
image.png
This i have to check for living anatomy. Describe each
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have sufficient material from the library plus my own anatomical knowledge to give a comprehensive answer for all 21 topics. Let me compile the full response.
Here is a detailed description of each topic on your living anatomy flashcards:
1. THENAR EMINENCE
The thenar eminence is the prominent fleshy mound on the lateral (radial) side of the palm at the base of the thumb. It is formed by three intrinsic thumb muscles:
- Abductor pollicis brevis - abducts the thumb
- Flexor pollicis brevis - flexes the proximal phalanx of the thumb
- Opponens pollicis - the deepest; rotates the 1st metacarpal, producing opposition
All three are innervated by the recurrent branch of the median nerve (C8, T1). In living anatomy, you assess it by looking at bulk (wasting = median nerve lesion) and testing opposition (thumb tip to little finger tip).
2. LIGAMENTUM PATELLAE
The ligamentum patellae (patellar ligament) is the strong, flat band that runs from the apex of the patella to the tibial tuberosity. It is the continuation of the quadriceps tendon below the patella. It transmits the force of the quadriceps femoris to the tibia, producing knee extension. In living anatomy, it is easily palpated just below the patella with the knee slightly flexed, and the patellar tendon reflex tests it (L2-L4).
3. MOVEMENTS OF THUMB
The thumb (pollex) has a saddle (carpometacarpal) joint that allows 5 movements:
- Flexion - across the palm (FPB, FPL)
- Extension - away from the palm (EPL, EPB)
- Abduction - anteriorly away from the plane of the palm (APB)
- Adduction - returning towards the index finger (adductor pollicis - ulnar nerve)
- Opposition - combined movement rotating the thumb to face the little finger (median nerve via opponens pollicis)
The key nerve division: median nerve governs opposition/abduction/flexion; ulnar nerve governs adduction.
4. PALPATE CAROTID ARTERY
The common carotid artery is palpated at the anterior border of sternocleidomastoid (SCM), at the level of the thyroid cartilage (C4 vertebral level), where it bifurcates into internal and external carotid arteries. In living anatomy:
- Gently press medial to SCM, lateral to larynx
- Feel the pulsation against the carotid tubercle of C6 (Chassaignac's tubercle)
- Never compress both sides simultaneously - risk of syncope from carotid sinus pressure (CN IX - Hering's nerve)
5. ANT. TIBIAL ARTERY
The anterior tibial artery is a branch of the popliteal artery. It passes forward through the interosseous membrane to enter the anterior compartment of the leg. It runs between tibialis anterior and extensor digitorum longus, descending to the ankle where it becomes the dorsalis pedis artery. In living anatomy, it is palpated on the dorsum of the foot between the tendons of extensor hallucis longus and extensor digitorum longus, lateral to the EHL tendon, at the level of the ankle.
6. MOVEMENT OF ATLANTOAXIAL AND ATLANTO-OCCIPITAL JOINTS
- Atlanto-occipital joint (C0-C1): Between the occipital condyles and superior facets of atlas. Primary movement is nodding (flexion/extension) - "yes" movement. About 15° each way.
- Atlantoaxial joint (C1-C2): Between the atlas and the odontoid process (dens) of the axis. Primary movement is rotation - "no" movement. About 45° each way, accounting for ~50% of all cervical rotation.
In living anatomy: test nodding (atlanto-occipital) and rotation (atlantoaxial) with the rest of the cervical spine stabilised.
7. HYPOTHENAR EMINENCE
The hypothenar eminence is the fleshy mound on the medial (ulnar) side of the palm at the base of the little finger. It contains three muscles:
- Abductor digiti minimi - abducts little finger
- Flexor digiti minimi brevis - flexes little finger
- Opponens digiti minimi - opposes little finger towards thumb
All are innervated by the deep branch of the ulnar nerve (C8, T1). Wasting of the hypothenar eminence indicates an ulnar nerve lesion.
8. POST. TIBIAL ARTERY
The posterior tibial artery is the larger terminal branch of the popliteal artery. It runs in the posterior (deep) compartment of the leg with the tibial nerve. In living anatomy, it is palpated posterior to the medial malleolus, between the medial malleolus and the calcaneus (heel bone). It is a key peripheral pulse assessed in vascular examinations; absence suggests peripheral arterial disease in the lower limb.
