diarrhea in detail its pathophysiolgy mechanism and types in detail and its diagnostic criteria and its treatment and managment criteria and anti diarrhea drugs in detail im a medical student
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from all major sources. Let me compile the complete, detailed response.
Diarrhea — Complete Medical Review
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles of Internal Medicine 22E; Guyton & Hall Textbook of Medical Physiology; Katzung's Basic & Clinical Pharmacology 16E; Rosen's Emergency Medicine
1. Definition
Diarrhea is a symptom, not a disease. Most clinicians define it as:
- ≥3 unformed/liquid stools per day, OR
- Stool weight >200 g/day in Western countries (up to 300 g on high-fiber diets in developing countries), OR
- Stool that "takes the form of the container"
Importantly, ~20% of patients referred for "diarrhea" evaluation have normal stool weight — they report it because of increased frequency or loose consistency. Fecal incontinence must always be distinguished from true diarrhea.
Duration classification (Rosen's/Harrison's):
| Duration | Category |
|---|---|
| < 7 days | Acute |
| 7–13 days | Prolonged |
| 14–29 days | Persistent |
| ≥ 30 days (or ≥4 weeks) | Chronic |
2. Pathophysiology — The Core Mechanism
Normal GI Fluid Handling
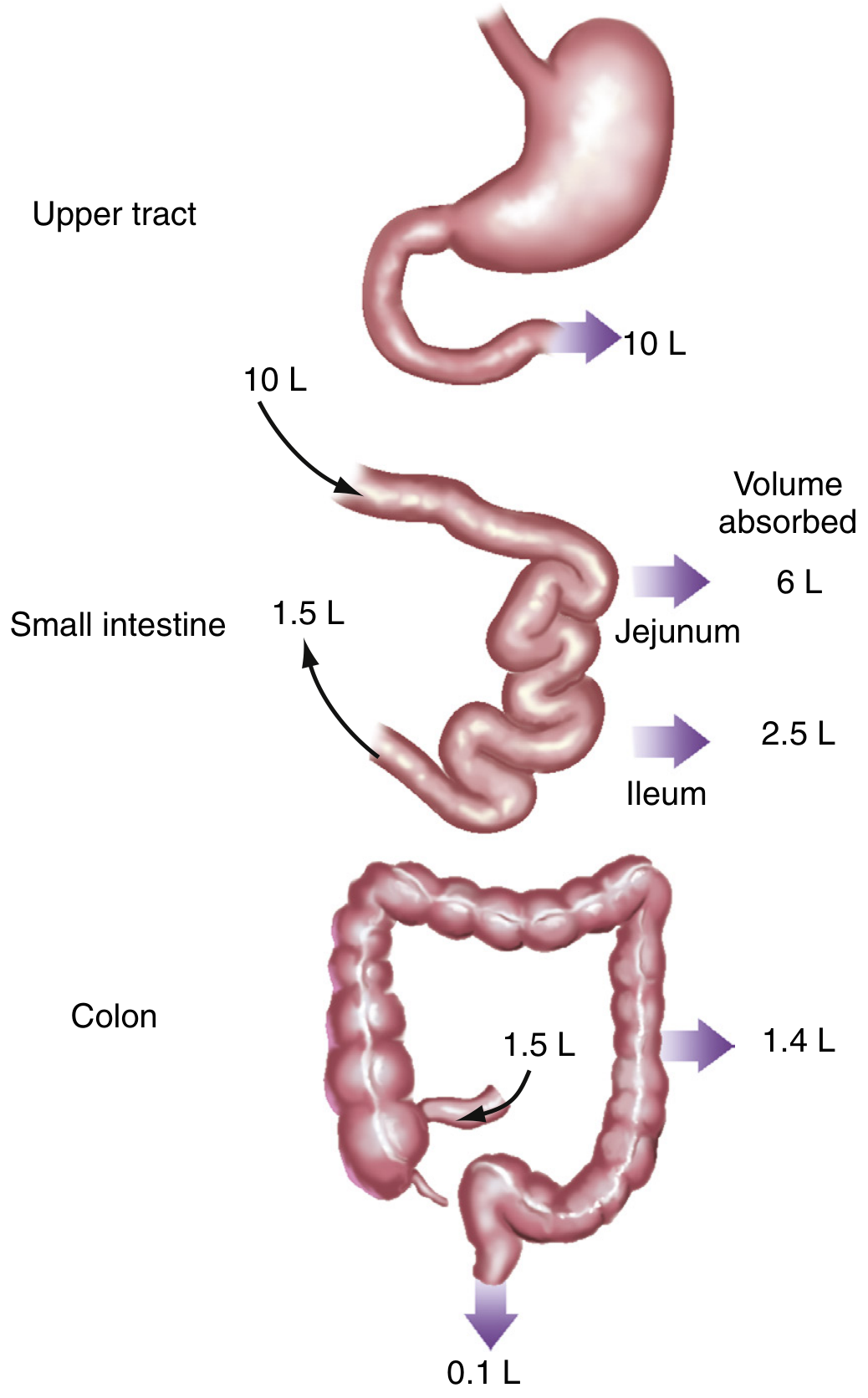
The small intestine and colon together absorb 99% of ~9–10 L of daily fluid passing the ligament of Treitz (oral intake + salivary, gastric, biliary, and pancreatic secretions). A reduction in net water absorption of as little as 1% is enough to produce diarrhea. (Sleisenger & Fordtran's)
Water itself is not actively transported — it follows osmotic gradients created by electrolyte and nutrient transport across paracellular and transcellular pathways.
