injection
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Here is a thorough overview of the four main parenteral injection routes.
Routes of Injection (Parenteral Administration)
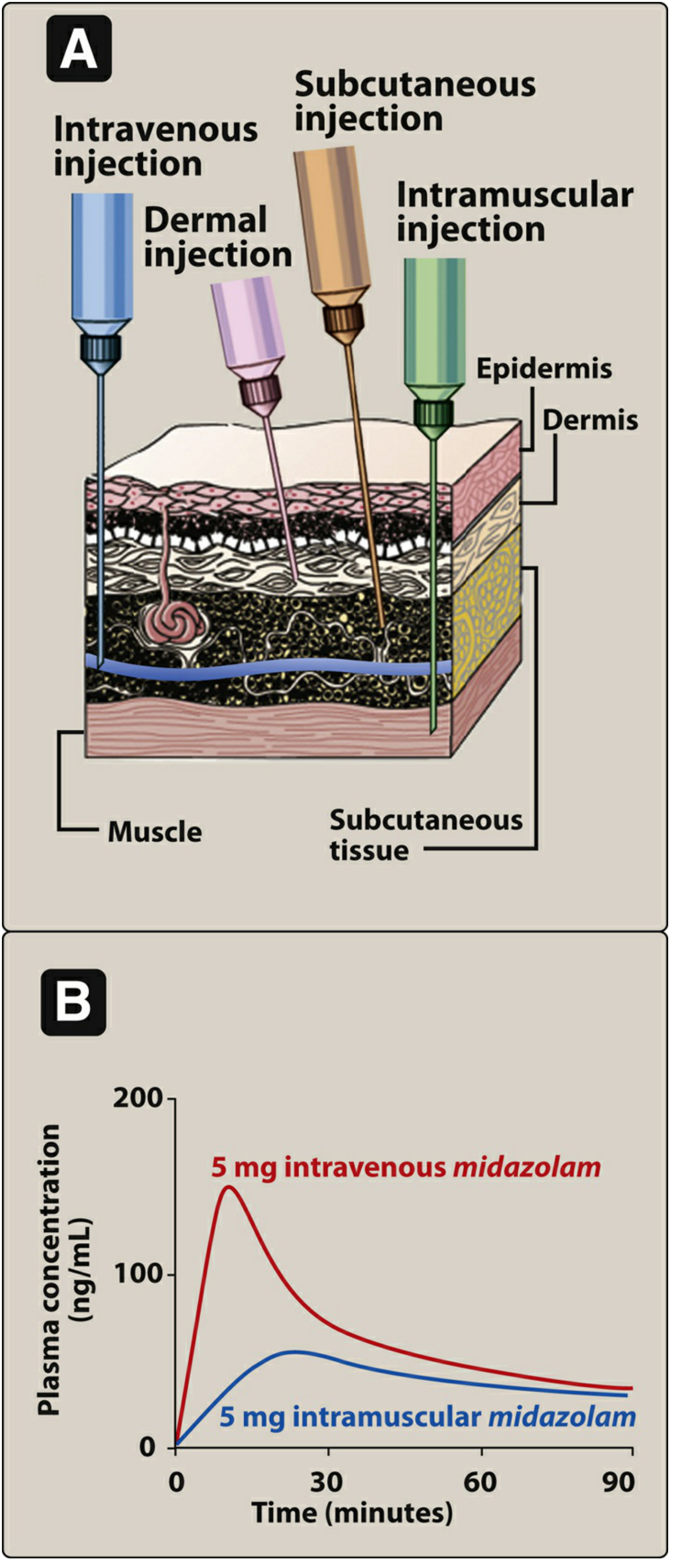
Fig. 1.3 - Lippincott Illustrated Reviews: Pharmacology. A: Cross-section showing depth of each injection route. B: Plasma concentration curves comparing IV vs. IM midazolam.
Why Use Parenteral Routes?
Parenteral routes bypass the GI tract entirely, which is useful when:
- A drug is poorly absorbed orally (e.g., heparin)
- A drug is unstable in the GI environment (e.g., insulin)
- The patient is unconscious or cannot swallow
- A rapid onset of action is needed
- Precise dose control is required
The trade-off: parenteral administration is irreversible, may cause pain, local tissue damage, and carries infection risk.
The Four Major Routes
1. Intravenous (IV)
- Depth: Directly into a vein (bypasses all tissue layers)
- Onset: Fastest of all routes - nearly immediate when given as a bolus
- Absorption: 100% bioavailability - no absorption step required
- Volume: Can accommodate large volumes
- Types:
- IV bolus - full dose delivered almost instantly
- IV infusion - drug delivered over time, giving lower peak concentrations and longer duration
- Examples: rocuronium, many antibiotics, emergency medications
- Risks: Hemolysis, thrombophlebitis, air embolism, infection
2. Intramuscular (IM)
- Depth: Into muscle tissue (below subcutaneous fat)
- Needle angle: 90 degrees
- Onset: Faster than SC, slower than IV
- Absorption: Via simple diffusion - rate depends on formulation
- Types of IM preparations:
- Aqueous solutions - absorbed rapidly
- Depot preparations - suspended in non-aqueous vehicles (e.g., polyethylene glycol, oil); the vehicle diffuses out, drug precipitates at the site, then dissolves slowly over days to weeks - ideal for long-acting formulations
- Common sites: Deltoid, vastus lateralis, ventrogluteal, dorsogluteal
- Max volume: ~3-5 mL in most sites
- Examples: vaccines, antipsychotics (depot), some antibiotics
3. Subcutaneous (SC)
- Depth: Into the subcutaneous (hypodermis) fat layer - below dermis, above muscle
- Needle angle: 45 degrees (can be 90° in obese patients with longer needles)
- Onset: Slower than IM due to lower vascularity of fat
- Absorption: Simple diffusion; provides slow, sustained, and constant drug release
- Advantages over IV: Minimizes risk of hemolysis or thrombosis
- Limitation: Should NOT be used for irritating drugs - risk of severe pain and necrosis
- Max volume: ~1-2 mL per site
- Examples: insulin, heparin, epinephrine auto-injectors
4. Intradermal (ID)
- Depth: Into the dermis (below epidermis, above subcutaneous tissue)
- Needle angle: 10-15 degrees (nearly flat to the skin)
- Onset: Slowest - minimal vascularity in dermis
- Primary uses:
- Allergy skin testing (diagnostic determination)
- Tuberculin (Mantoux) test (TB screening)
- Desensitization therapy
- Volume: Very small - typically 0.05-0.1 mL
- Expected result: A visible wheal (raised bleb) under the skin confirms correct placement
Quick Comparison Table
| Feature | IV | IM | SC | ID |
|---|---|---|---|---|
| Depth | Vein | Muscle | Fat | Dermis |
| Needle angle | 15-25° | 90° | 45-90° | 10-15° |
| Onset speed | Fastest | Fast | Moderate | Slowest |
| Bioavailability | 100% | High | High | Low |
| Max volume | Large | 3-5 mL | 1-2 mL | 0.1 mL |
| Typical uses | Emergency, large dose | Vaccines, depot drugs | Insulin, heparin | Allergy testing, TB test |
Speed of Absorption: IV > IM > SC > ID
The chart in the image illustrates this clearly - IV midazolam reaches a plasma concentration of ~150 ng/mL within ~15 minutes, while the same dose given IM peaks at roughly ~50 ng/mL over a longer, flatter curve.
- Lippincott Illustrated Reviews: Pharmacology, p. 25-26
This is a shared conversation. Sign in to Orris to start your own chat.