Grades of clubbing
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching the Web
grades of clubbing fingers Schamroth sign classification
Searching Images
grades of finger clubbing Schamroth sign
Here is a comprehensive overview of the grades of clubbing:
Grades of Finger Clubbing
Two grading systems are in common use — a 4-grade system (most cited in clinical medicine) and a 5-grade system (used by some nursing/allied health texts).
4-Grade System (most widely used)
| Grade | Name | Features |
|---|---|---|
| Grade I | Mild / Soft tissue fluctuation | Obliteration of the Lovibond angle (normal <165°); positive fluctuation test (nail bed feels spongy); Schamroth's window is obliterated but clubbing is not obvious on inspection alone |
| Grade II | Moderate | Parrot-beak appearance of the nail fold; apparent convexity of the nail plate; visually noticeable on inspection |
| Grade III | Gross clubbing | Thickening of the entire distal finger giving a drumstick / Hippocratic finger appearance; marked increase in all curvature planes |
| Grade IV | Hypertrophic osteoarthropathy (HOA) | Grade III changes plus shiny nail and skin with longitudinal striations; associated subperiosteal new bone formation causing periarthritis and pain in long bones (radius, ulna, tibia, fibula); most common with bronchogenic carcinoma, mesothelioma, bronchiectasis, liver cirrhosis |
5-Grade System (alternative)
| Grade | Feature |
|---|---|
| 1 | Softening and fluctuation of the nail bed |
| 2 | Hyponychial (Lovibond) angle >160° |
| 3 | Accentuated convexity of the nail plate |
| 4 | Drumstick / clubbed appearance of the fingertip |
| 5 | Nail and periungual skin become shiny with longitudinal striations |
Key Clinical Signs & Tests
Lovibond's Sign (Profile Sign)
The angle between the nail plate and the proximal nail fold (hyponychial angle) normally measures <165°. In clubbing, this angle is ≥180° (obliterated or reversed). This is the most sensitive individual measurement.
Schamroth's Window Test
- Place the dorsal surfaces of the terminal phalanges of corresponding fingers (especially ring fingers) back-to-back.
- Normal: A small diamond-shaped window is visible at the bases of the nail beds.
- Positive (clubbing): The window is obliterated — the earliest detectable sign of clubbing.
- Sensitivity 77–87%, specificity 90%, positive LR ~8.
Fluctuation Test
Press the nail base — a soft, boggy, spongy feeling indicates increased vascularity and connective tissue proliferation.
Phalangeal Depth Ratio (PDR)
The ratio of the digital depth at the nail fold to digital depth at the distal interphalangeal joint. A PDR > 1.0 is the objective standard for clubbing. The digital index (sum of PDR for all 10 fingers) ≥10.2 is diagnostic.
Pathophysiology (brief)
Clubbing results from:
- Increased soft tissue in the distal phalanx — driven by hypoxia-induced upregulation of VEGF, PDGF, HIF-1α, HIF-2α, and increased microvessel density.
- Peripheral arteriovenous shunting — megakaryocytes and platelets bypass pulmonary/hepatic filtration and release growth factors directly in digital capillaries.
Clubbing can develop rapidly (~2 weeks, e.g., new empyema) and similarly reverse after treatment (e.g., corrective cardiac surgery). — Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases
Causes (by grade severity)
| Cause | Typical grade |
|---|---|
| Cyanotic congenital heart disease | III–IV |
| Bronchogenic carcinoma | III–IV (with HOA) |
| Cystic fibrosis, bronchiectasis | II–IV |
| Pulmonary fibrosis, lung abscess | II–III |
| IBD, liver cirrhosis | II–III |
| Infective endocarditis | I–II |
| Idiopathic / familial | I–II |

Positive Schamroth sign: the normal diamond-shaped window between opposed terminal phalanges is absent, indicating clubbing.
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Dermatology 2-Volume Set 5e; Harrison's Principles of Internal Medicine 22E
Dyspnea gradings
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the key data. Here is the comprehensive answer:
Dyspnea Grading Scales
Multiple validated grading systems exist for dyspnea, each serving a different clinical context.