Three Fundamental Mechanisms
| Mechanism | Pathophysiology |
|---|---|
| 1. Altered mucosal transport | Increased secretion or decreased absorption of water & electrolytes in small intestine or colon |
| 2. Rapid transit | Reduced contact time in colon; fluid rushed through before adequate absorption |
| 3. Altered stool solid composition | Reduced water-binding capacity (e.g., steatorrhea) → looser stools despite normal water volume |
In most diseases, multiple mechanisms interplay — epithelial function, motor function, and luminal composition all contribute.
Infectious Mechanisms (4 specific types — Rosen's)
- Ingestion of preformed toxins — toxin already made before eating (e.g., S. aureus, B. cereus); onset 1–6 hours
- Adherence to intestinal cell walls — pathogen sticks to epithelium and disrupts brush border (e.g., ETEC, Giardia)
- Mucosal cell invasion — organism penetrates mucosa (e.g., Shigella, Campylobacter, Salmonella)
- Enterotoxin/cytotoxin production — toxin produced in vivo stimulates secretion (e.g., cholera toxin, C. difficile toxins A/B)
Each mechanism leads to increased fluid secretion or decreased fluid absorption, resulting in diarrhea.
3. Types / Classification of Diarrhea
A. By Duration
- Acute/Prolonged (≤13 days): Usually viral or bacterial
- Persistent/Chronic (>13 days): Protozoa, parasites, non-infectious
B. By Pathophysiological Mechanism
1. Osmotic Diarrhea
- Mechanism: Poorly absorbable solutes (non-electrolytes) remain in the lumen → osmotic gradient draws water in → intestinal distension → diarrhea
- Key feature: Stops with fasting
- Fecal osmotic gap: HIGH (>125 mOsm/kg) — unabsorbed solutes account for stool osmolality
- Formula: Osmotic gap = 290 – 2×([Na⁺] + [K⁺]) in stool water
- Causes: Lactase deficiency (lactose malabsorption), magnesium-containing antacids/laxatives, lactulose, celiac disease, short bowel syndrome, mannitol/sorbitol ingestion
2. Secretory Diarrhea
- Mechanism: Active secretion of Cl⁻ (via CFTR) or inhibition of neutral NaCl absorption → net fluid secretion into lumen. Crypts of Lieberkühn are the primary secretory sites.
