Thoracotomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive textbook content. Let me compile a thorough, well-organized response.
Thoracotomy
A thoracotomy is a surgical incision into the thoracic cavity, providing access to the lungs, heart, great vessels, esophagus, and posterior mediastinum. It remains one of the most important approaches in thoracic, cardiac, and trauma surgery.
Indications
The most frequent indication is lung cancer resection, but thoracotomy is used for access to:
-
Lung and major bronchi (pneumonectomy, lobectomy, segmentectomy)
-
Pleura (pleurectomy, decortication)
-
Thoracic aorta
-
Esophagus (esophagectomy, esophageal repair)
-
Posterior mediastinum (tumors, cysts)
-
Trauma (hemothorax, cardiac wounds, aortic injury)
-
Cardiac surgery (when sternotomy is not suitable)
-
Bailey and Love's Short Practice of Surgery 28th Edition, p. 1009
Types of Thoracotomy
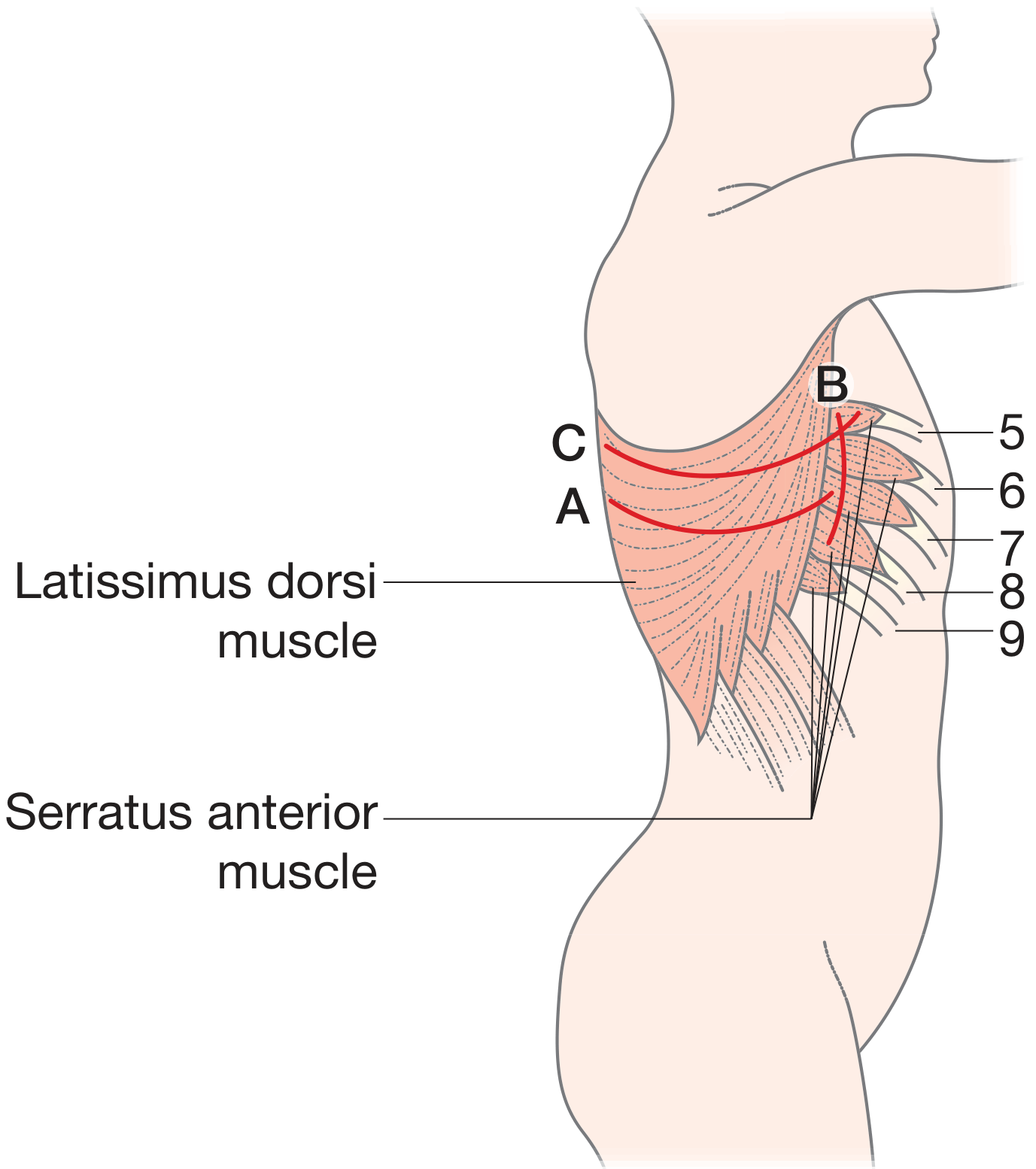
1. Posterolateral Thoracotomy (Standard)
The most widely used elective approach. Provides the best exposure for structures that are posterior - lungs, esophagus, thoracic aorta, and posterior mediastinum.