1. Modified Medical Research Council (mMRC) Dyspnea Scale
The most widely used scale in respiratory medicine (COPD, ILD, etc.). Grades 0–4 based on activity that provokes breathlessness.
| Grade | Description |
|---|---|
| 0 | Not troubled by breathlessness except with strenuous exercise |
| 1 | Troubled by shortness of breath when hurrying on level ground or walking up a slight hill |
| 2 | Walks slower than people of the same age on the level because of breathlessness, OR has to stop for breath when walking at own pace on the level |
| 3 | Stops for breath after walking about 100 yards (~91 m) or after a few minutes on level ground |
| 4 | Too breathless to leave the house, or breathless when dressing or undressing |
Clinical use: mMRC ≥2 indicates significant symptom burden in COPD (GOLD criteria). It is also a component of the BODE index (mMRC 0–1 = 0 points; 2 = 1 point; 3 = 2 points; 4 = 3 points). — Fishman's Pulmonary Diseases and Disorders; Harrison's 22E
2. New York Heart Association (NYHA) Functional Classification
Used primarily in heart failure and cardiac disease to grade exertional dyspnea.
| Class | Limitation | Description |
|---|---|---|
| I | None | Ordinary physical activity does not cause fatigue, dyspnea, palpitations, or angina |
| II | Mild | Comfortable at rest. Ordinary activity (e.g., carrying heavy packages) causes symptoms |
| III | Moderate | Comfortable at rest. Less than ordinary activity (e.g., getting dressed) causes symptoms |
| IV | Severe | Symptoms present at rest; any activity worsens symptoms |
Note: NYHA class does not correlate well with objective measures such as LV ejection fraction or peak VO₂ consumption. — Harrison's Principles of Internal Medicine 22E
3. Modified Borg Scale
Used to rate dyspnea intensity at a single point in time, especially during exercise testing (6-minute walk test, cardiopulmonary exercise testing).
| Score | Verbal Descriptor |
|---|---|
| 0 | Nothing at all |
| 0.5 | Very, very slight (just noticeable) |
| 1 | Very slight |
| 2 | Slight |
| 3 | Moderate |
| 4 | Somewhat severe |
| 5 | Severe |
| 6 | |
| 7 | Very severe |
| 8 | |
| 9 | Very, very severe (almost maximal) |
| 10 | Maximal |
Numerical rating scales (0–10) and visual analog scales (10 cm line) are equivalent in reliability. The Borg scale is a variant with verbal anchors at key points. All have been validated against each other. — Murray & Nadel's Textbook of Respiratory Medicine
4. American Thoracic Society (ATS) 5-Point Dyspnea Scale
An earlier scale based on the original MRC questionnaire, rating self-reported exercise tolerance.
| Grade | Description |
|---|---|
| 0 | No dyspnea except with strenuous exercise |
| 1 | Dyspnea when hurrying or walking up a slight hill |
| 2 | Walks slower than contemporaries on the level, or stops after ~15 min walking |
| 3 | Stops after ~100 yards on the level, or after a few minutes |
| 4 | Dyspnea at rest (too breathless to leave the house) |
5. Baseline Dyspnea Index (BDI) / Transition Dyspnea Index (TDI)
A rater-administered multidimensional scale that assesses:
- Magnitude of task that elicits dyspnea (e.g., hills vs. level ground)
- Impact on activities of daily living
- Effort required to produce dyspnea
The TDI measures change from baseline — used in clinical trials to assess treatment response in COPD.
Summary Comparison
| Scale | Range | Domain | Primary Use |
|---|---|---|---|
| mMRC | 0–4 | Activity level triggering dyspnea | COPD, ILD, respiratory medicine |
| NYHA | I–IV | Functional limitation from dyspnea | Heart failure, cardiology |
| Borg | 0–10 | Instantaneous dyspnea intensity | Exercise testing, rehabilitation |
| BDI/TDI | 0–12 / –9 to +9 | Multidimensional baseline + change | COPD clinical trials |
| BODE Index | 0–10 | Prognostic composite (B+O+D+E) | COPD mortality prediction |
Sources: Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine 22E; Lippincott Illustrated Reviews: Pharmacology
6 minutes walk test
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
6 minute walk test protocol normal values ATS guidelines clinical use
Reading File
Reading File
Here is a comprehensive overview of the 6-Minute Walk Test (6MWT):
6-Minute Walk Test (6MWT)
Definition
The 6MWT is a self-paced, submaximal field exercise test in which the patient walks as far as possible on a flat, hard surface in 6 minutes. The primary outcome is the 6-Minute Walk Distance (6MWD) in metres. It was first introduced in the early 1960s as a timed walking test and standardised by the ATS in 2002.
