myocarditis. definition, epidemiology,etiology, pathogenesis, histopathology, clinical features, diagnosis, management,prognosis, complications,and differential diagnosis (table). along with images
Reading File
Finding Sources
Searching PubMed
myocarditis diagnosis management
Searching the Web
myocarditis histopathology clinical features diagnosis management 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. I have two excellent images (histopathology panel and cardiac MRI). Let me now compile the full, detailed answer.
Myocarditis
Definition
Myocarditis is an inflammatory process involving the myocardium caused by infectious agents, immune-mediated damage, or toxins, defined histologically by the presence of myocyte injury (degeneration or necrosis) and an inflammatory infiltrate not due to ischemia. It is important to distinguish myocarditis from conditions such as ischemic heart disease, where myocardial inflammation is secondary to another cause of injury. - Robbins & Kumar Basic Pathology, p. 375; Goldman-Cecil Medicine, p. 511
Epidemiology
The true incidence of myocarditis is difficult to estimate due to its heterogeneous presentation and frequent absence of biopsy confirmation. Key figures:
-
Incidence: Estimated at 10-22 per 100,000 people per year (approximately 1.5 million global cases in 2013)
-
Population prevalence: Ranges from 1 in 100,000 to 1 in 10,000 in general estimates
-
Postmortem studies: Myocarditis reported in up to 12% of young victims of sudden cardiac death; autopsy prevalence ranges from 0.11-0.53% of all-cause deaths and 2-42% of sudden cardiac death in young adults
-
Heart failure burden: Myocarditis accounts for 0.5-4% of all heart failure hospitalizations; it is 11 times more common than atherosclerotic MI in patients aged 18-29
-
Sex/Age: More common in younger adults and males; peak incidence in the third decade
-
Viral myocarditis is the most common form in the Western world, implicated in approximately one-third of cases; Coxsackievirus infection causes myocarditis in 3.5-5% of infected patients
-
Chagas disease (Trypanosoma cruzi) is the most common infective myocarditis worldwide, endemic in rural South and Central America
-
COVID-19/Vaccine: SARS-CoV-2 infection causes acute cardiac injury in 12-33% of hospitalized patients; post-mRNA vaccine myocarditis occurs rarely, especially in male adolescents after a second dose
-
Fuster and Hurst's The Heart, 15th Edition, p. 658; Goldman-Cecil Medicine, p. 510
Etiology
| Category | Agents |
|---|---|
| Viral (most common in West) | Coxsackievirus A & B, echovirus, adenovirus, parvovirus B19, HIV, influenza A/B, CMV, EBV, HHV-6, SARS-CoV-2, measles, mumps, rubella, VZV, dengue, hepatitis C, RSV |
| Protozoal | Trypanosoma cruzi (Chagas disease), Toxoplasma gondii |
| Bacterial | Corynebacterium diphtheriae, Borrelia burgdorferi (Lyme), Staphylococcus, Streptococcus, Neisseria meningitidis, Salmonella, Mycoplasma pneumoniae, Mycobacterium |
| Spirochetal | Treponema pallidum, Borrelia, Leptospira |
| Rickettsial | Coxiella burnetii, Rickettsia rickettsii, R. tsutsugamushi |
| Fungal | Aspergillus, Candida, Cryptococcus, Histoplasma, Coccidioides |
| Parasitic (Helminthic) | Trichinella spiralis (most common helminthic cause), Echinococcus granulosus, Taenia solium |
| Autoimmune/Immune-mediated | SLE, scleroderma, polymyositis/dermatomyositis, rheumatoid arthritis, sarcoidosis, Kawasaki disease, Wegener's granulomatosis, celiac disease, heart transplant rejection |
| Drug hypersensitivity | Penicillin, sulfonamides, tetracycline, methyldopa, tricyclic antidepressants, thiazides, indomethacin |
| Toxic | Anthracyclines, cocaine, amphetamines, cyclophosphamide, immune checkpoint inhibitors (pembrolizumab, nivolumab, ipilimumab, etc.), clozapine, ethanol |
| Physical agents | Electric shock, radiation, hyperpyrexia |
| Heavy metals | Copper, iron, lead |
| Idiopathic | Giant cell myocarditis, cardiac sarcoidosis |
- Goldman-Cecil Medicine, p. 510-511; Fuster and Hurst's The Heart, p. 659
Pathogenesis
Three-Phase Model of Viral Myocarditis
Phase 1 - Direct Viral Injury (Days 0-3):
Cardiotropic viruses (e.g., coxsackievirus) enter cardiomyocytes via receptor-mediated endocytosis. The viral genome causes direct cytopathic effects and may cleave dystrophin, destabilizing the cytoskeleton. This triggers immediate innate immune activation with recruitment of natural killer (NK) cells and macrophages, and release of proinflammatory cytokines (IL-1, TNF-alpha).