9. SUPERFICIAL TEMPORAL ARTERY
A terminal branch of the external carotid artery, it emerges from the parotid gland and crosses the zygomatic arch anterior to the ear. In living anatomy, it is palpated just anterior to the tragus of the ear (pre-auricular area), where its pulse is readily felt. It branches into frontal and parietal branches. It is clinically important in temporal arteritis (giant cell arteritis), where it becomes thickened, nodular, and tender.
10. EXTRAOCULAR MUSCLES
Six muscles move each eyeball, tested by asking the patient to follow your finger in an "H" pattern:
| Muscle | Nerve | Primary Action |
|---|---|---|
| Superior rectus | CN III | Elevation |
| Inferior rectus | CN III | Depression |
| Medial rectus | CN III | Adduction |
| Inferior oblique | CN III | Elevation in adduction |
| Superior oblique | CN IV | Depression in adduction |
| Lateral rectus | CN VI | Abduction |
Memory: LR6 SO4 rest CN3. In living anatomy, test each of the 6 cardinal positions of gaze and look for diplopia or restriction.
11. TESTING MUSCLES OF FACIAL EXPRESSION
All muscles of facial expression are innervated by CN VII (facial nerve). Key muscles and their tests:
- Frontalis - "raise your eyebrows" (spared in UMN lesions)
- Orbicularis oculi - "close your eyes tight" / Bell's phenomenon
- Buccinator - "puff out your cheeks"
- Orbicularis oris - "whistle/show teeth"
- Platysma - "clench your teeth and pull your lips down"
Distinguish UMN (central) vs LMN (peripheral) facial palsy: UMN spares the upper face (forehead) because of bilateral cortical representation.
12. McBURNEY'S POINT
McBurney's point is located one-third of the way from the right anterior superior iliac spine (ASIS) to the umbilicus. It classically represents the surface marking of the base of the appendix where it joins the caecum. In appendicitis, there is:
- Direct tenderness at McBurney's point
- Rebound tenderness (Blumberg's sign)
- Rovsing's sign - pain at McBurney's point when the left iliac fossa is pressed
Note: The appendix tip is highly variable in position, so tenderness location can vary.
13. INFERIOR ANGLE OF SCAPULA
The inferior angle of the scapula lies at the level of the 7th intercostal space / 8th rib and the T7 spinous process. It is the lowest and most prominent part of the scapula. In living anatomy:
- Surface marking for the base of lung (lower lobe) at this level
- Used to count ribs from behind
- It moves laterally and rotates upward when the arm is raised above 90° (scapulohumeral rhythm)
- Winging of the inferior angle indicates serratus anterior paralysis (long thoracic nerve, C5-C7)
14. SERRATUS ANTERIOR
Origin: lateral surfaces of ribs 1-9 (as digitations)
Insertion: costal surface of the medial border of the scapula (mainly inferior angle)
Nerve: long thoracic nerve (nerve of Bell) - C5, C6, C7
Actions:
- Protracts (pulls forward) and rotates the scapula upward - essential for raising arm above 90°
- Holds the scapula flat against the thoracic wall
Testing: Push against a wall with outstretched arms. Paralysis causes "winged scapula" where the medial border lifts off the chest wall. This is the primary visual demonstration in living anatomy.
15. ADDUCTION & ABDUCTION OF FINGERS
- Abduction of fingers = spreading fingers apart, away from the middle finger axis (3rd digit). Performed by dorsal interossei (4 muscles) + abductor digiti minimi. Innervated by the deep ulnar nerve (C8, T1).
- Adduction of fingers = bringing fingers together, towards the middle finger axis. Performed by palmar interossei (3 muscles). Also deep ulnar nerve.
Testing in living anatomy: "spread your fingers apart" (abduction) and "grip a piece of paper between your fingers" (adduction). Froment's sign tests adductor pollicis (ulnar nerve).
16. LATISSIMUS DORSI
Origin: thoracolumbar fascia, spines of T7-L5, iliac crest, lower 3-4 ribs, inferior angle of scapula
Insertion: floor of the intertubercular (bicipital) groove of the humerus
Nerve: thoracodorsal nerve (C6, C7, C8)
Actions: Extension, adduction, and medial rotation of the arm at the shoulder. It is the "climbing muscle" and the "swimmer's muscle."
