Iron deficiency anemia pathology lab diagnosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"iron deficiency anemia"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Here is the full synthesis:
Iron Deficiency Anemia: Pathology & Laboratory Diagnosis
Overview
Iron deficiency is the most common nutritional disorder worldwide and the leading cause of microcytic hypochromic anemia. It results from inadequate hemoglobin synthesis due to depleted iron stores. - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 612
Iron Metabolism (Pathophysiologic Basis)
Normal total body iron is ~3450 mg in males and ~2450 mg in females, distributed as follows:
| Pool | Males (mg) | Females (mg) |
|---|---|---|
| Hemoglobin | 2100 | 1750 |
| Myoglobin | 300 | 250 |
| Enzymes | 50 | 50 |
| Storage (ferritin/hemosiderin) | 1000 | 400 |
- Dietary iron is absorbed in the proximal duodenum; ~20% of heme iron is absorbed vs. only 1-2% of nonheme iron.
- Hepcidin (liver-derived peptide) is the master regulator: it degrades ferroportin, blocking iron transfer from enterocytes and macrophages into plasma. In IDA, hepcidin falls to very low levels, maximizing absorption.
- Ferritin is the primary storage form; serum ferritin correlates with total body iron stores (normal ~12-150 µg/L; IDA: <12 µg/L; iron overload: up to 5000 µg/L).
- Hemosiderin is degraded ferritin aggregates that stain blue-black with Prussian blue (potassium ferrocyanide) stain.
- Robbins, Cotran & Kumar, pp. 612-614
Etiology / Causes
- Dietary deficiency - infants (low iron in milk), vegans, elderly, poverty
- Impaired absorption - celiac disease, gastrectomy, bariatric surgery, H. pylori gastritis, PPIs, IRIDA (TMPRSS6 mutations with high hepcidin)
- Increased requirements - pregnancy, growth spurts, erythropoiesis-stimulating agents
- Chronic blood loss (most common in developed countries):
- GI: peptic ulcer, colon cancer, angiodysplasias, IBD, hookworm
- Gynecologic: heavy menstrual bleeding, fibroids
- Urinary: PNH, bladder cancer
- Iatrogenic: hemodialysis, excess phlebotomy
In adult males and postmenopausal females, iron deficiency must be attributed to GI blood loss until proven otherwise - missing this is missing a possible GI cancer.
- Robbins, Cotran & Kumar, p. 614; Harrison's 22E, Table 102-2
Sequential Stages of Iron Depletion
IDA develops in three progressive stages - this is key for understanding lab changes:
| Stage | Iron Stores | Serum Iron/TIBC | Hemoglobin | CBC |
|---|---|---|---|---|
| 1 - Pre-latent (iron depletion) | Depleted (low ferritin) | Normal | Normal | Normal |
| 2 - Latent (iron-deficient erythropoiesis) | Absent | Low serum iron, high TIBC, low Tsat | Normal or mildly reduced | Normal MCV, increased RDW |