Phase 2 - Immune-Mediated Injury (Days 4-14):
Activation of CD4+ T lymphocytes promotes clonal expansion of B lymphocytes, producing anti-heart antibodies directed against contractile, structural, and mitochondrial proteins (e.g., myosin heavy chain). Virus-specific CD8+ cytotoxic T cells destroy virally infected myocytes. This autoimmune response can perpetuate myocardial damage even after viral clearance.
Phase 3 - Chronic/Remodeling Phase:
In genetically susceptible individuals, the autoimmune response persists, leading to long-term ventricular remodeling, progressive fibrosis, and ultimately dilated cardiomyopathy. Antiviral antibodies that cross-react with cardiac proteins sustain the process in the absence of ongoing infection.
Non-viral mechanisms:
-
Chagas disease: Direct myocardial parasitization by T. cruzi plus a mixed inflammatory infiltrate; chronic immune-mediated phase begins 10-20 years later
-
Hypersensitivity: Drug/immune reaction producing eosinophil-rich perivascular infiltrates
-
Giant cell myocarditis: Fused macrophages (multinucleate giant cells) causing widespread myocyte destruction; likely the fulminant end of the myocarditis spectrum
-
Checkpoint inhibitor myocarditis: T-cell dysregulation with PD-1/PD-L1 blockade leading to fatal lymphocytic infiltration
-
Goldman-Cecil Medicine, p. 511; Robbins Cotran & Kumar Pathologic Basis of Disease, p. 540; Fuster and Hurst's The Heart, p. 659
Histopathology
The histological classification follows the Dallas Criteria. Four patterns are recognized:
| Pattern | Description |
|---|---|
| Active myocarditis | Myocyte degeneration or necrosis + definite cellular infiltrate +/- fibrosis |
| Borderline myocarditis | Definite cellular infiltrate without myocardial cellular injury |
| Persistent myocarditis | Continued active myocarditis on repeated biopsy |
| Resolving/Resolved | Diminished/absent infiltrate with connective tissue healing |
Morphological Types
Grossly: Heart may be normal or dilated; in advanced stages, ventricular myocardium is flabby and mottled by pale foci or hemorrhagic lesions. Mural thrombi may be present.