In living anatomy, it is seen as the posterior axillary fold. Test by asking the patient to adduct the arm against resistance ("cough" test - palpate it during coughing).
17. PAROTID DUCT (Stensen's Duct)
The parotid duct runs horizontally from the parotid gland, crosses the masseter muscle (where it can be palpated), then turns sharply inward (at ~90°) at the anterior border of masseter, piercing the buccinator to open into the mouth opposite the upper 2nd molar tooth.
Surface marking: middle third of a line drawn from the tragus of the ear to the midpoint of the philtrum (upper lip). In living anatomy, roll a finger across the masseter muscle to feel the cord-like duct. Its opening is visible intraorally as a small papilla.
18. PALPATE FACIAL ARTERY
The facial artery is a branch of the external carotid artery. It enters the face by hooking over the lower border of the mandible at the anterior border of the masseter muscle - this is where it is palpated in living anatomy. From here it runs a tortuous course towards the medial canthus of the eye. It is the same as the angular artery near the eye. The pulse is best felt by pressing gently against the mandible at the point where masseter meets the lower jaw.
19. GASTROCNEMIUS
The most superficial muscle of the posterior (superficial) compartment of the leg, forming the bulk of the calf.
- Origin: Two heads from the medial and lateral femoral condyles (posterior aspect)
- Insertion: Via the calcaneal (Achilles) tendon into the posterior calcaneus
- Nerve: Tibial nerve (S1, S2)
- Actions: Plantarflexion of the foot; flexion of the knee (since it crosses both joints)
In living anatomy: it is the main muscle visible when standing on tiptoe. Test: repeated single-leg heel raises. Absent ankle jerk (S1) with wasting points to S1 radiculopathy.
20. PECTORALIS MAJOR
A large fan-shaped muscle forming the anterior axillary fold.
- Origin: Clavicular head (medial clavicle), sternocostal head (sternum + costal cartilages 1-6), abdominal part
- Insertion: Lateral lip of the bicipital groove of humerus
- Nerve: Medial and lateral pectoral nerves (C5-T1)
- Actions: Adduction, medial rotation, and flexion of the arm; clavicular head also flexes the shoulder
In living anatomy: Ask the patient to press their hands on their hips (medial rotation against resistance) or press palms together in front - the anterior axillary fold contracts visibly and is palpable.
21. MUSCLES OF MASTICATION
All four are innervated by the mandibular nerve (V3), the motor branch of the trigeminal nerve (CN V):
| Muscle | Location | Action |
|---|---|---|
| Masseter | Over the ramus of mandible | Elevation (closes jaw) |
| Temporalis | Temporal fossa, fan-shaped | Elevation + retraction |
| Medial pterygoid | Medial ramus | Elevation + protrusion |
| Lateral pterygoid | Infratemporal fossa | Depression + protrusion + lateral movements |
Testing in living anatomy: Ask to clench teeth (palpate masseter and temporalis contracting), open mouth against resistance (lateral pterygoid), protrude and move jaw side to side. Unilateral V3 lesion causes the jaw to deviate towards the side of the lesion on opening.
Quick reference - nerves tested across these cards:
- Median nerve - thenar eminence, opposition of thumb
- Ulnar nerve - hypothenar eminence, finger abduction/adduction
- Long thoracic nerve - serratus anterior (winging)
- Facial nerve (VII) - muscles of expression
- Trigeminal (V3) - muscles of mastication
- Tibial nerve - gastrocnemius, post. tibial artery territory
- Thoracodorsal nerve - latissimus dorsi
Somites
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Excellent - all the core content is in hand. Here is a comprehensive account of somites:
SOMITES
Definition & Origin
Somites are paired, segmental blocks of paraxial mesoderm that form on either side of the developing neural tube and notochord. The word comes from the Greek soma (body). They are the fundamental unit of body segmentation in the embryo.
Origin: Formed by condensation of paraxial mesoderm - the thick longitudinal columns of mesoderm that flank the notochord, derived from the primitive node during gastrulation.
When Do Somites Form?