- Key feature: Persists with fasting; large volume (often >1 L/day)
- Fecal osmotic gap: LOW (<50 mOsm/kg) — stool osmolality accounted for almost entirely by Na⁺, K⁺, and accompanying anions
- Classic example — Cholera: Cholera toxin activates adenylyl cyclase → ↑ cAMP → opens CFTR Cl⁻ channels in crypts → massive Cl⁻ secretion followed by water → 10–12 L/day secretion (colon can only reabsorb max 6–8 L/day) → life-threatening losses (Guyton & Hall)
- Other causes: VIPoma (watery diarrhea, hypokalemia, achlorhydria — WDHA/Verner-Morrison syndrome), carcinoid syndrome (serotonin), gastrinoma, microscopic colitis, bile acid malabsorption, fatty acids in colon, congenital chloridorrhea
3. Inflammatory/Exudative Diarrhea
- Mechanism: Mucosal inflammation and ulceration → exudation of protein, blood, pus into the lumen → disrupted absorption + stimulated secretion; also increased motility
- Features: Mucus, blood, pus in stool; fever; fecal leukocytes positive; tenesmus
- Causes: IBD (UC — diffuse colonic inflammation and ulceration; Crohn's — transmural, skip lesions anywhere GI), invasive bacteria (Shigella, Campylobacter, Salmonella), C. difficile colitis, CMV, ischemic colitis, radiation colitis, colorectal cancer
4. Motility-Related Diarrhea
- Mechanism: Rapid intestinal transit reduces contact time for absorption; or paradoxically, slow motility → bacterial overgrowth → secondary malabsorption
- Causes: IBS-D (post-infectious), hyperthyroidism, diabetes (autonomic neuropathy with diarrhea predominant), post-vagotomy, psychogenic diarrhea (parasympathetic stimulation → ↑ motility + ↑ mucus secretion — Guyton), post-gastrectomy dumping syndrome
5. Malabsorptive / Fatty Diarrhea (Steatorrhea)
- Mechanism: Failure of digestion or absorption → unabsorbed fats/carbohydrates reach colon → osmotic effect + bacterial fermentation → gas + diarrhea; reduced water-binding
- Features: Bulky, greasy, foul-smelling, floating stools; Sudan stain positive; 72-hr fecal fat > 7 g/day
- Causes: Pancreatic exocrine insufficiency, celiac disease, Whipple's disease, SIBO, bile acid deficiency, lymphatic obstruction
C. By Volume
| Pattern | Likely Location |
|---|---|
| Large-volume, painless stools | Small bowel or right colon origin; rectosigmoid reservoir intact |
| Frequent small-volume painful stools | Distal colon / rectosigmoid pathology (reservoir compromised) |
IBS typically produces normal or slightly elevated 24-hr stool weight; weights >1000 g suggest secretory or infectious cause. (Sleisenger)
4. Differential Diagnosis by Setting
| Patient Group | Common Causes |
|---|---|
| Travelers | ETEC, Salmonella, Shigella, Campylobacter, Giardia, amoebiasis |
| Hospitalized/Post-antibiotic | C. difficile (pseudomembranous colitis), antibiotic-associated diarrhea |
| AIDS/Immunocompromised | Cryptosporidium, CMV, MAC, microsporidia, isosporiasis |
| Diabetics | Autonomic neuropathy, celiac disease, pancreatic insufficiency, SIBO, metformin |
| Elderly/Institutionalized | C. difficile, overflow diarrhea (fecal impaction), ischemic colitis |
| Outbreaks | Norovirus, rotavirus, Brainerd diarrhea |
5. Diagnostic Criteria & Evaluation
Acute Diarrhea — When to Investigate
Indications for stool microbiologic studies (Harrison's):
- Profuse diarrhea with signs of dehydration
- Overtly bloody stools
- Fever ≥38.5°C
- Duration >48 hours without improvement
- Recent antibiotic use
- New community outbreak
- Severe abdominal pain in patients >50 years
- Age ≥70 or immunocompromised patients
For most acute cases, no investigation is needed — illness is self-limited.