Microscopically:
-
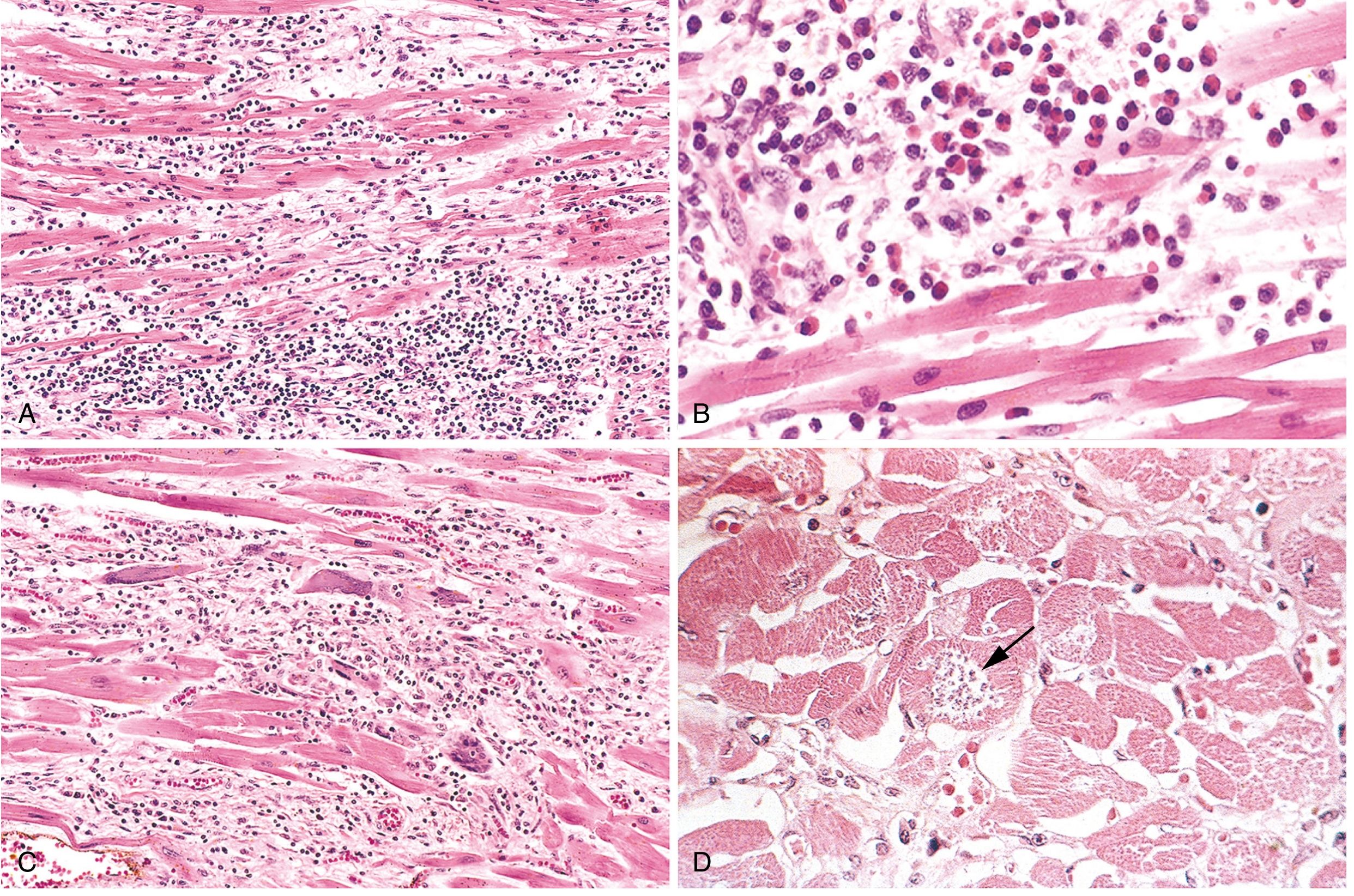
Lymphocytic (viral) myocarditis: Diffuse mononuclear (predominantly lymphocytic) interstitial inflammatory infiltrate associated with myocyte injury and edema (most common pattern; ~61.8% of cases). Inflammatory involvement is patchy - hence endomyocardial biopsy can be spuriously negative.
-
Hypersensitivity myocarditis: Perivascular and interstitial infiltrates composed of lymphocytes, macrophages, and a high proportion of eosinophils (~9.2% of cases).
