explain 10 common heart diseases with ecg changes and ecg images of those diseases
myocardial infarction STEMI ECG ST elevation changes
atrial fibrillation ECG electrocardiogram
heart block complete AV block third degree ECG
ventricular tachycardia VT ECG wide complex tachycardia
left ventricular hypertrophy ECG high voltage criteria
pericarditis ECG saddle-shaped ST elevation diffuse
Wolff-Parkinson-White WPW syndrome ECG delta wave pre-excitation
right bundle branch block RBBB ECG RSR pattern V1
dilated cardiomyopathy heart failure ECG changes
pulmonary embolism PE ECG S1Q3T3 right heart strain
10 Common Heart Diseases: ECG Changes & Images
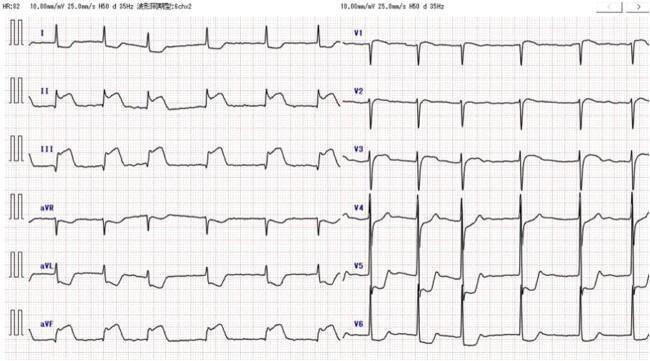
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Overview
ECG Changes
| Feature | Description |
|---|---|
| ST elevation | Convex ("tombstone") ST elevation ≥1 mm in ≥2 contiguous leads |
| Reciprocal ST depression | In leads facing the opposite wall |
| Hyperacute T-waves | Tall, peaked T-waves in early phase |
| Pathological Q-waves | Develop within hours (>40 ms wide, >25% of R-wave amplitude) |
| T-wave inversion | Late/evolving change |
Localization
- Anterior (LAD): ST ↑ in V1–V4
- Inferior (RCA): ST ↑ in II, III, aVF
- Lateral (LCx): ST ↑ in I, aVL, V5–V6
ECG Images
2. 🫀 Atrial Fibrillation (AF)
Overview
ECG Changes
| Feature | Description |
|---|---|
| No P-waves | Replaced by fine irregular fibrillatory (f) waves |
| Irregularly irregular rhythm | No two R-R intervals are the same |
| Narrow QRS | Unless aberrant conduction or bundle branch block coexists |
| Variable ventricular rate | Typically 100–160 bpm in uncontrolled AF |
ECG Image

3. 🫀 Complete (Third-Degree) Heart Block
Overview
ECG Changes
| Feature | Description |
|---|---|
| AV dissociation | P-waves march through QRS complexes with no fixed PR interval |
| Regular P-P intervals | Normal atrial rate (60–100 bpm) |
| Slow escape rhythm | Ventricular rate 20–40 bpm (junctional) or 30–40 bpm (ventricular) |
| Wide QRS | >120 ms if ventricular escape; narrow if junctional escape |
ECG Image
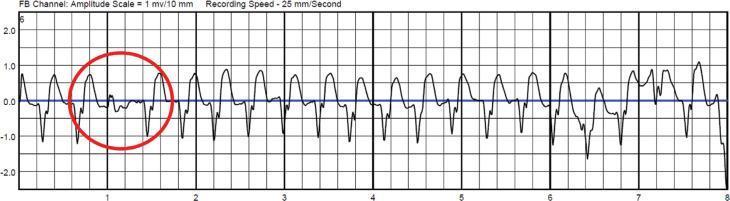
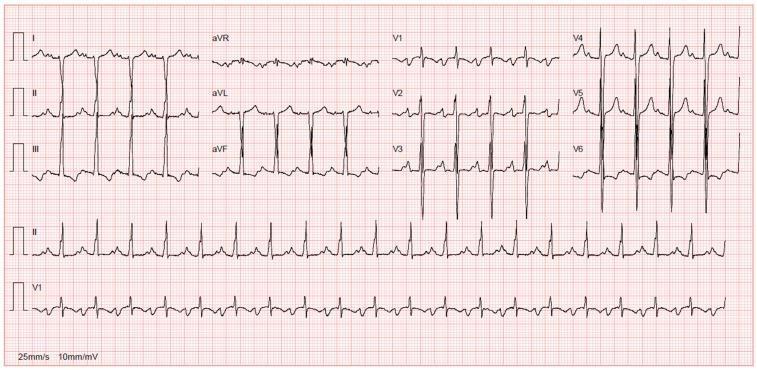
4. 🫀 Ventricular Tachycardia (VT)
Overview
ECG Changes
| Feature | Description |
|---|---|
| Wide QRS | >120 ms (typically >140 ms) |
| Regular, rapid rhythm | 100–250 bpm |
| AV dissociation | P-waves independent of QRS (pathognomonic) |
| Fusion/capture beats | Intermittent narrow QRS = sinus capture (confirms VT) |