Protocol (ATS Guidelines)
| Parameter | Specification |
|---|---|
| Course | Flat, hard corridor, 30 m long (cones at each end); marked every 3 m |
| Patient preparation | Rest in chair for ≥10 min before test; no warm-up |
| Footwear | Comfortable walking shoes |
| Medications | Usual medications taken as normal |
| Supplemental O₂ | Carry if usually prescribed; document flow rate |
| Instructions | "Walk as far as possible in 6 min; you may slow down or stop if needed" |
| Encouragement | Standardised verbal cues given every minute (e.g., "You're doing well, 3 minutes left") |
| Monitoring | SpO₂, heart rate, dyspnea (Borg scale) — before and after |
| Repetition | Two tests if needed; best result used; tests separated by ≥30 min |
| Timing | Same time of day for serial tests |
Contraindications
| Type | Condition |
|---|---|
| Absolute | Unstable angina within past month; MI within past month |
| Relative | Resting HR >120 bpm; SBP >180 mmHg; DBP >100 mmHg |
Stop the test if: chest pain, intolerable dyspnea, leg cramps, staggering, diaphoresis, pallor, SpO₂ <85%.
Normal Values
| Group | Reference 6MWD |
|---|---|
| Healthy adults (40–80 yrs) | 400–700 m |
| Median men | ~576 m |
| Median women | ~494 m |
| Lower limit of normal (men) | predicted − 153 m |
| Lower limit of normal (women) | predicted − 139 m |
Reference equations (Enright et al., 1998) for healthy adults 40–80 yrs:
- Men: 6MWD = (7.57 × height cm) − (5.02 × age) − (1.76 × weight kg) − 309
- Women: 6MWD = (2.11 × height cm) − (2.29 × weight kg) − (5.78 × age) + 667
Minimal Clinically Important Difference (MCID)
| Condition | MCID |
|---|---|
| COPD, heart failure, ILD, PAH | ~30 m (ATS/ERS standard) |
| Range across studies | 14–30.5 m |
A change of ≥30 m is considered clinically meaningful in most cardiopulmonary conditions.
Clinical Indications
- Measuring response to interventions — pulmonary rehabilitation, pharmacotherapy (PAH, heart failure), lung transplant, LVRS
- Functional status assessment — COPD, cystic fibrosis, heart failure, IPF, peripheral vascular disease
- Pre-transplant evaluation — eligibility and timing for lung transplantation
- Prognosis prediction — component of the BODE index in COPD; correlates with mortality in COPD, IPF, PAH, heart failure
- Titrating supplemental oxygen — assess exertional hypoxemia and oxygen flow requirements
- Preoperative risk assessment — predictor of postoperative outcomes
BODE Index (uses 6MWD)
The 6MWD is a key component of the BODE prognostic index in COPD:
| 6MWD (metres) | BODE Points |
|---|---|
| ≥350 m | 0 |
| 250–349 m | 1 |
| 150–249 m | 2 |
| ≤149 m | 3 |
A BODE score >7 → ~30% 2-year mortality; score 5–6 → ~15%; score <5 → <10%. — Fishman's Pulmonary Diseases and Disorders
Comparison with Other Exercise Tests
| Test | Equipment | Information | Best use |
|---|---|---|---|
| 6MWT | None (corridor) | Submaximal functional capacity, SpO₂, 6MWD | Routine clinic, serial monitoring |
| Incremental Shuttle Walk Test (ISWT) | Audio cassette/speaker | Externally paced; correlates with VO₂ max | Pulmonary rehab assessment |
| CPET (Cardiopulmonary Exercise Test) | Treadmill/cycle ergometer, metabolic cart | VO₂ max, anaerobic threshold, VCO₂, full physiology | Unexplained dyspnea, pre-surgical evaluation, research |
Key Advantages & Limitations
Advantages
- Simple, cheap, no specialised equipment
- Reflects daily activity functional capacity better than maximal tests
- Well validated; widely used in RCTs
- Correlates with QoL measures; changes in 6MWD correlate with improvements in dyspnea
Limitations
- Submaximal — most patients do not reach maximal exercise capacity
- Cannot identify the specific physiologic cause of exercise limitation (unlike CPET)
- Practice/learning effect — 2nd test is typically ~25 m longer than 1st
- Results sensitive to corridor length, encouragement style, and patient motivation
- No universally accepted reference standards across all age groups
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Miller's Anesthesia 10e; ATS Statement (2002); NCBI StatPearls
Pneumothorax
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching Images
pneumothorax chest X-ray tension pneumothorax types
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a comprehensive overview of Pneumothorax:
Pneumothorax
Definition: Accumulation of air within the pleural cavity (between visceral and parietal pleura), causing partial or complete lung collapse.