| 3 - Iron deficiency anemia | Absent | Low serum iron, high TIBC, very low Tsat | Reduced | Microcytic, hypochromic |
Anemia only appears when stores are completely exhausted. The earliest detectable change is a falling serum ferritin. - Robbins, p. 614
Laboratory Diagnosis: Complete Panel
1. Complete Blood Count (CBC)
| Parameter | Finding in IDA |
|---|---|
| Hemoglobin / Hematocrit | Decreased |
| MCV | Low (<80 fL) - microcytic |
| MCH | Low - hypochromic |
| MCHC | Low |
| RDW | High (anisocytosis - hallmark of IDA, distinguishes from thalassemia) |
| Reticulocyte count | Low (hypoproliferative) |
| Platelets | May be elevated (reactive thrombocytosis) - common in IDA; also may be low |
| WBC | Usually normal |
2. Peripheral Blood Smear Morphology

Fig. 14.22 - Iron deficiency anemia peripheral blood smear. Hypochromic microcytic RBCs with enlarged central pallor (>1/3 cell diameter), a narrow peripheral rim of hemoglobin, and "pencil cells" (elongated poikilocytes). A single neutrophil for comparison. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Key morphologic features:
- Hypochromia: Zone of central pallor enlarged beyond 1/3 cell diameter; hemoglobin seen only in a narrow peripheral rim
- Microcytosis: Small red cells (MCV < 80 fL)
- "Pencil cells" (elliptocytes): Elongated, cigar-shaped poikilocytes - characteristic
- Anisocytosis + poikilocytosis
3. Iron Studies (Serum)
| Test | IDA | Normal range |
|---|---|---|
| Serum ferritin | Low (<15-30 µg/L) | 20-200 µg/L |
| Serum iron | Low | 60-170 µg/dL |
| TIBC (Transferrin) | Increased | 250-370 µg/dL |
| Transferrin saturation (Tsat) | Decreased (<10%) | 20-50% |
| Soluble transferrin receptor (sTfR) | Increased | (lab-specific) |
| Hepcidin | Very low | (lab-specific) |
| Zinc protoporphyrin (Zn-PP) | High (>80 µM/mol heme) | (screening use) |
Key diagnostic rule: Low ferritin is diagnostic of IDA. However, ferritin is an acute-phase reactant and may be falsely normal/elevated in inflammation - in that setting, use sTfR or the sTfR/log ferritin index (>2 = IDA, <1 = anemia of inflammation). - Tietz Textbook of Laboratory Medicine, p. 2994-2995
4. Bone Marrow Examination
- Gold standard (rarely needed clinically)
- Prussian blue stain shows absent stainable iron in macrophages - definitive
- Mild to moderate erythroid hyperplasia
- Erythroid precursors are small with scanty cytoplasm
MCV-Based Diagnostic Algorithm
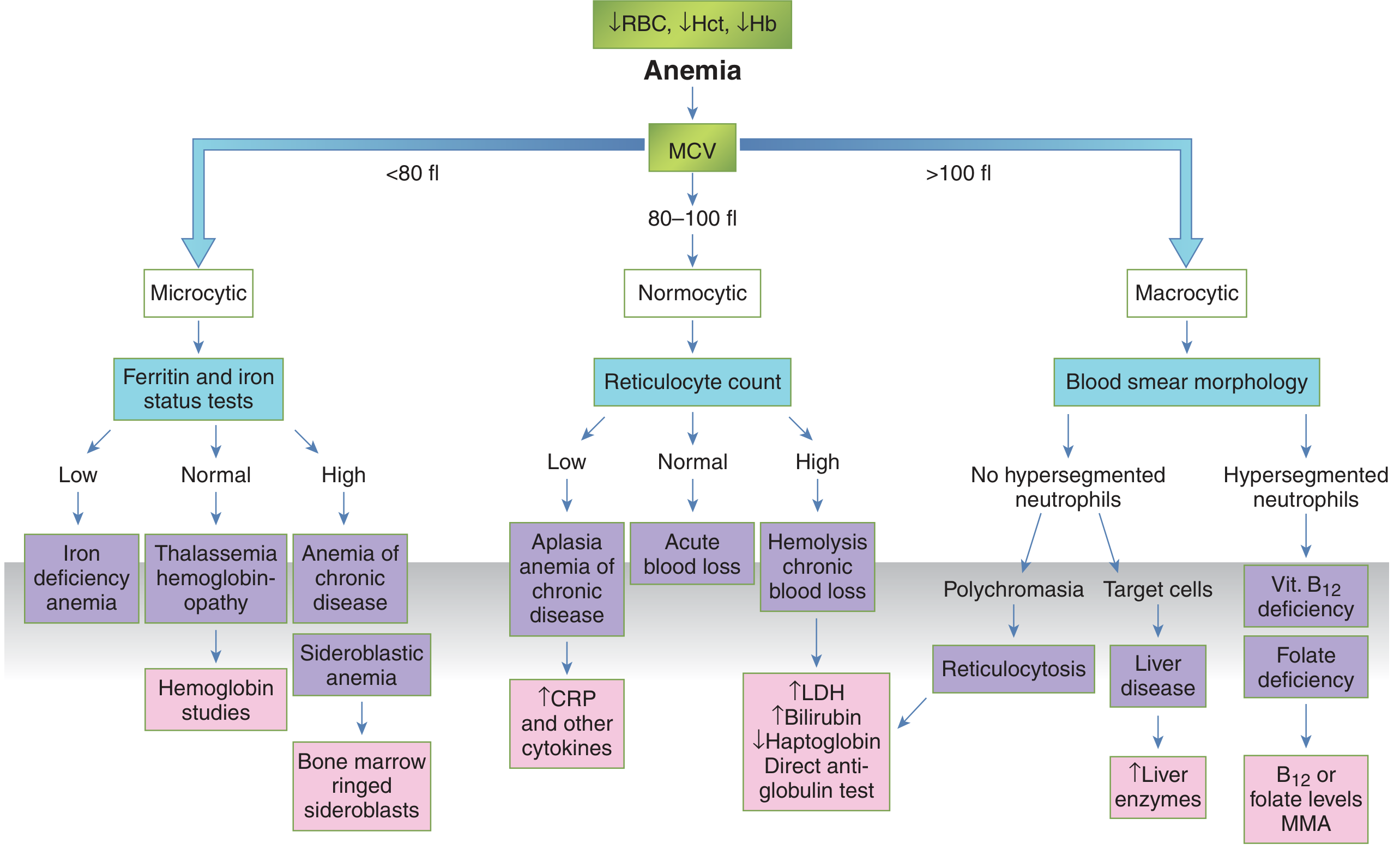
Fig. 76.11 - MCV-based algorithmic approach to anemia diagnosis. For microcytic anemia, ferritin and iron status tests are the first-line follow-up. - Tietz Textbook of Laboratory Medicine, 7th Ed.