-
Giant cell myocarditis: Widespread inflammatory infiltrate with multinucleate giant cells (fused macrophages) interspersed with lymphocytes, eosinophils, plasma cells, and macrophages; focal to extensive myocyte damage. Fulminant course with poor prognosis (~3.8% of cases).
-
Granulomatous myocarditis (Sarcoidosis): Non-caseating granulomas with lymphocytic infiltrate (~6.5%).
-
Chagas disease myocarditis: Parasitization of scattered myofibers by trypanosomes + mixed infiltrate of neutrophils, lymphocytes, macrophages, and occasional eosinophils.
If the patient survives the acute phase, lesions may either resolve completely (no residual change) or heal by progressive fibrosis, which forms the substrate for subsequent dilated cardiomyopathy and arrhythmia. - Robbins Cotran & Kumar Pathologic Basis of Disease, p. 540; Robbins Basic Pathology, p. 375
Clinical Features
The clinical presentation spans a wide spectrum:
Prodromal Symptoms (preceding days-weeks)
- Fever, myalgia, fatigue, arthralgia
- Upper respiratory symptoms (coryzal), gastroenteritis
- These reflect the underlying viral infection
Cardiac Presentations (5 recognized clinical syndromes per ESC)
| Syndrome | Features |
|---|---|
| 1. Acute chest pain (most common) | Sharp or pleuritic chest pain mimicking ACS or pericarditis; onset within 3 months |
| 2. New/worsening heart failure (acute) | Dyspnea, orthopnea, peripheral edema; LVEF impairment within 3 months |
| 3. Subacute/chronic heart failure (>3 months) | Gradual worsening dyspnea, fatigue, signs of biventricular failure |
| 4. Arrhythmia/syncope | Palpitations, unexplained arrhythmia (AF, VT, VF), syncope, or sudden cardiac death |
| 5. Cardiogenic shock | Fulminant myocarditis; acute cardiovascular collapse requiring inotropic/mechanical support |
Physical Examination Signs
- Tachycardia (sinus tachycardia most common)
- Muffled heart sounds, S3 or S4 gallop
- Pericardial friction rub (when myopericarditis coexists)
- Signs of heart failure: elevated JVP, pulmonary crackles, peripheral edema, hepatomegaly
- In fulminant cases: hypotension, weak peripheral pulses, cool/mottled extremities, narrow pulse pressure, elevated lactate
