (>50% in South Asia). Nitrofurantoin or Fosfomycin are better choices.
However, if culture shows E. coli/Enterococcus sensitive to amoxicillin:
Amoxicillin 500 mg 3 times a day x 5-7 days (women, uncomplicated)
x 10-14 days (men, complicated)
Never prescribe amoxicillin blind for UTI without culture.
OPD Scenario 7 - Dental Infection (Abscess, Cellulitis from Tooth)
Prescribe:
Amoxicillin-Clavulanate 625 mg twice daily x 5 days
If they are on metronidazole already (from dentist):
Add amoxicillin 500 mg TID - the combination covers oral anaerobes very well.
Dog/Cat/Human bite:
Amoxicillin-Clavulanate 625 mg twice daily x 5 days
(Start within 12 hours of bite)
Cover tetanus too. Human bites are nastier than dog bites.
OPD Scenario 8 - Pregnant Patient with Infection
Penicillins are the SAFEST antibiotics in pregnancy (Category B - used for decades).
- Throat/ear/sinus: Amoxicillin 500 mg TID (safe in all trimesters)
- Skin infection: Amoxicillin-clavulanate (safe)
- GBS carrier (if you have her antenatal records): Refer for IV Pen G in labor
Avoid fluoroquinolones, tetracyclines - use penicillins confidently in pregnancy.
The One Question You Always Ask Before Prescribing
"Are you allergic to penicillin or amoxicillin?"
If yes - ask what happened:
- "I got a rash" → Was it the pink blotchy rash on amoxicillin? That's NOT allergy (especially if they had mono/viral infection). You can likely still use it with caution.
- "My throat closed / I couldn't breathe / I needed injection in emergency" → TRUE anaphylaxis. Never give any penicillin. Use alternatives.
Alternatives if truly allergic:
| For | Use |
|---|---|
| Strep throat | Azithromycin 500 mg day 1, then 250 mg x 4 days |
| Skin infection (MSSA) | Co-trimoxazole DS twice daily OR Clindamycin |
| CAP | Azithromycin OR Levofloxacin |
| Sinusitis/otitis | Azithromycin OR Levofloxacin |
How to Write the Prescription (Examples)
Example 1 - Adult sinusitis
Rx
1. Amoxicillin + Clavulanate (500+125 mg) tab
1 tab BD x 7 days [Take after food]
2. Cetirizine 10 mg tab
1 tab OD at night x 5 days
3. Normal saline nasal drops / saline rinse
2 drops each nostril TID
Advice: Plenty of fluids. Return if not improved in 72 hours.
Example 2 - Child with otitis media (12 kg)
Rx
1. Amoxicillin 250 mg/5 mL syrup
7 mL twice daily x 10 days [With or without food]
2. Paracetamol 250 mg/5 mL syrup
5 mL every 6 hours if pain/fever
Advice: Finish full 10 days. Recheck at 2 weeks.
Example 3 - Cellulitis leg
Rx
1. Amoxicillin + Clavulanate (625 mg) tab
1 tab BD x 7 days [After food]
2. Ibuprofen 400 mg tab
1 tab TID with food x 5 days
3. Elevation of leg. Rest.
Advice: Mark the border of redness with pen to track spread.
Return immediately if redness crosses the mark or fever develops.
5 Mistakes Doctors Commonly Make
-
Prescribing amoxicillin for sinusitis - most sinusitis pathogens produce beta-lactamase, so plain amoxicillin often fails. Use amox-clavulanate.
-
Underdosing amoxicillin in children for otitis media - 25 mg/kg/day is too low. Use 80-90 mg/kg/day to cover resistant pneumococci.
-
Labeling ampicillin rash as penicillin allergy - the maculopapular rash from ampicillin/amoxicillin during viral illness is NOT IgE-mediated. Don't restrict the entire penicillin class based on this.
-
Prescribing cloxacillin/dicloxacillin after food - absorption drops significantly. Always tell patients to take it on an empty stomach.
-
Short courses for strep throat - 5 days is not enough. It needs 10 days to prevent rheumatic fever. Full 10-day course every time.
Quick Reference Card (Screenshot this)
AMOXICILLIN
Adult: 500 mg TID or 875 mg BD
Child: 40-90 mg/kg/day ÷ TID (high dose for ear/pneumonia)
With or without food ✓
AMOXICILLIN-CLAVULANATE (Augmentin 625 mg)
Adult: 1 tab BD
Child: 45 mg/kg/day ÷ BD
After food ✓ (reduces GI upset)
CLOXACILLIN / DICLOXACILLIN
Adult: 500 mg QID
EMPTY stomach (1 hr before food)
PEN V
Adult: 500 mg QID x 10 days
Empty stomach
ALLERGY = STOP + Azithromycin / Co-trimoxazole / Levofloxacin
This is a shared conversation. Sign in to Orris to start your own chat.