Classification
1. Spontaneous Pneumothorax
Primary Spontaneous Pneumothorax (PSP)
- Occurs without underlying lung disease
- Caused by rupture of apical pleural blebs (small cystic spaces within or immediately under the visceral pleura)
- Typical patient: tall, thin, young males (15–35 yrs); smokers
- ~50% recurrence after first episode
- CT findings of multiple blebs/bullae → higher recurrence risk
Secondary Spontaneous Pneumothorax (SSP)
- Occurs in the presence of underlying lung disease
- More life-threatening due to reduced pulmonary reserve
- Causes:
- COPD (most common — bleb/bulla rupture)
- Cystic fibrosis
- Asthma
- AIDS/Pneumocystis jirovecii pneumonia
- Metastatic cancer (especially sarcoma)
- TB, lung abscess
- Catamenial pneumothorax — in women, within 72 hours of menses onset (related to endometriosis)
2. Traumatic Pneumothorax
- From penetrating (stab, gunshot) or blunt chest trauma
- Present in 40% of blunt thoracic trauma and 20% of penetrating injuries
- Includes iatrogenic causes:
- Transthoracic needle aspiration
- Thoracentesis
- Central venous catheter insertion (subclavian/internal jugular)
- Mechanical ventilation (barotrauma/volutrauma)
- Positive pressure ventilation (alveolar overdistention → rupture)
3. Tension Pneumothorax
- Air enters the pleural space via a one-way valve mechanism — cannot escape
- Progressive air trapping → rising intrapleural pressure
- Causes:
- Contralateral mediastinal shift
- Compression/kinking of SVC and IVC → ↓ venous return → ↓ cardiac output
- Obstructive shock
- Most common in: mechanically ventilated patients; also traumatic and resuscitation settings
Clinical Features of Tension Pneumothorax
| Sign | Detail |
|---|---|
| Tracheal deviation | Away from affected side |
| Absent/diminished breath sounds | Affected side |
| Hyperresonance on percussion | Affected side |
| Jugular venous distension | ↑ IVC pressure |
| Hypotension + tachycardia | Obstructive shock |
| ↑ Peak airway pressure | In ventilated patients |
| Hypoxemia | Near-universal in ventilated patients; 50% in spontaneous breathers |
4. Open Pneumothorax (Sucking Chest Wound)
- Chest wall defect allows air entry through the wound with breathing
- If wound size ≈ trachea size → air preferentially enters wound rather than airway → impairs ventilation
- Management: 3-sided occlusive dressing (Heimlich flutter valve) → allows air egress but not entry → followed by operative repair
Diagnosis
Chest X-Ray
- Hyperlucent area with absent bronchovascular markings peripheral to a visible visceral pleural line
- Lung collapse toward hilum
- Tension: mediastinal shift to contralateral side + hemidiaphragm depression
CT Chest
- Most sensitive; detects occult pneumothoraces
- Quantifies size; identifies blebs/bullae; guides management decisions
Ultrasound (POCUS)
| Finding | Significance |
|---|---|
| Absent pleural sliding | Suggests pneumothorax (also in apnea, adhesions) |