Key distinguishing feature from ACS: Myocarditis typically affects younger patients without cardiovascular risk factors; chest pain is often pleuritic; troponin elevation is present but coronary angiography shows normal arteries.
- Goldman-Cecil Medicine, p. 511; Fuster and Hurst's The Heart, p. 659-660
Diagnosis
Myocarditis requires a high index of clinical suspicion as it may mimic ACS, dilated cardiomyopathy, or arrhythmias.
1. Cardiac Biomarkers
- Troponin I/T: Elevated in acute myocarditis; reflects myocyte necrosis. Sensitivity is limited (troponin elevated in only 34-53% of biopsy-proven cases)
- CK-MB: May be elevated
- BNP/NT-proBNP: Elevated with heart failure; useful for monitoring
2. ECG
- Nonspecific ST-T wave changes most common (diffuse, not following a coronary territory)
- Sinus tachycardia
- AV block (I to III degree) - particularly with Lyme disease or sarcoidosis
- Bundle branch block
- Low QRS voltage
- Pathologic Q waves (can mimic MI)
- Ventricular tachycardia/fibrillation, SVT
3. Echocardiography
- May be normal in mild disease
- Global or regional wall motion abnormalities (not following coronary territory)
- Reduced LVEF (systolic dysfunction)
- Diastolic dysfunction
- Ventricular dilation
- Mural thrombus
- Pericardial effusion (myopericarditis)
- Preserved or hyperdynamic function in fulminant myocarditis (distinguishes it from acute DCM)
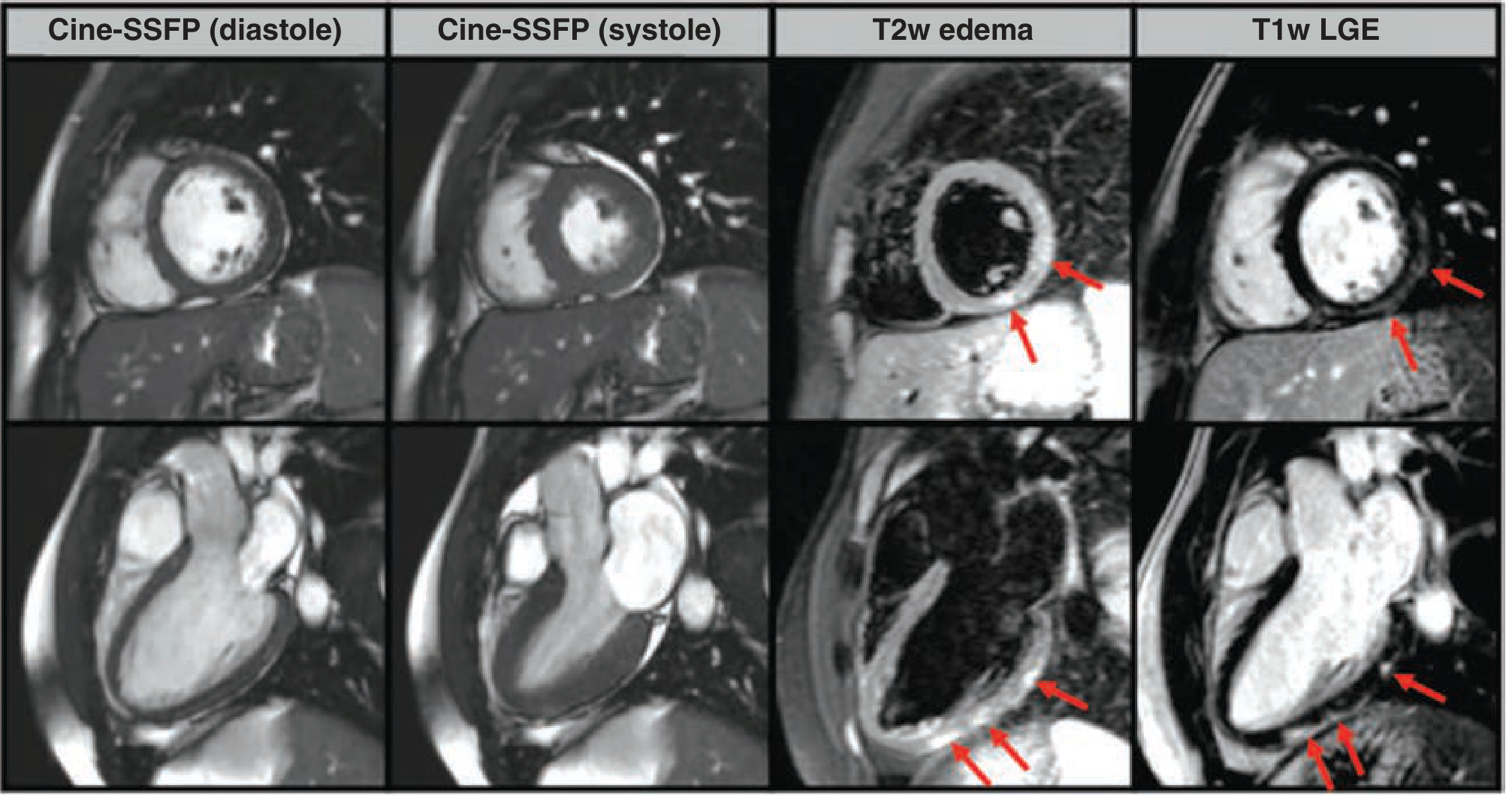
4. Cardiac MRI (CMR) - Gold Standard Non-Invasive Test
CMR is the most important non-invasive imaging modality. The Lake Louise Criteria (2018 updated) require ≥1 of the following:
| CMR Criterion | Interpretation |
|---|---|
| T2-weighted imaging (myocardial edema) | Focal/diffuse high T2 signal indicating inflammation |
| T1-weighted LGE (Late Gadolinium Enhancement) | Non-ischemic distribution (subepicardial or mid-myocardial, not subendocardial); typically in inferolateral wall |
| T1 mapping / ECV | Increased native T1 and extracellular volume fraction |
CMR also helps identify etiology by LGE location: parvovirus B19 → lateral wall; HHV-6 → septal. If initial CMR is normal but strong clinical suspicion exists, repeat CMR at 1-2 weeks is recommended.
