Ovarian tumor pathology according to harsh Mohan
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the key content needed. Let me compile a comprehensive, well-structured answer on ovarian tumor pathology as covered in Harsh Mohan's style (which follows the same WHO classification as Robbins).
Ovarian Tumor Pathology (Harsh Mohan / WHO Classification)
Note: Harsh Mohan's Textbook of Pathology is not directly available in this library, but it follows the WHO classification identical to Robbins & Cotran. The content below is drawn from Robbins & Cotran Pathologic Basis of Disease and Robbins & Kumar Basic Pathology, which are the primary reference sources Harsh Mohan cites throughout his text.
Overview and Classification
Ovarian tumors arise from three main cell lineages:
- Surface/fallopian tube epithelium (and endometriosis)
- Germ cells
- Gonadal stroma (sex cord-stromal cells)
About 80% of ovarian tumors are benign; they occur mostly in women aged 20-45. Malignant tumors are more common between 45-65 years. Ovarian cancer accounts for 3% of cancers in females and is the fifth most common cause of cancer death in women.
WHO Classification of Ovarian Neoplasms
| Category | Subtypes |
|---|---|
| Surface Epithelial-Stromal Tumors | Serous, Mucinous, Endometrioid, Clear cell, Brenner tumors |
| Sex Cord-Stromal Tumors | Granulosa cell, Fibroma, Fibrothecoma, Thecoma, Sertoli-Leydig cell, Steroid cell tumors |
| Germ Cell Tumors | Teratoma (mature/immature), Dysgerminoma, Yolk sac tumor, Choriocarcinoma, Embryonal carcinoma, Gonadoblastoma |
| Metastatic Tumors | Krukenberg tumor (from GIT, breast) |
Each major category has benign, borderline (low malignant potential), and malignant variants.
Type I vs. Type II Ovarian Carcinoma (Pathogenesis)
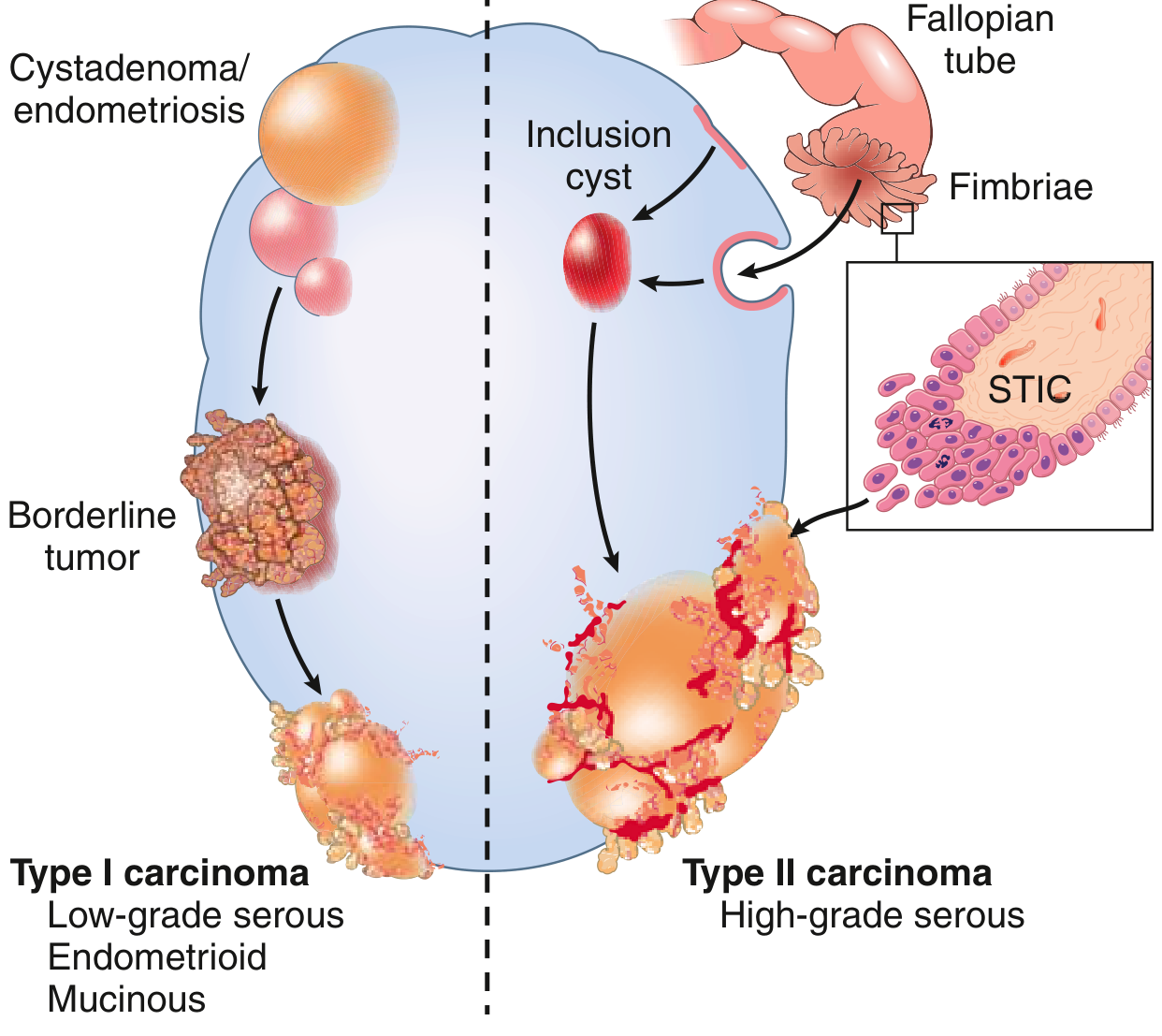
| Feature | Type I | Type II |
|---|---|---|
| Grade | Low-grade | High-grade |
| Precursor | Borderline tumors, endometriosis | Serous tubal intraepithelial carcinoma (STIC), inclusion cysts |
| Histology | Low-grade serous, mucinous, endometrioid | High-grade serous carcinoma (most common) |
| Behavior | Slow-growing, confined to ovary longer | Aggressive, rapidly disseminating |
| Key mutations | KRAS, BRAF, PTEN, PIK3CA, ARID1A | TP53 (>95%), BRCA1/2 |
I. Surface Epithelial Tumors (~65% of all ovarian tumors; 90% of malignancies)
A. Serous Tumors (most common epithelial tumor)
- 70% benign or borderline, 30% malignant
- Benign/borderline: ages 20-45; serous carcinomas: older (familial cases earlier)
- Risk factors: increasing age, nulliparity, early menarche/late menopause, BRCA1/BRCA2 mutations (20-60% lifetime risk by age 70)
