Lung volume fishman
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Searching Images
lung volumes subdivisions spirometry diagram TLC FRC RV
I have comprehensive content from Fishman's. Let me now compile the full answer.
Lung Volumes — Fishman's Pulmonary Diseases and Disorders
Definitions and Subdivisions
Lung volumes and capacities are the fundamental descriptors of respiratory function. The convention divides the total volume of gas in the lungs into volumes (non-overlapping compartments) and capacities (combinations of two or more volumes).
TABLE 31-1 Glossary for Static Lung Volumes and Capacities
Volumes (primary, non-overlapping):
| Term | Symbol | Definition |
|---|---|---|
| Tidal volume | TV (Vt) | Volume inspired or expired per breath during quiet breathing |
| Inspiratory reserve volume | IRV | Maximum additional volume inspired from end-tidal inspiration |
| Expiratory reserve volume | ERV | Maximum volume expired from the resting end-expiratory level |
| Residual volume | RV | Volume remaining after maximal expiration |
Capacities (sums of volumes):
| Term | Symbol | Definition |
|---|---|---|
| Inspiratory capacity | IC | IRV + TV; max volume inspired from end-expiratory level |
| Vital capacity | VC | Max volume expired from TLC (= TLC − RV) |
| Functional residual capacity | FRC | RV + ERV; volume in lungs at resting end-expiratory position |
| Total lung capacity | TLC | All volumes combined; volume at end of maximal inspiration |
| Closing capacity | CC | Closing volume + RV (CC/TLC, %) |
| RV/TLC ratio | RV/TLC% | Expressed as a percentage |
Determinants of Key Lung Volumes
Functional Residual Capacity (FRC)
FRC is the major reference point for all lung volume subdivisions. It is set by the balance of opposing recoil forces of the lungs (inward) and chest wall (outward) when the respiratory muscles are at rest. — Fishman's, Ch. 10
Total Lung Capacity (TLC)
TLC is determined by the balance between:
- The force-generating capacity of the inspiratory muscles, and
- The opposing elastic recoil of lungs + chest wall.
Weakness of inspiratory muscles or increased lung stiffness → ↓ TLC
Loss of lung retractive force (e.g., emphysema) → ↑ TLC — Fishman's, Ch. 10
Residual Volume (RV)
RV is set by the balance between:
- Expiratory muscle force + lung recoil (favoring volume decrease), and
- Outward recoil of chest wall (favoring expansion).
In middle-aged and older individuals, small airway closure at low lung volumes and air trapping becomes an important determinant of RV. — Fishman's, Ch. 10
Measurement Methods
Spirometry
Spirometers measure volumes directly but cannot measure RV, FRC, or TLC — these require indirect techniques. Spirometry provides: TV, IRV, ERV, VC, IC, FVC, FEV₁, PEF, FEF₂₅–₇₅, MVV.
Technique: the patient breathes quietly to establish the resting end-expiratory level (FRC), then inspires maximally → slow, complete expiration. Attempts to maximize flow in obstructive disease paradoxically reduce volumes due to dynamic airway compression.
Indirect Measurement of FRC (and thus RV, TLC)
RV is determined indirectly: (1) Measure FRC by one of three methods → (2) Measure ERV spirometrically → (3) RV = FRC − ERV.
1. Closed-Circuit Helium Dilution
- Based on the conservation of mass principle and insolubility of He in tissues.
- System loaded with ~10% helium; patient breathes quietly until equilibration.
- Formula: FRC = V_He × (C₁ − C₂) / C₂
- Limitation: underestimates lung volume in patients with trapped gas (bullae, severe obstruction) — communicating gas only.
2. Open-Circuit Nitrogen Washout
- Patient breathes 100% O₂; N₂ washed out of lungs and collected.
- Uses: initial alveolar N₂ concentration (~81% fasting) and measured expired N₂ volume.
- FRC = V_E × F_EN₂ / F_AN₂
- Also underestimates in poorly-communicating regions.
3. Body Plethysmography (Gold Standard)
- Based on Boyle's Law (P₁V₁ = P₂V₂).
- Patient sits in a sealed box; at end-expiration shutter closes; patient pants against closed shutter.
- Measures thoracic gas volume (TGV) = all intrathoracic gas, including trapped gas.
- Advantage over dilution techniques: measures non-communicating (trapped) gas — therefore typically gives higher values than gas dilution in obstructive disease.