5. Endomyocardial Biopsy (EMB)
The definitive diagnostic test but with limitations:
- Dallas criteria sensitivity is only 10-20% due to patchy inflammation (sampling error)
- Enhanced by: nested PCR / RT-PCR for viral genomes + immunohistochemistry for lymphocyte subtypes and cellular adhesion molecules
- Indications (ACC/AHA):
- Rapidly progressive heart failure not responding to standard therapy
- Unexplained cardiomyopathy requiring inotropic or mechanical support
- Mobitz type II or higher-degree heart block
- Ventricular tachycardia or failure to respond to treatment
- When biopsy may alter therapy (e.g., suspected giant cell, sarcoidosis, or autoimmune myocarditis)
6. Coronary Angiography
- Performed to exclude ACS when troponin is elevated and presentation mimics MI
- Normal coronary arteries in the setting of troponin elevation strongly suggests myocarditis
7. Laboratory
-
CBC (lymphocytosis in viral disease; eosinophilia in hypersensitivity myocarditis)
-
ESR, CRP (elevated in inflammation)
-
Viral serology (IgM/IgG) - limited clinical utility
-
ANA, anti-dsDNA, ENA, complement (C3/C4), rheumatoid factor - for autoimmune workup
-
Myositis immunoblot screen (if polymyositis suspected)
-
Goldman-Cecil Medicine, p. 511-512; Fuster and Hurst's The Heart, p. 661-665
Management
General Principles
Treatment strategy depends on the clinical presentation, severity, and underlying etiology.
1. Activity Restriction
- Mandatory rest during the acute phase (avoid competitive sports and strenuous exercise for at least 3-6 months, or until normalization of LV function, biomarkers, and ECG)
- NSAIDs are NOT indicated (harmful in animal models; unlike pericarditis)
2. Standard Heart Failure Therapy (for patients with LV dysfunction)
- ACE inhibitors / ARBs - neurohormonal blockade, reduce remodeling
- Beta-blockers - after hemodynamic stabilization (avoid in acute decompensated or fulminant phase due to negative inotropy)
- Mineralocorticoid receptor antagonists (spironolactone/eplerenone)
- Diuretics - for congestion (loop diuretics)
- SGLT2 inhibitors (dapagliflozin/empagliflozin) - supported by modern HFrEF guidelines
3. Antiarrhythmic Therapy
- Arrhythmias are managed as per standard guidelines
- ICD implantation: indicated for sustained VT/VF or primary prevention if LVEF <35% that persists despite optimal medical therapy for ≥3 months
- Temporary pacing: For high-degree AV block (e.g., Lyme myocarditis - usually self-limited)
4. Mechanical Circulatory Support (Fulminant Myocarditis)
- Early recognition of circulatory collapse is critical (sinus tachycardia, narrow pulse pressure, elevated lactate)
- ECMO (extracorporeal membrane oxygenation) - effective bridge to recovery
- IABP (intra-aortic balloon pump) or VAD (ventricular assist device) - bridge to recovery or transplantation
- Rate-control agents (beta-blockers, CCBs with negative inotropy) should be avoided in the acute phase
- Patients should be transferred to centers with capability for mechanical support, EMB, and advanced imaging
5. Immunosuppression (Etiology-Specific)
| Type of Myocarditis | Immunosuppressive Approach |
|---|---|
| Viral myocarditis / Unknown cause | Broad immunosuppression NOT beneficial; avoid |
| Autoimmune myocarditis (antibody-positive or with systemic autoimmune disease) | Steroids alone or with cyclosporine A or azathioprine; guided by HLA-DR upregulation on EMB |