-
First pair appears around day 20 in the future occipital region, just caudal to the otic placode
-
They form in a strict craniocaudal (head-to-tail) sequence - one new pair every ~6 hours
-
Between days 26-32: 38-39 pairs form (the "somite period" of development)
-
By end of week 5: 42-44 pairs total
-
Because somites are so prominent and countable during weeks 4-5, they are used as one of the key criteria for staging embryo age
-
- Langman's Medical Embryology, p. 114
Total Number and Regional Distribution
The full complement is:
| Region | Number of Pairs |
|---|---|
| Occipital | 4 (5 formed, but 1st regresses) |
| Cervical | 8 |
| Thoracic | 12 |
| Lumbar | 5 |
| Sacral | 5 |
| Coccygeal | 8-10 (most regress) |
| Total | ~42-44 pairs |
The first occipital somites and most coccygeal somites regress during further development, so the final adult segmentation corresponds to 33 vertebral segments.
-
- General Anatomy & Musculoskeletal System (THIEME Atlas), p. 5423
Structure of a Somite
Each somite initially forms as a cuboidal epithelial block arranged around a small central cavity (somitocoele). In transverse section they are roughly triangular. As differentiation proceeds, the somite reorganises into three distinct zones:
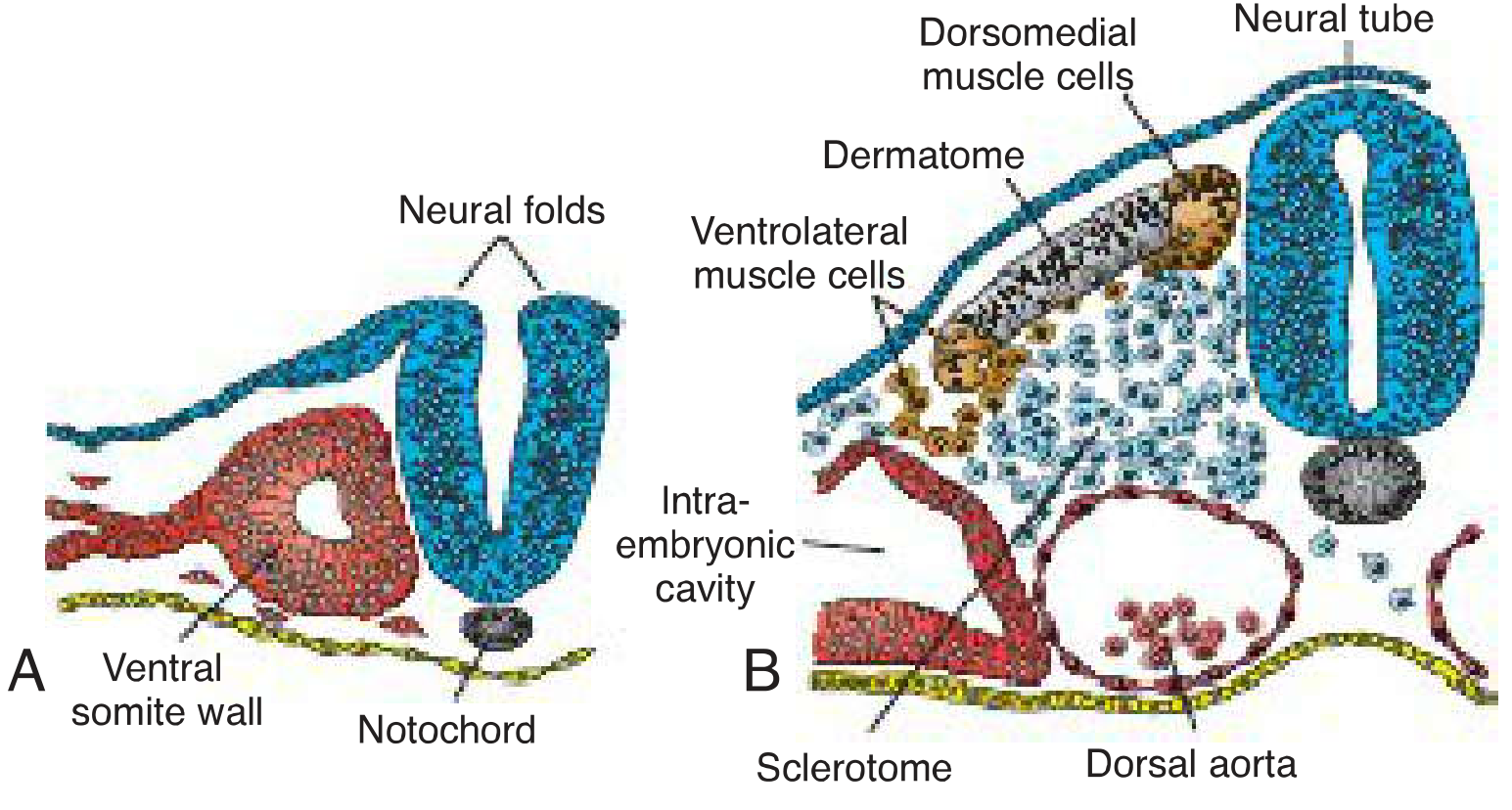
Langman's Medical Embryology Fig. 10.1 - Somite differentiation. (A) Early somite around neural tube with notochord below. (B) Sclerotome forms ventrally as cells lose epithelial arrangement; dermatome remains dorsally; myotome forms between them.