- OCP use reduces risk (suppression of ovulation)
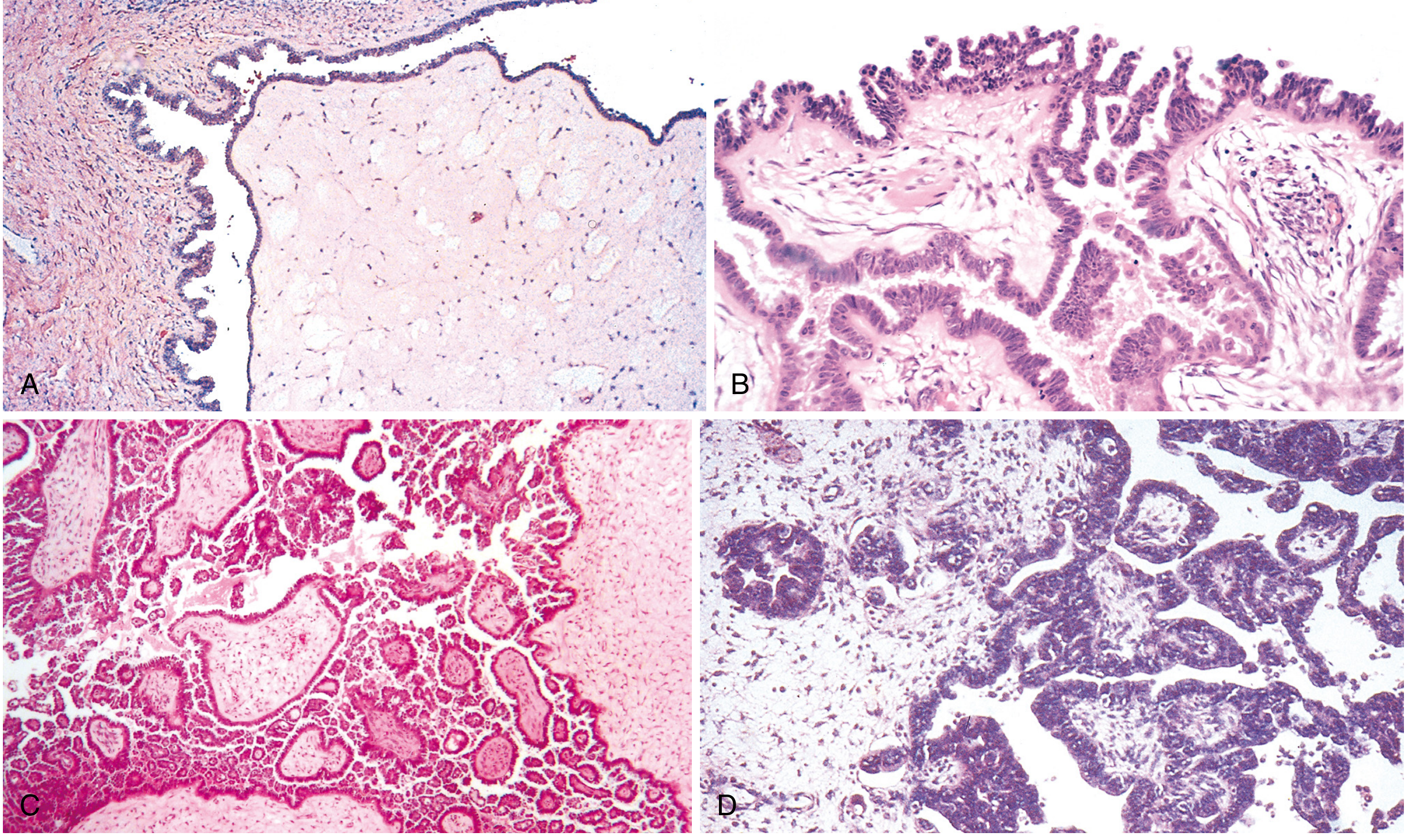
Morphology:
- Serous cystadenoma (benign): lined by single layer of columnar, ciliated cells resembling fallopian tube epithelium; may be papillary; bilateral in 20%
- Borderline serous tumor: increased architectural complexity, epithelial stratification without stromal invasion; psammoma bodies common
- Low-grade serous carcinoma: complex micropapillary growth; KRAS/BRAF mutations
- High-grade serous carcinoma: marked nuclear atypia, brisk mitoses, stromal invasion; TP53 mutations (>95%); often bilateral; frequently diagnosed at advanced stage; psammoma bodies (calcified concentric laminations) are a hallmark
B. Mucinous Tumors
- Less common than serous; can grow to enormous size (>25 kg recorded)
- Bilateral in only 5% (vs. 20-25% for serous) - ovarian surface rarely involved
- Key mutation: KRAS (present in benign, borderline, and malignant mucinous tumors - suggests a stepwise progression)
- Origin: likely from mucinous glands of teratomas, Brenner tumors, or Müllerian epithelium with mucinous differentiation
Morphology:
- Benign: tall columnar cells with apical mucin, no cilia; gastric/intestinal differentiation; multiloculated, filled with sticky gelatinous fluid
- Borderline: epithelial stratification, tufting, papillary intraglandular growth; resembles intestinal villous adenoma
- Malignant: confluent glandular "expansive" invasion or desmoplastic stromal invasion
- Pseudomyxoma peritonei: gelatinous mucinous implants in peritoneum - usually from appendiceal primary, not ovarian
C. Endometrioid Tumors
- Distinguished by tubular glands resembling endometrium
- 40% bilateral at presentation
- Associated with endometriosis (precursor in 15-20% of cases)
- Share molecular features with endometrial carcinoma: PTEN, PIK3CA, ARID1A, KRAS mutations
- 5-year survival for stage I: ~75%
D. Clear Cell Carcinoma
- Large epithelial cells with abundant clear cytoplasm (resembles hypersecretory gestational endometrium)
- Now regarded as a variant of endometrioid adenocarcinoma
- Shared mutations: PIK3CA, ARID1A, KRAS, PTEN, TP53
- Often associated with endometriosis or endometrioid carcinoma
- Confined to ovary: 90% 5-year survival; advanced stage: poor prognosis
E. Brenner Tumors (Transitional Cell Tumors)
- ~10% of ovarian epithelial tumors
- Usually unilateral (~90%); 90% are benign
- Solid or cystic; range from <1 cm to 20-30 cm
- Morphology: fibrous stroma (resembling normal ovary) with sharply demarcated nests of transitional (urothelium-like) epithelial cells, often with mucinous glands in centers (the "Walthard cell nests")