| Giant cell myocarditis | High-dose corticosteroids + cyclosporine (improves survival, but often requires transplantation) |
| Cardiac sarcoidosis | Corticosteroids |
| Eosinophilic / NEM myocarditis | High-dose corticosteroids; anticoagulation for necrotizing form (due to microvascular thrombosis) |
| Immune checkpoint inhibitor myocarditis | IV corticosteroids promptly to prevent progression to fulminant myocarditis; discontinue the offending agent |
6. Immunomodulation and Antiviral Therapy
- Interferon-beta: Benefit in enteroviral/adenoviral myocarditis (improved LV function in small trials)
- IVIG: Limited benefit in adults; may be considered in unstable patients not responding to steroids; useful in pediatric populations
- Antivirals (acyclovir, ganciclovir, antiretrovirals): Effective for clearing peripheral virus but have not consistently improved myocardial function
- Statins: Small randomized trial showed improvement in LVEF
- Colchicine: Useful adjunct when myopericarditis is present
7. Anticoagulation
- Consider in patients with mural thrombus, AF, severely reduced LVEF (<35%), or necrotizing eosinophilic myocarditis
8. Cardiac Transplantation
-
Reserved for patients with refractory heart failure or giant cell myocarditis unresponsive to immunosuppression
-
Fuster and Hurst's The Heart, 15th Edition, p. 664-666; Goldman-Cecil Medicine, p. 512
Prognosis
The natural history is highly variable and depends on the clinical presentation, LVEF, and underlying etiology:
- Overall: ~50% of acute myocarditis cases recover completely; ~25% experience a slow decline in LV function; ~25% rapidly progress to severe LV dysfunction, transplantation, or death
- Mild cases (normal or near-normal LVEF): Excellent prognosis with complete recovery
- Fulminant myocarditis (paradoxically): Despite severe initial presentation, has a better chance of full recovery in adults than non-fulminant acute myocarditis (due to reversible hemodynamic insult rather than chronic fibrosis)
- Giant cell myocarditis: Poor prognosis; median transplant-free survival is approximately 5.5 months without immunosuppression
- Necrotizing eosinophilic myocarditis (NEM): Markedly poor prognosis
- Chagas disease: ~10% die during acute phase; 20-30% develop cardiac disease over years-decades
Independent Predictors of Poor Prognosis
-
Initial presentation with biventricular failure
-
Sustained ventricular arrhythmia
-
Low cardiac output state
-
LVEF < 50% at presentation
-
LGE extent on CMR (fibrosis burden)
-
HIV-associated myocarditis (strong predictor of poor prognosis)
-
Fuster and Hurst's The Heart, 15th Edition, p. 658; Goldman-Cecil Medicine
Complications
| Complication | Notes |
|---|---|
| Dilated cardiomyopathy (DCM) | Most common long-term complication; fibrosis after healing leads to progressive LV dilation and dysfunction |
| Chronic heart failure | Left- or biventricular failure; may require transplant listing |
| Arrhythmias | PVCs, NSVT, sustained VT/VF, AF; risk of sudden cardiac death |
| AV conduction block | Lyme disease (self-limited); giant cell/sarcoid (may require permanent pacemaker) |
| Sudden cardiac death | Accounts for 2-42% of sudden death in young adults at autopsy |
| Cardiogenic shock / Fulminant myocarditis | Requires ECMO/VAD support |
| Mural thrombus and systemic embolism | Due to ventricular dilation and reduced flow |
| Pericardial effusion / Cardiac tamponade | When myopericarditis is present |