| Concordance | All precordial leads positive or all negative |
| No preceding P-waves | Ectopic ventricular origin |
ECG Image
5. 🫀 Acute Pericarditis
Overview
ECG Changes (4 Stages)
| Stage | Timing | ECG Feature |
|---|---|---|
| Stage 1 | Hours–days | Diffuse concave ("saddle-shaped") ST elevation + PR depression |
| Stage 2 | Days 1–3 | ST normalizes, PR depression persists |
| Stage 3 | Days 3–7 | Diffuse T-wave inversion |
| Stage 4 | Weeks | ECG normalizes |
- ST elevation is diffuse (not localized to one territory)
- PR segment depression in II, V4–V6 (and PR elevation in aVR)
- No reciprocal ST depression
- Spodick's sign: downsloping TP segment
ECG Image

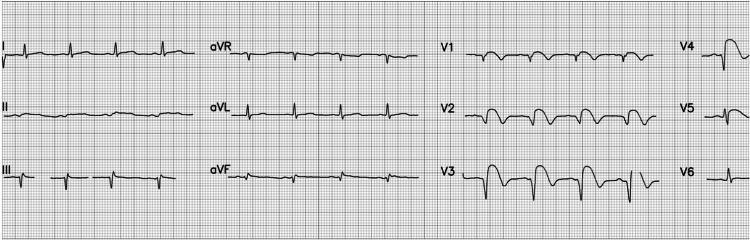
6. 🫀 Left Ventricular Hypertrophy (LVH)
Overview
ECG Changes
| Feature | Description |
|---|---|
| Sokolow-Lyon criteria | S in V1 + R in V5 or V6 ≥35 mm |
| Cornell criteria | R in aVL + S in V3 >28 mm (men) or >20 mm (women) |
| Left axis deviation | QRS axis between −30° and −90° |
| Strain pattern | ST depression + T-wave inversion in I, aVL, V5–V6 |
| Repolarization changes | Asymmetric T-wave inversion in lateral leads |
ECG Image
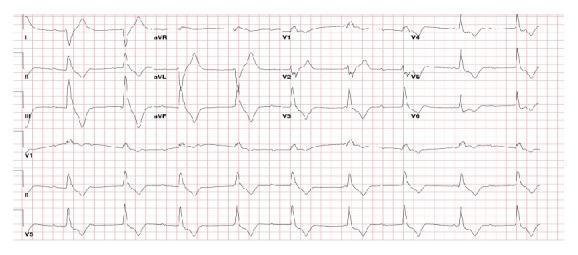
7. 🫀 Wolff-Parkinson-White (WPW) Syndrome
Overview
ECG Changes
| Feature | Description |
|---|---|
| Short PR interval | <120 ms (bypasses AV nodal delay) |
| Delta wave | Slurred upstroke at beginning of QRS |
| Wide QRS | >120 ms (fusion of normal conduction + pre-excitation) |
| Secondary ST-T changes | Discordant T-waves (repolarization abnormality) |
| Pseudo-infarct pattern | Negative delta waves in inferior leads can mimic Q-waves |
ECG Image

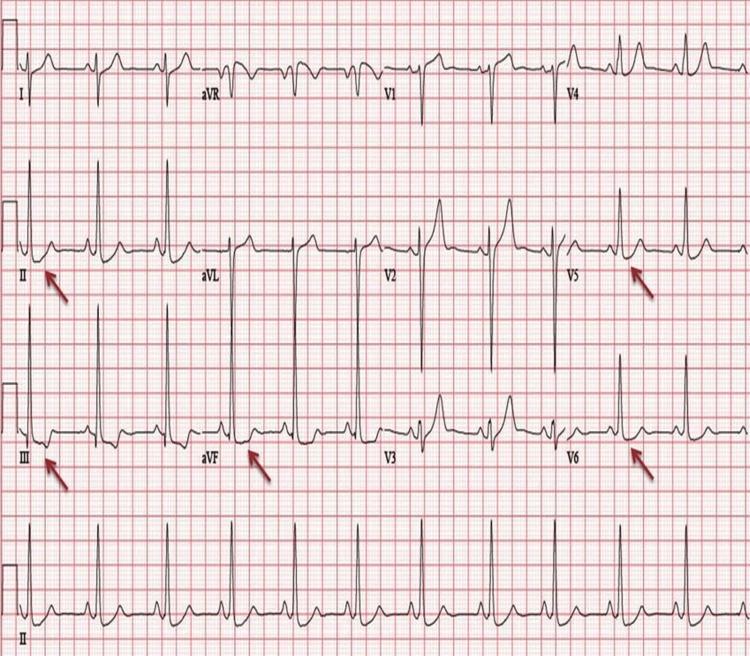
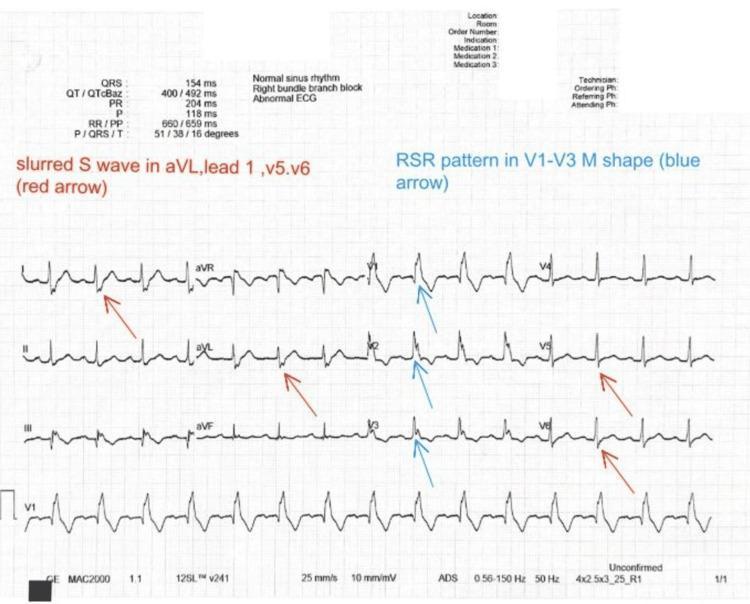
8. 🫀 Right Bundle Branch Block (RBBB)
Overview
ECG Changes
| Feature | Description |
|---|---|
| Wide QRS | >120 ms (complete RBBB); 100–119 ms (incomplete) |
| RSR' pattern in V1 | "Rabbit-ear" or "M-shaped" morphology |
| Slurred S-waves | Wide S in leads I, V5, V6 ("lateral leads") |
| T-wave inversion | In V1–V3 (secondary repolarization change) |
| ST depression | V1–V3 (secondary change, not ischemia) |
ECG Image
9. 🫀 Pulmonary Embolism (PE)
Overview
ECG Changes
| Feature | Description |
|---|---|
| Sinus tachycardia | Most common finding (70%+) |
| S1Q3T3 pattern | Deep S in lead I, Q-wave in III, T-inversion in III |
| New RBBB | Acute right ventricular strain/dilatation |
| Right axis deviation | From RV pressure overload |