Three Compartments of a Differentiated Somite
1. SCLEROTOME (Ventromedial)
- Cells in the ventromedial wall lose their epithelial arrangement and become mesenchymal
- Induced by Sonic Hedgehog (SHH) secreted by the notochord and floor plate of neural tube
- Migrates medially to surround the notochord and neural tube
- Gives rise to: vertebral column (vertebral bodies, arches, pedicles), ribs, costal cartilages, and the intervertebral discs
Key point: Each vertebra is formed by the lower half of one sclerotome + upper half of the next sclerotome (sclerotomal resegmentation). This is why spinal nerves run between vertebrae, not with them.
2. MYOTOME (Middle)
- Forms from cells in dorsomedial and ventrolateral regions of the somite
- Induced by WNT proteins from dorsal neural tube (dorsomedial) and BMP4 + FGF from lateral plate mesoderm (ventrolateral)
- Divides into:
- Epimere (epaxial muscles) - dorsal part → intrinsic (deep) back muscles; innervated by dorsal (posterior) primary ramus of spinal nerve
- Hypomere (hypaxial muscles) - ventral part → muscles of anterolateral chest/abdominal wall, and limbs; innervated by ventral (anterior) primary ramus
Persistence of segmentation: Original segmental pattern is retained only in deep back muscles (rotatores, interspinales, intertransversarii) and intercostal muscles. Superficial trunk muscles form by fusion of multiple myotomes ("polymerisation"), but the segmental neurovascular supply still reveals the original arrangement.
Limb muscles: Myotome cells at the level of limb buds migrate into the limb buds and split into dorsal (extensor) and ventral (flexor) blastemas. These are innervated by ventral rami forming the brachial and lumbosacral plexuses.
3. DERMATOME (Dorsal epithelial layer)
- The dorsal midportion of the somite remains epithelial
- Induced by neurotrophin-3 (NT-3) secreted by the dorsal neural tube
- Gives rise to: dermis and subcutaneous connective tissue of the back and skin of the trunk/limbs
Molecular Control of Somitogenesis
Somite formation is tightly regulated by a molecular segmentation clock:
| Signal | Role |
|---|---|
| WNT + FGF gradient | Maintains unsegmented presomitic mesoderm in the posterior |
| Delta-Notch signaling | Drives the oscillating clock that times each new somite pinch-off |
| FoxC1 / FoxC2 | Transcription factors expressed just before somite formation |
| Tbx6 (T-box gene) | Critical for somitogenesis; loss causes vertebral segmentation defects |
| HOX genes | Determine the identity of each somite along the craniocaudal axis |
The segmentation clock produces periodic waves of gene expression along the presomitic mesoderm. Where a wave "freezes" at the anterior determination front (set by WNT/FGF levels), a new somite boundary forms.