| "Barcode/stratosphere" sign on M-mode | Absent sliding (cf. "seashore sign" = normal) |
| B-lines present | Excludes pneumothorax at that location |
| Lung point | Highly specific for pneumothorax — marks the edge |
"A lung point represents the edge of the pneumothorax where the lung has fallen away from the parietal pleura" — Murray & Nadel's
Size Assessment
| Classification | Chest X-Ray |
|---|---|
| Small | <2 cm rim between lung and chest wall (BTS); some guidelines use <3 cm apex |
| Large/Moderate | ≥2 cm (BTS) or ≥3 cm |
Management
Tension Pneumothorax — Medical Emergency
Treat clinically before imaging
- Immediate needle decompression (temporising):
- 14–16G cannula (adults), 18G (children); ≥3–5 cm length
- 2nd intercostal space, midclavicular line (traditional)
- OR 4th/5th ICS, midaxillary line (preferred by ATLS — less chest wall thickness, avoids internal mammary vessels)
- Confirmed by air escaping under pressure or rapid haemodynamic improvement
- Definitive: Tube thoracostomy (chest drain)
Primary Spontaneous Pneumothorax
| Scenario | Management |
|---|---|
| Asymptomatic, small | Conservative observation (outpatient if good support) |
| Symptomatic or moderate/large | Needle aspiration (first line) or tube drainage |
| Recurrent or failed aspiration | VATS + bleb stapling + pleurodesis (~100% successful) |
Secondary Spontaneous Pneumothorax
| Size | Management |
|---|---|
| Small (<1 cm) | Admission + O₂ + 24h observation |
| Moderate (1–2 cm) | Trial of simple needle aspiration |
| Large (>2 cm) or failed aspiration | Tube thoracostomy (small bore 8–14F pigtail catheter) |
| Respiratory distress / tension / hemopneumothorax | Moderate tube (14–28F); large bore (>28F) for hemothorax |
Traumatic Pneumothorax
- Most treated with tube drainage unless very small
- Hemopneumothorax: two chest tubes — one superior (air), one inferior (blood)
- Iatrogenic: supplemental O₂ or aspiration first; tube if fails
Chest Tube Management
- Attached to water seal device
- Routine suction not recommended (does not improve outcomes)
- Suction (−20 cm H₂O) reserved for lung failure to re-expand after 24–48h
- Remove when lung fully re-expanded and air leak ceased
- Clamp test ×4 hours before removal
Recurrence Prevention
- VATS with bleb resection + mechanical/talc pleurodesis: nearly 100% effective
- Chemical pleurodesis alone: if not surgical candidate
- Indications for surgery (first episode PSP): occupational hazard (pilots, divers), remote travel, CT showing multiple blebs
Complications
- Tension pneumothorax → obstructive shock → death if untreated
- Re-expansion pulmonary oedema (rare — after large pneumothorax evacuation)
- Re-expansion hypotension (rare)
- Chest tube complications: malposition, pleural infection, pain
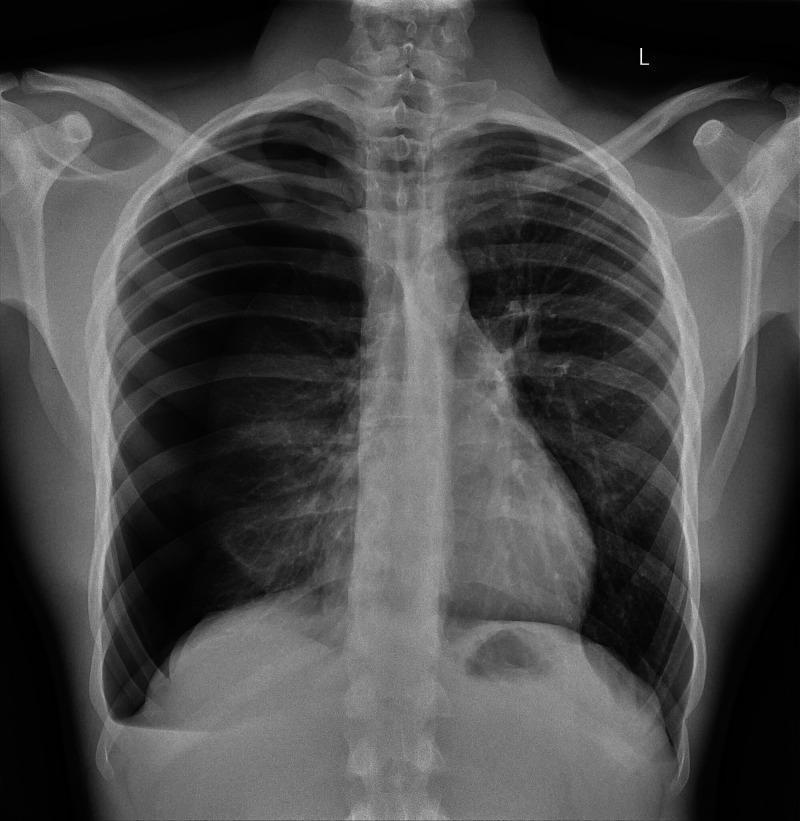
CXR: Large right-sided tension pneumothorax — right lung fully collapsed, mediastinum and trachea shifted to the left, right hemidiaphragm depressed.