| Myocarditis-related arrhythmogenic cardiomyopathy | Inflammatory phase of ARVC/fibrotic substrate for reentrant VT |
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Acute MI (ACS) | Subendocardial LGE on CMR following a coronary territory; culprit lesion on coronary angiography; older patients with cardiovascular risk factors; troponin rise-and-fall kinetics |
| Dilated Cardiomyopathy (idiopathic) | Gradual onset without preceding viral illness; no acute inflammation on CMR; EMB may show fibrosis but no active infiltrate |
| Pericarditis | Chest pain is predominantly positional/pleuritic; pericardial friction rub; diffuse saddle-shaped ST elevation; normal LVEF; no myocyte necrosis; responds to NSAIDs/colchicine |
| Arrhythmogenic Cardiomyopathy (ARVC) | Fatty/fibrous replacement on CMR; epsilon wave on ECG; RV-dominant disease; desmosomal gene mutation; Task force criteria |
| Stress Cardiomyopathy (Takotsubo) | Post-emotional/physical stress; apical ballooning on echo; predominantly post-menopausal women; rapid normalization; no inflammatory infiltrate on CMR |
| Cardiac Sarcoidosis | Non-caseating granulomas on EMB; systemic sarcoidosis features; patchy LGE (basal, septal); thallium/FDG-PET abnormalities; responds to steroids |
| Cardiac Amyloidosis | Diffuse subendocardial LGE; low voltage on ECG with increased wall thickness ("pseudo-LVH"); restrictive physiology; congo red staining on biopsy |
| Hypertrophic Cardiomyopathy (HCM) | LV hypertrophy (often asymmetric septal); LVOT obstruction; SAM of mitral valve; family history/genetic mutation; no acute inflammation |
| Rheumatic Carditis | Post-streptococcal (ASO titer); Jones criteria; valvular involvement (mitral regurgitation most common); Sydenham chorea; subcutaneous nodules |
| Hypertensive Heart Disease | Long-standing hypertension history; concentric LV hypertrophy; LGE absent or minimal |
| Drug-induced cardiomyopathy | Dose-dependent (anthracyclines); history of chemotherapy; no inflammatory infiltrate |
| Endocrine cardiomyopathy (e.g., thyrotoxicosis) | Thyroid function tests; hyperdynamic state; AF; diffuse ventricular dysfunction |
Summary
Myocarditis is a heterogeneous inflammatory disease of the myocardium that ranges from subclinical to life-threatening. Viral etiology dominates in the Western world; Chagas disease globally. The pathogenesis involves three phases: direct viral injury, immune-mediated damage, and chronic remodeling. Histopathology reveals four patterns (lymphocytic, hypersensitivity, giant cell, granulomatous), classified by Dallas criteria. CMR with Lake Louise criteria is the gold standard non-invasive diagnostic tool. Management is largely supportive (HF therapy, rest, arrhythmia management) with specific immunosuppression for autoimmune, giant cell, eosinophilic, and checkpoint inhibitor subtypes. Prognosis varies - most mild cases recover fully, but giant cell and necrotizing eosinophilic subtypes carry poor outcomes. The main long-term complication is dilated cardiomyopathy.
Sources:
- Robbins Cotran & Kumar Pathologic Basis of Disease, 10th Edition
- Robbins & Kumar Basic Pathology, 10th Edition
- Fuster and Hurst's The Heart, 15th Edition
- Goldman-Cecil Medicine, International Edition
- Braunwald's Heart Disease, 12th Edition
- 2024 ACC Expert Consensus Decision Pathway on Myocarditis
- 2025 ESC Guidelines for the Management of Myocarditis and Pericarditis
This is a shared conversation. Sign in to Orris to start your own chat.