- Three types of plethysmograph: pressure (most common), volume, and pressure-corrected flow. — Fishman's, Ch. 31
Changes with Age
Figure 18-8 — Lung volume changes with age (cross-sectional data):
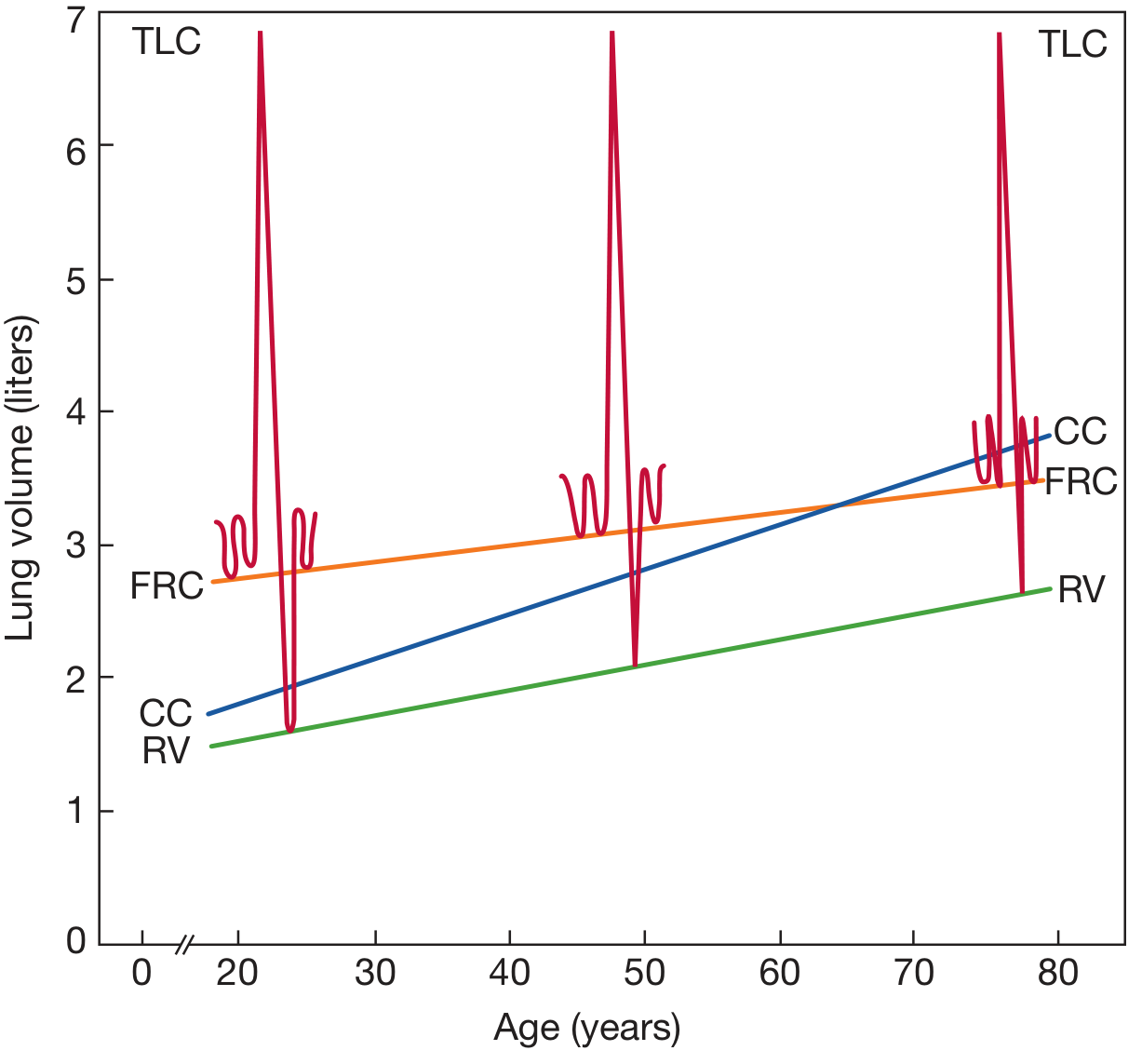
Key age-related patterns:
- TLC: little or no significant decline with age (cross-sectional data). Longitudinal studies suggest small but significant falls may exist (~25 mL/year in fit elderly men).
- RV: increases consistently with age (airway closure and air trapping).
- VC / FVC: declines with age — 21–33 mL/year in men, 18–29 mL/year in women (cross-sectional).
- FRC: rises with age (loss of lung elastic recoil, chest wall stiffening).
- Closing capacity (CC): rises with age and may exceed FRC, leading to airway closure during tidal breathing → V/Q mismatch.
— Fishman's, Ch. 18
Compliance and Elastic Recoil
Compliance (C) = ΔV_L / Δ(P_A − P_pl) — describes distensibility (ease of inflation). Its inverse is elastance (stiffness).
The pressure-volume (P-V) curve of the lung is nonlinear: compliance is greatest at low volumes (near RV) and least at high volumes (near TLC), where elastic elements approach their distensibility limits.
Hysteresis: the inflation and deflation P-V curves differ due to:
- Surface tension forces (surfactant)
- Sequential recruitment of closed lung units during inflation
- Stress adaptation of lung tissue
Static elastic recoil pressure ≈ 5 cmH₂O at FRC and ≈ 30 cmH₂O at TLC. — Fishman's, Ch. 10
Interpretation of Abnormal Lung Volumes
| Pattern | TLC | RV | FRC | RV/TLC |
|---|---|---|---|---|
| Restriction (e.g., IPF) | ↓ | ↓ | ↓ | Normal or ↑ |
| Obstruction (e.g., COPD) | Normal or ↑ | ↑ | ↑ | ↑ |
| Emphysema | ↑ | ↑↑ | ↑ | ↑↑ |
| Air trapping | Normal | ↑ | ↑ | ↑ |
Important: TLC <5th percentile = restriction; TLC >95th percentile = hyperinflation. RV/TLC or FRC/TLC >95th percentile indicates air trapping even when TLC is normal.
All static lung volumes expressed at BTPS (body temperature, ambient pressure, saturated with water vapour).
Sources: Fishman's Pulmonary Diseases and Disorders (9th ed.), Chapters 10 (Respiratory System Mechanics), 18 (Aging Lung), and 31 (Pulmonary Function Testing).
This is a shared conversation. Sign in to Orris to start your own chat.