Clinical Significance
| Defect | Mechanism | Result |
|---|---|---|
| Hemivertebra | Failure of one half of sclerotome to develop | Congenital scoliosis |
| Klippel-Feil syndrome | Failure of cervical somite segmentation | Fusion of cervical vertebrae, short neck, low hairline |
| Spina bifida | Failure of neural arch (sclerotome) closure | Exposed spinal cord |
| Situs inversus / laterality defects | Abnormal left-right signals affecting paraxial mesoderm | Mirror-image organ arrangement |
| Tbx6 mutations | Loss of somite identity | Rib-vertebra malformations |
Summary Diagram (Epaxial vs Hypaxial)
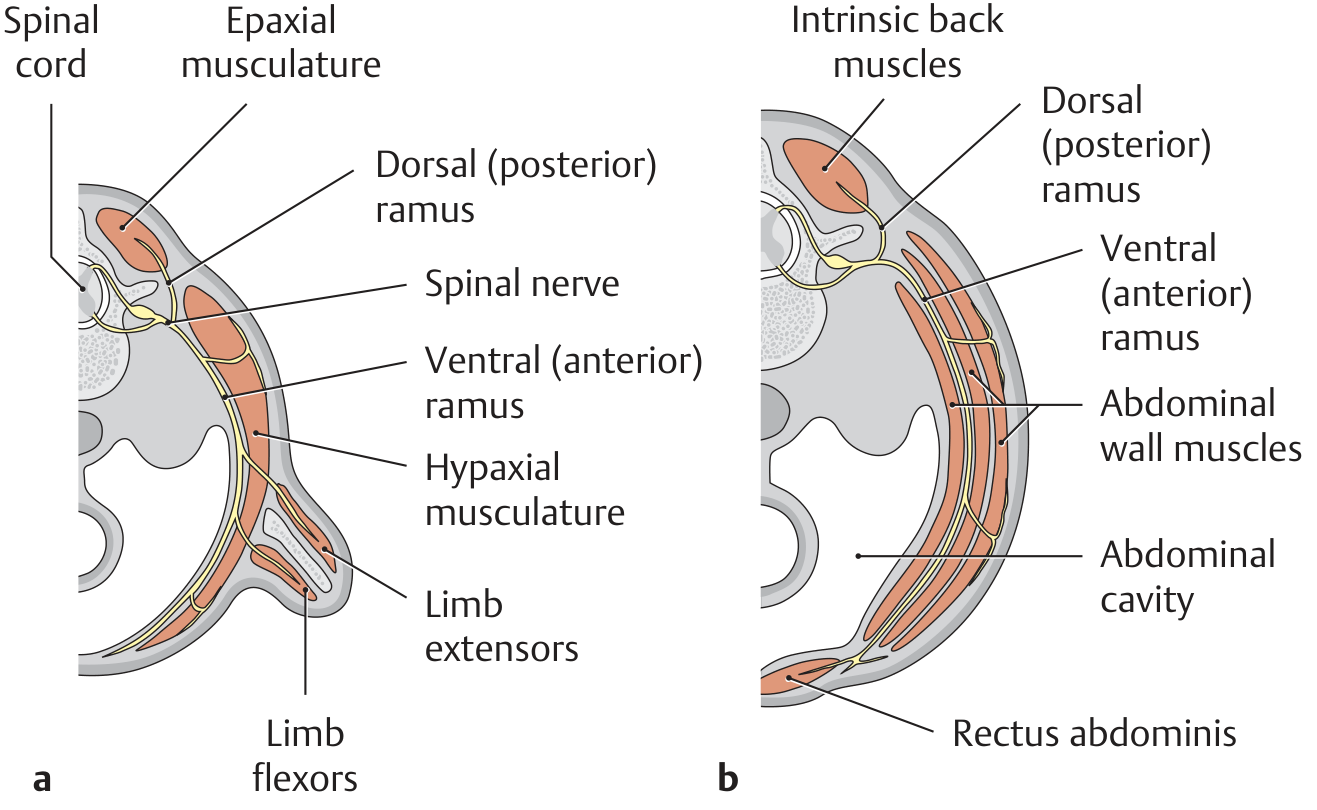
THIEME Atlas - Epaxial muscles (dorsal ramus) vs hypaxial muscles (ventral ramus). At limb level (a): hypomere forms both limb flexors and extensors. At trunk level (b): hypomere forms abdominal wall muscles and rectus abdominis.
Quick Recall Summary
Paraxial mesoderm → Somite
|
_____|_____________________
| | |
Sclerotome Myotome Dermatome
(SHH) (WNT/BMP4) (NT-3)
| | |
Vertebrae Epaxial & Dermis of
Ribs Hypaxial back & trunk
Discs muscles
- Sources: The Developing Human (Moore & Persaud), p. 212-213; Langman's Medical Embryology, p. 114, 167; THIEME Atlas - General Anatomy & Musculoskeletal System, p. 5423-5449
This is a shared conversation. Sign in to Orris to start your own chat.