Diagnostic Workup
History: Onset and duration; volume; blood/mucus; fever; abdominal pain; tenesmus; recent travel; antibiotic/drug use; food exposures; sexual history; immunocompromise; family history of IBD
Physical Exam: Hydration status (skin turgor, mucous membranes, orthostatic vitals), abdominal tenderness, rectal exam
Stool Studies (acute):
- Culture-independent multiplex PCR — first-line (more sensitive/specific/rapid)
- Stool culture for bacteria (Salmonella, Shigella, Campylobacter, E. coli O157:H7)
- Ova and parasites (O&P) × 3 specimens
- C. difficile toxin assay / GDH + PCR
- Fecal leukocytes / calprotectin / lactoferrin — marker of inflammatory diarrhea
- Giardia/Cryptosporidium antigen tests
Stool Studies (chronic diarrhea — the "comprehensive stool analysis"):
- 24-hour stool weight: determines if true diarrhea exists (>200 g/day)
- Fecal osmotic gap = 290 – 2([Na⁺] + [K⁺]): high = osmotic, low = secretory
- Sudan stain / 72-hour fecal fat: steatorrhea screen
- Fecal pH: low (<5.5) suggests carbohydrate malabsorption
- Fecal elastase: pancreatic exocrine function
- Fecal calprotectin: IBD vs. functional (very useful noninvasive marker)
- α₁-antitrypsin clearance: protein-losing enteropathy
- Laxative screen (if factitious diarrhea suspected)
Blood Tests (chronic):
- CBC, CRP, ESR (inflammation)
- CMP (electrolytes, albumin — nutritional/absorption status)
- TSH (hyperthyroidism)
- Tissue transglutaminase IgA + total IgA (celiac screen)
- Vitamin B12, folate, iron — malabsorption markers
- Chromogranin A, 24-hr urine 5-HIAA (carcinoid)
- VIP level (VIPoma)
Endoscopy:
- Colonoscopy with biopsies: for chronic diarrhea with suspected IBD, microscopic colitis (normal gross appearance but biopsy shows collagenous/lymphocytic colitis), colorectal cancer evaluation, or blood/pus in stool
- Upper endoscopy with duodenal aspirate/biopsy: for malabsorption, giardiasis, celiac disease, Whipple's disease
- Sigmoidoscopy (without full prep): adequate for suspected proctitis or pseudomembranous colitis
Imaging:
- Abdominal CT: bowel wall thickening, mass lesions, mesenteric changes, obstruction
- CT enterography / MRI: Crohn's disease extent
- Abdominal X-ray: if ileus or toxic megacolon suspected
Management Algorithm for Acute Diarrhea
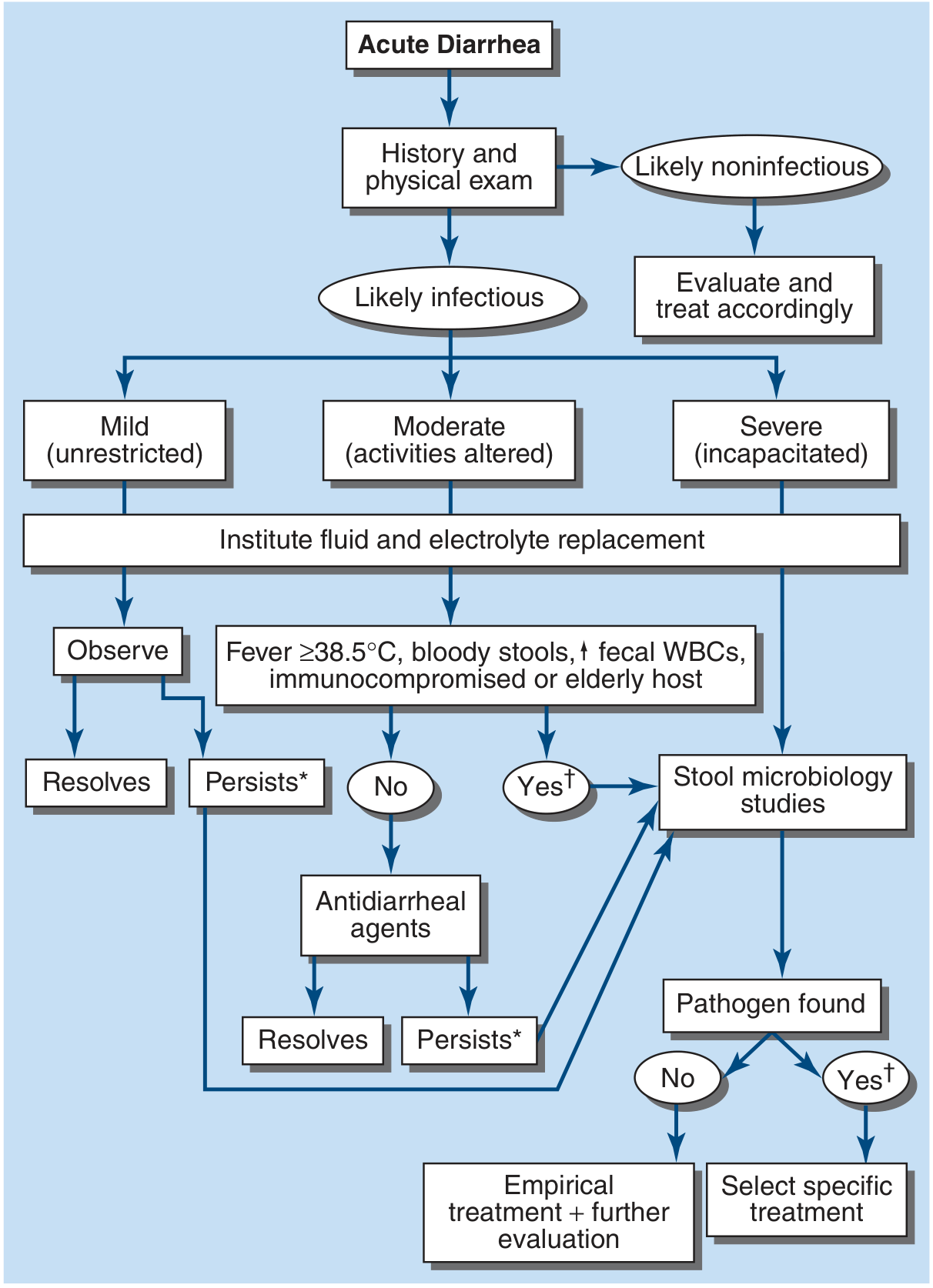
6. Treatment & Management
A. Fluid & Electrolyte Replacement — CORNERSTONE
Oral Rehydration Therapy (ORT): For mild-to-moderate dehydration. WHO ORS contains glucose + Na⁺ + K⁺ + bicarbonate/citrate. Glucose-coupled Na⁺ co-transport (SGLT1) remains intact even in secretory diarrhea, making ORT highly effective.