| T-wave inversions V1–V4 | Right ventricular strain pattern |
| P-pulmonale | Tall, peaked P-waves (right atrial enlargement) |
ECG Image

10. 🫀 Dilated Cardiomyopathy (DCM)
Overview
ECG Changes
| Feature | Description |
|---|---|
| Left bundle branch block (LBBB) | Wide QRS >120 ms, broad notched R in V6, no septal Q in I/aVL/V6 |
| Atrial fibrillation | Common, from atrial dilatation |
| PVCs / ventricular ectopics | Common, risk of VT/VF |
| Left axis deviation | From ventricular remodeling |
| Prolonged PR | First-degree AV block |
| Nonspecific ST-T changes | Diffuse repolarization abnormalities |
| Low voltage | If pericardial effusion coexists |
ECG Image
Quick-Reference Summary Table
| Disease | Key ECG Finding | Distinguishing Feature |
|---|---|---|
| STEMI | ST elevation in contiguous leads | Reciprocal changes, territory-based |
| Atrial Fibrillation | No P-waves, irregular rhythm | Irregularly irregular R-R |
| Complete Heart Block | AV dissociation | P and QRS march independently |
| Ventricular Tachycardia | Wide complex tachycardia | Capture/fusion beats, concordance |
| Pericarditis | Diffuse saddle-shaped ST elevation | PR depression, all leads except aVR |
| LVH | High-voltage QRS | Strain pattern in I, aVL, V5–V6 |
| WPW | Short PR + delta wave | Pre-excitation; wide QRS |
| RBBB | RSR' in V1, slurred S in V6 | Secondary T-wave changes V1–V3 |
| Pulmonary Embolism | Sinus tachycardia + S1Q3T3 | New RBBB, right axis deviation |
| Dilated Cardiomyopathy | LBBB, AF, diffuse ST-T changes | Broad notched R in V6, no septal Q |
Clinical Note: ECG findings must always be interpreted in clinical context. Many of these patterns overlap, and serial ECGs are often essential for diagnosis. Any hemodynamically unstable patient with ECG changes requires urgent cardiology review.
common chest xray pathologies with images and findings and how to read it ?
normal chest X-ray PA view anatomy landmarks
pneumothorax chest X-ray absent lung markings visceral pleural line
pleural effusion chest X-ray blunting costophrenic angle meniscus sign
lobar pneumonia consolidation chest X-ray air bronchogram
pulmonary edema chest X-ray bat wing perihilar haziness Kerley B lines
cardiomegaly enlarged heart chest X-ray cardiothoracic ratio
pulmonary tuberculosis cavitation upper lobe chest X-ray
ARDS acute respiratory distress syndrome bilateral white out chest X-ray
lung mass solitary pulmonary nodule chest X-ray
tension pneumothorax mediastinal shift tracheal deviation chest X-ray