Patient position: Lateral decubitus, affected side up.
Incision: Passes 1-2 cm below the tip of the scapula, extending posteriorly and superiorly between the medial border of the scapula and the spine.
Layers encountered:
- Skin and subcutaneous tissue
- Latissimus dorsi - divided with coagulating diathermy
- Plane deep to scapula and serratus anterior is developed manually
- 6th rib periosteum is scored; intercostal muscle cut just above the rib
- Pleura entered by blunt dissection
- Rib spreader inserted gently (to prevent fracture)
Anesthesia: Requires a double-lumen endotracheal tube for one-lung ventilation - ventilates the non-operated lung while the operative lung collapses to facilitate surgery. This also protects the non-operated lung.
- Bailey and Love's, p. 1009; Schwartz's Principles of Surgery 11e
2. Anterolateral Thoracotomy
Most versatile incision for emergent thoracic exploration. Allows quick entry into the chest with the patient supine, which is critical in hemodynamic instability (the lateral decubitus position compromises resuscitation efforts).
Incision location: Fifth interspace, inframammary line.
Extends to: "Clamshell" thoracotomy - the original incision extended across the sternum with a Lebsche knife, giving bilateral thoracic access.
-
Internal mammary arteries must be ligated when the sternum is divided.
-
Provides access to: heart, lungs, descending aorta, pulmonary hilum, esophagus.
-
Schwartz's Principles of Surgery 11e, p. (block 3)
3. Clamshell (Bilateral Anterior) Thoracotomy
A bilateral anterior thoracotomy incision with transverse sternotomy. Provides the widest exposure to the heart and mediastinum.
Key uses:
-
Preferred approach for double-lung transplantation in many centers
-
Bilateral thoracic trauma
-
Mediastinal tumors requiring bilateral access
-
Schwartz's Principles of Surgery 11e
4. Median Sternotomy
Not a true thoracotomy, but the principal approach for cardiac surgery. A midline sternal split from suprasternal notch to xiphoid. Both pleural cavities are accessible but entry can be avoided. Used for anterior mediastinal structures.
Trap-door thoracotomy: Combines upper sternotomy from sternal notch to 4th intercostal space with dual left lateral incisions (supraclavicular + 4th interspace anterolateral) - used for access to the proximal left subclavian artery, especially post-resuscitative thoracotomy.
5. Mini-Thoracotomy (Muscle-Sparing)
A shorter incision (6-8 cm) along the standard incision line, covering the width of the latissimus dorsi anterior to the triangle of auscultation. Useful when full access is not needed, and can be extended if necessary.
Standard incision line (Fischer's concept) - defined by 3 points:
- A point in the 4th or 5th intercostal space along the midclavicular line
- A point one fingerbreadth under the tip of the scapula
- A point equidistant between the spine and scapula at the level of the middle of the scapula
The line connecting these three points can accommodate virtually all thoracotomy variants.
- Fischer's Mastery of Surgery 8th Edition
6. Right vs. Left Posterolateral Approach
| Approach | Best for |
|---|---|
| Left posterolateral | Posterior heart, descending thoracic aorta, distal esophageal injuries, left lower lobe |
| Right posterolateral | Upper and middle thoracic esophagus, trachea/main stem bronchi near carina, right lung |
- Fischer's Mastery of Surgery 8th Edition
Resuscitative Thoracotomy (Emergency Department Thoracotomy - EDT)
A life-saving procedure performed outside the operating room for patients in extremis or recent traumatic arrest.