Intravenous fluids (Ringer's lactate or normal saline): For severe dehydration, inability to tolerate oral intake, or profound losses (e.g., cholera — volumes up to 10–12 L/day). IV therapy + antibiotics reduces cholera mortality from up to 50% to near zero (Guyton & Hall).
B. Diet
- Avoid: dairy (secondary lactase deficiency), caffeine (potentiates cramps), alcohol
- Allow: soups, saltines, bananas, mashed potatoes, rice (BRAT-type diet)
- In children: restart feeding immediately after tolerating oral intake
- Bowel rest provides only partial relief; early refeeding is preferred (Sleisenger)
C. Antimicrobial Therapy — Indications & Choices
Antibiotics are indicated in only a limited subset of acute infectious diarrhea. Clear indications: C. difficile, V. cholerae, and some cases of severe febrile dysentery. Antibiotics should generally be withheld in STEC/E. coli O157:H7 (increases HUS risk).
| Indication | Drug of Choice |
|---|---|
| Empirical (travelers' diarrhea, severe) | Azithromycin (preferred) or fluoroquinolone × 3–5 days |
| C. difficile (mild-moderate) | Vancomycin (oral) or fidaxomicin; metronidazole if vancomycin unavailable |
| Cholera | Doxycycline (single dose) or azithromycin |
| Giardiasis | Metronidazole or tinidazole |
| Amebiasis (E. histolytica) | Metronidazole then a luminal agent (paromomycin/iodoquinol) |
| Shigella (severe) | Azithromycin or fluoroquinolone |
| ETEC/travelers | Rifaximin (non-invasive), azithromycin |
Duration: typically 3–5 days; 5 days was superior for S. dysenteriae type 1. For travelers' diarrhea and cholera, single-dose therapy may be effective.
Note on fluoroquinolones: FDA now recommends against use for uncomplicated infections due to risk of tendinopathy, peripheral neuropathy, CNS effects, and aortic dissection. Azithromycin is increasingly preferred.
D. Chronic Diarrhea Management
- Treat the underlying cause (IBD → 5-ASAs, steroids, biologics; celiac → gluten-free diet; microscopic colitis → bismuth, budesonide; pancreatic insufficiency → enzyme replacement; bile acid diarrhea → cholestyramine)
- Empirical anti-motility agents for symptomatic relief when cause cannot be eliminated
- IBS-D: dietary modification (low-FODMAP), antispasmodics, rifaximin (non-absorbed antibiotic), alosetron (women with severe IBS-D), loperamide
7. Antidiarrheal Drugs — Detailed Pharmacology
Class 1: Opioid-Receptor Agonists (Anti-motility)
These act on μ-opioid receptors in the enteric nervous system to decrease intestinal motility and increase sphincter tone.
Loperamide (Imodium) — First-line antidiarrheal
- Class: Phenylpiperidine opioid derivative
- Mechanism: Agonist at peripheral μ-opioid receptors in the myenteric plexus → ↓ peristalsis, ↑ anal sphincter tone, ↓ intestinal transit time → more time for fluid and electrolyte absorption. Also inhibits Ca²⁺/calmodulin-dependent secretion.