Sources: Harrison's Principles of Internal Medicine 22E; Murray & Nadel's Textbook of Respiratory Medicine; Rosen's Emergency Medicine; Schwartz's Principles of Surgery 11e; Roberts and Hedges' Clinical Procedures in Emergency; Murray & Nadel's (POCUS chapter)
Metabolic equivalent
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a comprehensive overview of the Metabolic Equivalent of Task (MET):
Metabolic Equivalent of Task (MET)
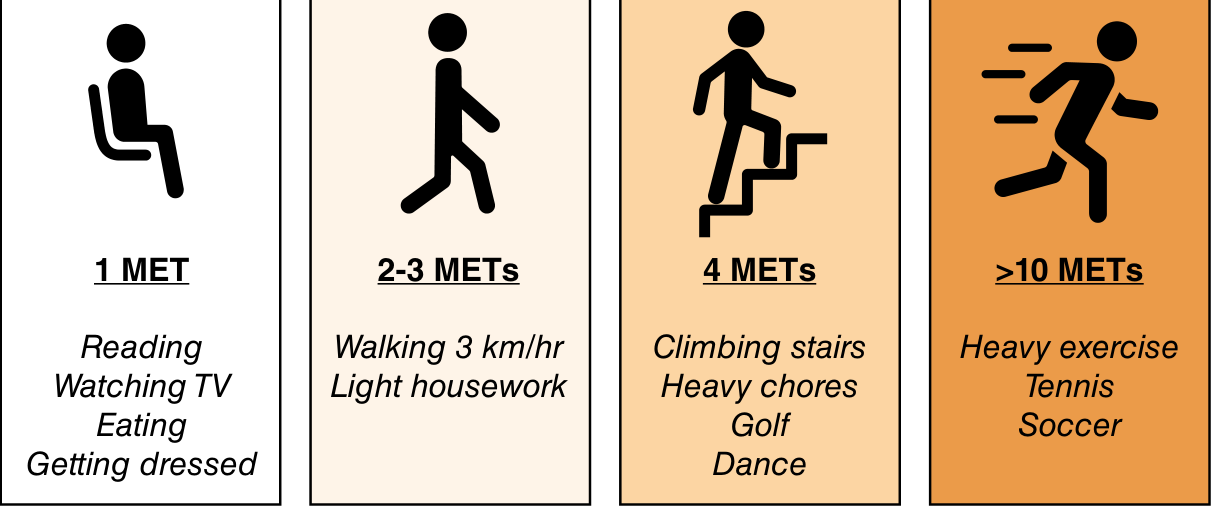
Definition
One MET = the resting metabolic rate in a sitting position = oxygen consumption of 3.5 mL O₂/kg/min (approximately 1 kcal/kg/hour).
Any activity's MET value represents how many times more oxygen is consumed compared to rest. For example, an activity of 4 METs consumes 4× the resting oxygen = 14 mL O₂/kg/min.