Indications
- Trauma victims with severe refractory instability or cardiac arrest
- Nontraumatic hypothermic cardiac arrest
Contraindications
- Blunt trauma cardiac arrest without signs of life
- Obvious non-survivable injuries
- Initial rhythm of asystole without signs of life
- Signs of prolonged arrest (lividity, rigor mortis)
Goals of EDT
- Release cardiac tamponade
- Control cardiac hemorrhage
- Control massive intrathoracic hemorrhage
- Perform open cardiac massage
- Cross-clamp descending aorta (to redistribute blood to heart and brain)
Approach: Left anterolateral thoracotomy at the 4th or 5th intercostal space - no special positioning or equipment required. Can be quickly converted to a clamshell for bilateral access.
Survival rates are poor overall, but EDT is not futile in the correct setting (penetrating trauma, witnessed arrest, with surgical backup available). The 2003 ACSCOT guidelines and subsequent publications provide selection criteria.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Thoracotomy Closure
- Intercostal space: 3-5 figure-of-eight stitches with heavy Vicryl (No.2 Vicryl, blunt-point needle). Confirm chest tube position and inflate lung before tightening.
- Muscle layers: Latissimus dorsi and serratus anterior closed by approximating the divided midpoints.
- Chest tube: Placed at conclusion of most thoracic operations to drain air (if air leak present) and blood/fluid. Removed when air leak resolves and drainage <400 mL/24 hours (current evidence-based threshold).
- Fischer's Mastery of Surgery 8th Edition; Schwartz's Principles of Surgery 11e
Postoperative Analgesia
Pain control after thoracotomy is critical - inadequate analgesia impairs deep breathing and coughing, leading to pulmonary complications.
Methods:
- Thoracic epidural catheter - placed preoperatively by anesthesia; reduces incidence of pulmonary complications
- Paravertebral catheter - surgically placed intraoperatively, increasingly popular
- Intercostal nerve blocks - long-acting local anesthetic infiltrated intraoperatively
- IV/oral analgesics as adjuncts
Chronic post-thoracotomy pain (PTPS) is a recognized complication - intercostal nerve injury during rib spreading is the primary mechanism. Muscle-sparing approaches and careful rib retraction reduce this risk.
- Bailey and Love's, p. 1009-1010; Maingot's Abdominal Operations
VATS as an Alternative
Video-assisted thoracoscopic surgery (VATS) is now the approach of choice for early-stage lung resections. Key advantages over open thoracotomy:
- No rib spreading
- Reduced postoperative pain
- Shorter length of stay
- Faster recovery, especially in frail patients
- Full hilar dissection and lymph node staging achievable via uniportal, 2-port, or 3-port techniques
Open thoracotomy remains preferred when VATS is not feasible (e.g., large central tumors, prior pleural disease, conversion due to bleeding).
- Bailey and Love's, p. 1010; Fishman's Pulmonary Diseases and Disorders
Summary of Approaches by Indication
| Clinical Scenario | Preferred Approach |
|---|---|
| Elective lung resection | Posterolateral thoracotomy or VATS |
| Esophageal surgery (upper/mid) | Right posterolateral thoracotomy |
| Esophageal surgery (distal) | Left 6th ICS posterolateral thoracotomy |
| Emergent thoracic exploration | Anterolateral thoracotomy (supine) |
| Penetrating cardiac wound | Left anterolateral or anterolateral → clamshell |
| Cardiac surgery | Median sternotomy |
| Double lung transplant | Clamshell (bilateral anterior + sternotomy) |
| Proximal left subclavian injury | Trap-door thoracotomy |
| Pancoast tumor | Extended posterolateral (standard line extended toward head) |
| Extrapleural pneumonectomy | Extended standard line + anterior extension to hypochondrium |
This is a shared conversation. Sign in to Orris to start your own chat.