- Key pharmacology: Very limited CNS penetration (P-glycoprotein pumps it out of the brain) → negligible abuse potential and no CNS opioid effects → available OTC without prescription
- Dosing: 4 mg initially, then 2 mg after each loose stool; max 16 mg/day
- Uses: Traveler's diarrhea, IBS-D, chronic diarrhea, chemotherapy-induced diarrhea, ileostomy output control
- Contraindications: Bloody diarrhea / dysentery, suspected invasive infection (especially STEC — risk of HUS/TTP, toxic megacolon), C. difficile (without antibiotic cover), pseudomembranous colitis, <2 years old, obstructive ileus
- Adverse effects: Constipation, abdominal distension, nausea; at very high doses (misuse) — QTc prolongation, cardiac arrhythmia
Diphenoxylate + Atropine (Lomotil) — Schedule V
- Class: Phenylpiperidine; metabolized to active metabolite difenoxin (Schedule IV)
- Mechanism: Same as loperamide — μ-opioid receptor agonism in the ENS; also small CNS effect
- Atropine is added in sub-therapeutic doses — too low to have antidiarrheal effect, but discourages misuse (anticholinergic side effects at doses required to get "high" from diphenoxylate). (Katzung)
- Poor solubility also limits IV abuse
- Dosing: 2 tablets (5 mg diphenoxylate / 0.025 mg atropine each) to start, then 1 after each diarrheal stool
- Contraindications: Same as loperamide; also jaundice; children <2 years (atropine toxicity risk)
Codeine / Tincture of Opium — used in refractory chronic diarrhea
- Full μ-opioid agonist; antidiarrheal + analgesic
- Reserved for severe chronic diarrhea unresponsive to other agents
- Higher abuse potential, CNS depression
Class 2: Bismuth Subsalicylate (Pepto-Bismol)
- Mechanism (multiple):
- Anti-secretory: bismuth and salicylate both reduce intestinal secretion
- Antimicrobial: bismuth is toxic to enteric pathogens (H. pylori, ETEC, other bacteria)
- Anti-inflammatory: salicylate component inhibits prostaglandin synthesis
- Adsorbent: binds toxins in the lumen
- Dose: 524 mg every 30–60 min as needed (max 8 doses/24 h)
- Uses: Traveler's diarrhea (prophylaxis and treatment), dyspepsia, ETEC diarrhea, vomiting with minimal diarrhea, H. pylori eradication regimens
- Efficacy: Safe and efficacious in bacterial diarrheas (Yamada's)
- Contraindications: Should NOT be used in immunocompromised patients or those with renal impairment (risk of bismuth encephalopathy — bismuth accumulates); avoid in aspirin-allergic patients; avoid in children with viral illness (Reye's syndrome risk from salicylate)
- Side effects: Black stools and black tongue (harmless — bismuth sulfide), tinnitus (salicylism at high doses), bismuth encephalopathy (with overuse)
Class 3: Antisecretory Agents
Racecadotril (Acetorphan)
- Mechanism: Enkephalinase (NEP/CD10) inhibitor → prevents breakdown of endogenous enkephalins → ↑ enkephalin activity at δ-opioid receptors → inhibits cAMP-stimulated Cl⁻ secretion without affecting motility
- Key advantage: Anti-secretory WITHOUT constipation (no motility effect) → preferred in children, secretory diarrhea
- Available in many countries (Europe, Asia, Latin America); not FDA-approved in the US
Octreotide (Somatostatin analog)
- Mechanism: Mimics somatostatin → ↓ secretion of GI hormones (VIP, serotonin, gastrin, glucagon) → ↓ intestinal secretion; also slows motility
- Uses: Carcinoid diarrhea (gold standard), VIPoma (WDHA syndrome), dumping syndrome, AIDS-related secretory diarrhea, chemotherapy-induced diarrhea, refractory secretory diarrhea
- Route: SC or IV; long-acting formulation (Sandostatin LAR) IM monthly
- Side effects: Steatorrhea (inhibits pancreatic enzyme and bile secretion), gallstone formation, bradycardia, hyperglycemia or hypoglycemia
Class 4: Adsorbents
Kaolin-Pectin (Kaopectate — old formulation)
- Mechanism: Adsorb toxins and bacteria to their surface; increase stool consistency
- Limited efficacy; replaced by bismuth in many markets
- No systemic absorption; safe in pregnancy