Differential Diagnosis of Microcytic Anemia
This is the critical table for lab-based differentiation:
| Parameter | IDA | Anemia of Chronic Disease | Thalassemia Trait |
|---|---|---|---|
| Ferritin | Low (<15-30) | Normal to high (>100) | Normal to high |
| Serum iron | Low | Low | Normal to high |
| TIBC | Increased | Decreased | Normal |
| Transferrin saturation | Low (<10%) | Low (<20%) | Normal to high |
| MCV | Low | Low to normal | Very low (disproportionate) |
| RDW | High | Normal | Low to normal |
| sTfR | High | Low to normal | Normal to high |
| sTfR/log ferritin | >2 | <1 | N/A |
| Hepcidin | Very low | Normal to high | Low to normal |
| % Hypochromic RBCs | High (>6%) | High | High |
| CHr (reticulocyte Hb content) | Low | Low | Low |
Key distinguishing points:
- High RDW + low ferritin + high TIBC = IDA (vs. thalassemia where RDW is often normal/low and ferritin is not low)
- Low TIBC in anemia of chronic disease (transferrin synthesis is suppressed by inflammation)
- Mentzer index (MCV/RBC count): <13 suggests thalassemia, >13 suggests IDA
- Tietz Lab Medicine, Table 76.3; Harrison's 22E, Table 102-3
Additional/Newer Biomarkers
- Reticulocyte hemoglobin content (CHr or Ret-He): Reflects real-time iron availability for erythropoiesis; low in IDA. Useful as an early marker (drops within days of iron restriction before MCV changes).
- % Hypochromic red cells (% HYPO): >6% is significant; measured by automated analyzers.
- Zinc protoporphyrin: Elevated when zinc substitutes for iron in the last step of heme synthesis; useful in screening programs.
- Soluble transferrin receptor (sTfR): Unlike ferritin, sTfR is not affected by inflammation - useful in suspected IDA with concurrent inflammatory disease.
- Harrison's 22E, Table 102-3
Clinical Features (Pathology Correlates)
- General anemia symptoms: Fatigue, pallor, exertional dyspnea, palpitations
- Iron-deficiency specific: Koilonychia (spoon nails), glossitis, angular cheilosis, Plummer-Vinson syndrome (esophageal web + IDA + dysphagia), pica (craving non-food items like ice/clay)
- Reactive thrombocytosis: Due to shared erythroid-megakaryocyte progenitor commitment in iron-deficient state
- Children: Cognitive impairment, developmental delay, reduced immunity
Summary: Diagnostic Approach
- CBC + reticulocyte count → microcytic hypochromic anemia, high RDW, low reticulocyte count
- Peripheral smear → hypochromia, microcytosis, pencil cells
- Iron studies → low ferritin (most specific early marker), low serum iron, high TIBC, transferrin saturation <10%
- Exclude ACD/thalassemia using the table above; sTfR/log ferritin index if inflammation is present
- Bone marrow Prussian blue stain if diagnosis remains uncertain (gold standard)
- Identify the underlying cause - GI workup in adult males/postmenopausal females is mandatory
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, pp. 612-615
- Tietz Textbook of Laboratory Medicine, 7th Ed., pp. 2993-2995, Table 76.3
- Harrison's Principles of Internal Medicine, 22E (2025), Table 102-2 and 102-3
This is a shared conversation. Sign in to Orris to start your own chat.