- Malignant Brenner: rare; show invasion
II. Germ Cell Tumors (~15-20% of ovarian tumors)
A. Teratomas
1. Mature Cystic Teratoma (Dermoid Cyst) - most common
- Most common ovarian tumor in women <30 years
- Contains well-differentiated tissues from all three germ layers: skin, hair follicles, sebaceous glands, teeth, bone, brain, thyroid
- Benign in >99% of cases; malignant transformation in <1% (usually squamous cell carcinoma)
- Bilateral in 10-15%
2. Immature Teratoma
- Contains immature (embryonic) tissue, particularly primitive neuroepithelium
- Graded 1-3 based on amount of immature neural tissue
- Rapidly growing, penetrates capsule, local/distant spread
- Stage I, grade 1: excellent prognosis
- Grade 2-3: treated with adjuvant chemotherapy
3. Monodermal (Specialized) Teratomas
- Struma ovarii: composed entirely of thyroid tissue; may cause hyperthyroidism
- Carcinoid: from intestinal tissue; if >7 cm, may cause carcinoid syndrome even without hepatic metastases (ovarian veins → systemic circulation directly)
- Strumal carcinoid: combination of both
B. Dysgerminoma
- Ovarian counterpart of testicular seminoma
- Most common malignant germ cell tumor (~50% of malignant GCTs)
- 75% occur in 2nd and 3rd decades; may arise in gonadal dysgenesis
- Most have no endocrine activity; a few produce hCG (syncytiotrophoblastic giant cells)
- Markers: OCT3, OCT4, NANOG (stem cell); KIT (receptor tyrosine kinase) - KIT mutations in 30-50%
- Associated with isochromosome 12p
Morphology:
- 80-90% unilateral; solid, yellow-white to gray-pink, soft and fleshy
- Large vesicular cells (resembling primordial germ cells) with distinct cell membranes and centrally placed nuclei
- Divided into lobules by fibrous septa infiltrated by lymphocytes (identical histology to seminoma)
- Excellent prognosis - highly radiosensitive; 5-year survival >90%
C. Yolk Sac Tumor (Endodermal Sinus Tumor)
- Second most common malignant GCT in children/young women
- Produces AFP (alpha-fetoprotein) - used as tumor marker
- Schiller-Duval bodies (perivascular pseudorosettes) - pathognomonic
- Aggressive; treated with BEP chemotherapy (Bleomycin-Etoposide-Cisplatin)
D. Choriocarcinoma (Non-gestational)
- Extremely rare, highly malignant
- Produces hCG (beta-hCG tumor marker)
- Composed of cytotrophoblasts and syncytiotrophoblasts
- Occurs in young girls; causes isosexual precocious puberty
E. Embryonal Carcinoma
- Rare, highly malignant
- Produces both AFP and hCG
- Large primitive cells with prominent nucleoli
III. Sex Cord-Stromal Tumors (~5-10% of ovarian tumors)