Metabolic Equivalents of Task (METs) — Sabiston Textbook of Surgery
MET Scale: Activities by Level
| METs | Activity |
|---|---|
| 1 | Eating, watching TV, reading, working at computer, dressing/getting dressed |
| 2 | Walking down stairs, cooking, light housework, walking 3 km/hr |
| 3 | Walking 1–2 blocks on level ground |
| 4 | Raking leaves, gardening, climbing 1 flight of stairs, golf, dancing |
| 5 | Climbing 1 flight of stairs, bicycling, dancing |
| 6 | Playing golf (carrying clubs) |
| 7 | Playing singles tennis |
| 8 | Rapidly climbing stairs, slow jogging |
| 9 | Jumping rope slowly, moderate cycling |
| 10 | Swimming quickly, jogging briskly |
| ≥10 | Cross-country skiing, full-court basketball, football, heavy exercise |
| 12 | Running rapidly for moderate-to-long distances |
Clinical Classification of Functional Capacity
| Category | MET Range | Clinical Meaning |
|---|---|---|
| Poor | < 4 METs | Cannot climb 1 flight of stairs or walk on level ground at 4 mph; high perioperative risk |
| Moderate | 4–7 METs | Can climb stairs, do light housework, play golf |
| Good / Excellent | ≥ 7–10 METs | Active lifestyle, sports activity |
| Very Good | > 10 METs | Strenuous exercise, competitive sports |
The critical clinical threshold is 4 METs. — ACC/AHA 2014 Guidelines
Clinical Significance — Perioperative Risk Assessment
The MET is the foundation of preoperative functional capacity assessment, directly tied to perioperative cardiac risk:
ACC/AHA Guideline Recommendation
- ≥4 METs functional capacity → patient may proceed directly to surgery (low perioperative cardiac risk)
- <4 METs OR uncertain functional capacity → consider exercise/pharmacologic cardiac stress testing if results would alter management
Why 4 METs?
- Based on exercise testing studies linking poor functional capacity with elevated major adverse cardiac events (MACE) perioperatively
- ≥4 METs ≈ ability to climb 1 flight of stairs or do light gardening — activities of moderate exertion
Practical Bedside Markers for ≥4 METs
| Marker | Significance |
|---|---|
| Self-reported ability to climb ≥3 flights of stairs | Identifies ≥4 MET capacity |
| DASI score ≥32 | Correlates with ≥4 METs |
| ≥6 METs on MET-REPAIR questionnaire | Identifies ≥4 MET capacity |
| Inability to climb 2 flights of stairs | Increased perioperative cardiac risk |
Assessment Tools
1. Duke Activity Status Index (DASI)
A 12-item self-administered questionnaire that estimates functional capacity (VO₂ peak) from daily activities:
Formula: VO₂ peak (mL/kg/min) = (0.43 × DASI score) + 9.6
MET estimate: METs = VO₂ peak × 0.286
MET estimate: METs = VO₂ peak × 0.286
| DASI Score | Clinical significance |
|---|---|
| ≥32 | ~≥4 METs — adequate functional capacity |
| <32 | Reduced functional capacity, increased surgical risk |
| <25 | Clinically meaningful increase in perioperative risk |
DASI activities (representative items):
- Take care of yourself (eating, dressing, bathing) — 2.75 pts
- Walk 200 yards on level ground — 2.75 pts
- Climb a flight of stairs or walk up a hill — 5.50 pts
- Run a short distance — 8.00 pts
- Do heavy housework (moving furniture) — 8.00 pts
- Play golf / doubles tennis / dance — 6.00 pts
- Strenuous sports (singles tennis, basketball, skiing) — 7.50 pts
2. MET-REPAIR Questionnaire
A structured questionnaire used as an alternative to unstructured interviews; ≥6 METs on MET-REPAIR identifies patients with adequate capacity.
3. Objective Testing
When questionnaires are inconclusive:
- 6-Minute Walk Test — poor performance → increased major postoperative complications
- Incremental Shuttle Walk Test
- CPET (gold standard) — directly measures VO₂ max, anaerobic threshold
Important: Resting LVEF is NOT a proxy for functional capacity — exercise capacity can vary considerably among patients with similar resting EF. — Miller's Anesthesia 10e
MET in Other Contexts
| Context | Use |
|---|---|
| BODE index (COPD) | Component: mMRC dyspnea + 6MWD reflect functional capacity |
| Cardiac rehabilitation | Exercise prescription based on target MET intensity |
| Pulmonary rehabilitation | Target training intensity ≈ 60–80% of peak MET achieved on testing |
| Physical activity guidelines | Moderate intensity = 3–6 METs; vigorous = >6 METs (WHO) |
| Occupational medicine | Work clearance based on MET demands of job vs. patient's capacity |
Key Formula
1 MET = 3.5 mL O₂/kg/min ≈ 1 kcal/kg/hour
MET × 3.5 mL/kg/min = oxygen consumption at that activity level
Sources: Sabiston Textbook of Surgery; Miller's Anesthesia 10e; Morgan & Mikhail's Clinical Anesthesiology 7e; Campbell-Walsh-Wein Urology (DASI formula)
This is a shared conversation. Sign in to Orris to start your own chat.