Attapulgite
- Hydrated magnesium aluminum silicate clay
- Binds water, toxins, and irritants in the gut
- OTC; symptomatic use only
Cholestyramine (bile acid sequestrant)
- Mechanism: Binds bile acids in the colon → prevents their pro-secretory/pro-motility effect on colonic mucosa
- Uses: Bile acid malabsorption diarrhea (type 1–3: ileal resection, primary bile acid diarrhea), post-cholecystectomy diarrhea, C. difficile toxin binding (adjunctive — limited evidence)
- Side effects: Bloating, constipation, malabsorption of fat-soluble vitamins (A, D, E, K), drug interactions (binds warfarin, thyroid hormone, digoxin — take other medications ≥1 hour before)
Class 5: Probiotics
- Mechanism: Competitive exclusion of pathogens, mucosal barrier reinforcement, immune modulation, production of antimicrobial substances
- Evidence-based uses:
- Lactobacillus rhamnosus GG and Saccharomyces boulardii: reduce duration of acute infectious diarrhea by ~1 day in children
- Reduce antibiotic-associated diarrhea (including C. difficile-associated)
- Generally safe; caution in severely immunocompromised (rare case of fungemia with S. boulardii)
Class 6: Antibiotics with Gut-Specific Action
Rifaximin
- Mechanism: Non-absorbable rifamycin antibiotic; inhibits bacterial RNA polymerase locally in the GI tract
- Uses: Traveler's diarrhea (non-invasive, non-bloody), IBS-D (reduces bacterial overgrowth; FDA-approved), hepatic encephalopathy prevention
- Advantage: Minimal systemic absorption → minimal systemic side effects, low resistance selection pressure for systemic pathogens
- Dosing for traveler's diarrhea: 200 mg TID × 3 days; for IBS-D: 550 mg TID × 14 days
Class 7: 5-HT3 Antagonists
Ondansetron
- Primarily antiemetic; also slows intestinal transit
- Used off-label for IBS-D and chemotherapy-induced diarrhea; reduces acute vomiting and diarrhea in gastroenteritis
Alosetron
- Selective 5-HT3 antagonist; slows colonic transit + reduces visceral hypersensitivity
- FDA-approved only for women with severe IBS-D unresponsive to other treatments
- Black box warning: Ischemic colitis and serious complications of constipation (requires REMS program)
Class 8: Enkephalin Analogs / μ-Opioid Agonists (Novel)
Eluxadoline (Viberzi)
- Mixed μ- and κ-opioid agonist + δ-opioid antagonist
- FDA-approved for IBS-D in adults
- Reduces abdominal pain and diarrhea; δ-antagonism prevents constipation rebound
- Contraindication: Patients without a gallbladder (pancreatitis risk); alcohol misuse
Summary Table: Antidiarrheal Drug Classes
| Drug | Class | Mechanism | Key Use | Key Contraindication |
|---|---|---|---|---|
| Loperamide | Opioid (peripheral) | ↓ peristalsis, ↑ sphincter tone | IBS-D, traveler's | Bloody diarrhea, invasive infection, STEC |
| Diphenoxylate + atropine | Opioid + anticholinergic | μ-receptor agonism | Acute/chronic | Same + children <2 yrs |
| Bismuth subsalicylate | Multi-mechanism | Antisecretory + antimicrobial | Traveler's, H. pylori | Immunocompromised, renal failure, aspirin allergy |
| Racecadotril | Enkephalinase inhibitor | ↑ enkephalins → ↓ secretion | Secretory, children | — |
| Octreotide | Somatostatin analog | ↓ hormone secretion | Carcinoid, VIPoma | — |
| Cholestyramine | Bile acid sequestrant | Binds bile acids | Bile acid diarrhea | Drug interactions (warfarin, digoxin) |
| Rifaximin | Non-absorbable antibiotic | Bacterial RNA pol inhibition | IBS-D, traveler's | Invasive/bloody diarrhea |
| Alosetron | 5-HT3 antagonist | ↓ colonic transit | Severe IBS-D (women only) | Men, ischemic colitis risk |
| Eluxadoline | μ/κ agonist + δ antagonist | Mixed opioid | IBS-D | No gallbladder |
| ORS | Hydration | SGLT1-mediated Na-glucose co-transport | All diarrhea | — |
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles of Internal Medicine 22E; Guyton & Hall Textbook of Medical Physiology; Katzung's Basic & Clinical Pharmacology 16E; Rosen's Emergency Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.