A. Granulosa Cell Tumor
- Most common malignant sex cord-stromal tumor
- Functionally active: secretes estrogens - leads to:
- Precocious puberty (in children)
- Menstrual irregularities, endometrial hyperplasia/carcinoma (in adults)
- Postmenopausal bleeding (in elderly)
- Call-Exner bodies: small follicle-like spaces filled with eosinophilic secretion surrounded by granulosa cells - pathognomonic
- FOXL2 mutation (C134W) in ~97% - molecular marker
- Indolent but late recurrences possible (up to 30 years); 5-year survival ~90%
B. Thecoma
- Usually benign, unilateral, occurs in postmenopausal women
- Estrogen-secreting → endometrial hyperplasia
- Lipid-laden stromal cells; yellow cut surface
C. Fibroma
- Benign, most common sex cord-stromal tumor (overall)
- Meigs Syndrome: fibroma + ascites + right pleural effusion (resolves after tumor removal)
- Non-functional (no hormone secretion)
- Firm, white, whorled on cut section
D. Sertoli-Leydig Cell Tumor (Androblastoma)
- Rare; occurs in young women (20-30 years)
- Androgen-secreting → virilization: hirsutism, voice deepening, clitoromegaly, breast atrophy
- Well-differentiated: tubules lined by Sertoli cells with clusters of Leydig cells
- Usually benign/low-grade malignancy
IV. Metastatic Tumors (Krukenberg Tumor)
- Secondary tumors to ovary from primary sites: stomach (most common), colon, breast, appendix
- Krukenberg tumor: bilateral ovarian metastases characterized by mucin-secreting signet ring cells in a cellular ovarian stroma
- Stomach is the most common primary site (~70%)
- Presents with bilateral solid ovarian masses
- Poor prognosis (usually indicates systemic disease)
Key Tumor Markers Summary
| Tumor | Marker |
|---|---|
| High-grade serous carcinoma | CA-125 |
| Mucinous carcinoma | CEA, CA 19-9 |
| Dysgerminoma | LDH, PLAP |
| Yolk sac tumor | AFP |
| Choriocarcinoma | β-hCG |
| Granulosa cell tumor | Inhibin, AMH, FOXL2 |
| Immature teratoma | AFP (if neuroepithelium present) |
Important Histological Landmarks
| Feature | Tumor |
|---|---|
| Psammoma bodies | Serous carcinoma (also papillary thyroid Ca) |
| Call-Exner bodies | Granulosa cell tumor |
| Schiller-Duval bodies | Yolk sac tumor |
| Signet ring cells in stroma | Krukenberg tumor |
| Walthard cell nests | Brenner tumor |
| Coffee-bean nuclei | Granulosa cell tumor |
| Reinke crystals | Leydig cell tumor |
| Meigs syndrome | Fibroma |
Sources: Robbins & Cotran Pathologic Basis of Disease (10th ed.) - Chapter 22: Female Genital Tract; Robbins & Kumar Basic Pathology - Chapter 17
This is a shared conversation. Sign in to Orris to start your own chat.